
Wed, Jul 29, 2026
[Archive]
Volume 19, Issue 2 (2026)
J Med Edu Dev 2026, 19(2): 69-79 |
Back to browse issues page

Ethics code: KNSMIMS/ IEC/2025/74
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Rajani M, Sedani S. Comparative evaluation of objective structured viva voce versus traditional viva voce in assessment of student performance in microbiology. J Med Edu Dev 2026; 19 (2) :69-79
URL: http://edujournal.zums.ac.ir/article-1-2628-en.html
URL: http://edujournal.zums.ac.ir/article-1-2628-en.html

1- Department of Microbiology, Dr. KNS Memorial Institute of Medical Sciences, Barabanki, Uttar Pradesh, India ²Datta Meghe Institute of Higher Education and Research, Wardha, Maharashtra, India , drmonikarajani@gmail.com
2- Department of Microbiology, Dr. KNS Memorial Institute of Medical Sciences, Barabanki, Uttar Pradesh, India ²Datta Meghe Institute of Higher Education and Research, Wardha, Maharashtra, India
2- Department of Microbiology, Dr. KNS Memorial Institute of Medical Sciences, Barabanki, Uttar Pradesh, India ²Datta Meghe Institute of Higher Education and Research, Wardha, Maharashtra, India
Full-Text [PDF 727 kb]
(194 Downloads)
| Abstract (HTML) (383 Views)
Full-Text: (96 Views)
Abstract
Background & Objective: Inconsistent evaluation with traditional viva voce undermines the reliability and validity of assessments. Objective Structured Viva Voce (OSVV) with standardized scoring ensures objective evaluation, less examiner bias, and subjectivity. This study aimed to compare the effectiveness of OSVV and traditional viva voce in assessing student performance.
Materials & Methods: This educational interventional study was carried out on 133 second-year Bachelor of Medicine and Bachelor of Surgery (MBBS) students. A pre-validated collection of viva cards, targeting recall and higher-order cognitive domains, was developed based on the Attitude, Ethics, and Communication (AETCOM) Module. The students were evaluated through two types of viva voce examinations using a crossover study design. Evaluation was done by comparing student scores using both methods, followed by a feedback questionnaire.
Results: There was a statistically significant difference (p < 0.001) in student scores, with higher average marks with the OSVV versus the traditional approach. The comparatively lower inter-batch variation in OSVV (F-value = 0.31, p-value = 0.734) highlights its greater consistency and unbiasedness in evaluation across different batches. Among the students, the overall satisfaction index was 59.53, suggesting a generally positive perception of OSVV. Faculty feedback indicated that OSVV can be used as a superior alternative to the traditional approach as an assessment tool.
Conclusion: The study highlights OSVV as a superior alternative to traditional viva, reducing bias and enhancing fairness. It demonstrated significant improvement in student performance and consistency. OSVV represents a progressive reform ensuring fairness, transparency, and competency in MBBS graduate assessments.
Introduction
Viva voce complements theory and practical examinations. It helps in the comprehensive assessment of students' capabilities in examinations. It involves face-to-face interaction where the examiner probes the student’s understanding, reasoning, and critical thinking skills. Viva voce aims to assess discernment and the student's ability to comprehend knowledge, think quickly, and demonstrate eloquent professional etiquette [1]. Our institute conducts undergraduate MBBS assessments using the traditional viva-voce, typically during the later phase of the practical examination. However, it is frequently observed that this conventional method lacks consistency, as the outcomes are often influenced by the examiner’s mood and personal biases. Conventional viva voce is traditionally conducted by different examiners depending on their availability on the day of the examination, thereby introducing additional variability in assessment. Examiner judgment may be affected by personal preferences, variations in their method of questioning, emphasis on specific content areas, and several other confounding factors.
Despite adequate knowledge, students may be unable to respond effectively due to limited recall time or intimidating behavior during the viva voce, resulting in heightened stress. Examiners may experience fatigue, lack of interest, or time constraints, which can influence the conduct of the assessment. The lack of standardisation results in considerable variability in question content and difficulty among examiners, frequently leading to incomplete coverage of the syllabus. Consequently, such variability may compromise the fairness of student assessment.
The examination largely emphasizes recall of knowledge, often restricted to core topics preferred by individual examiners. Owing to the lack of a structured format, higher-order cognitive domains such as application, reasoning, problem-solving, analysis, and synthesis are not adequately assessed. Additionally, domains such as ethics and professional attitude receive little attention in the traditional viva. Essential microbiology competencies, including respectful handling of patient samples and maintenance of patient confidentiality, are seldom evaluated. To achieve these objectives, we need an assessment tool that demonstrates validity, reliability, feasibility, and a positive professional educational impact. In an effort to address existing discrepancies in assessment practices, we sought to make the process more viable, uniform, transparent, and effective by implementing a structured viva voce examination. As assessment is a core component of Competency-Based Medical Education (CBME), the adoption of innovative assessment methods such as the OSVV in our institute is expected to overcome the limitations associated with conventional assessment approaches. Thus, this study was designed to study whether OSVV would be a better tool in assessing the performance of the students during examinations.
OSVV provides a uniform, preformed assessment framework with questionnaires and standardised scoring, ensuring objective evaluation consistently [2]. This reduces variability and minimises examiner bias and subjectivity, significantly improving the reliability and validity of assessments. OSVV helps assess specific competencies by framing questions with learning objectives and desired outcomes [3]. Students’ logical medical analysis, problem-solving capacities, and communication skills are evaluated [3]. OSVV provides more constructive appraisals to the students about their performance. Increasing evidence indicates that OSVV can assess students’ achievements in course outcomes beyond simple knowledge recall, encompassing problem-solving, critical thinking, decision-making, professionalism, ethics, and interpersonal skills [4, 5]. There is a paucity of data on the assessment of higher-order cognitive and affective domains through structured viva in the subject of microbiology. Some comparative studies conducted in the evaluation of student performance through traditional and structured viva only address the questions testing the simple recall of knowledge. Studies assessing the affective domain are also limited. 17 We included specific scenario-based questions integrated into the structured viva to probe a student's ethical judgment and professional attitudes, which fall under the higher levels of the affective domain. Thus, this study was designed to investigate whether OSVV would be a more effective tool in assessing student performance and to evaluate higher domains of learning through a structured viva in microbiology.
Materials & Methods
Design and setting(s)
This was an educational interventional study. This study was conducted at the Department of Microbiology, Dr. KNS Memorial Institute of Medical Sciences, over a duration of six months. The study duration was from January 2025 to June 2025.
Participants and sampling
A total of 133 second-year MBBS students were enrolled in the study. Convenience sampling was used: all second-year MBBS students willing to take part were included, while those not willing were excluded. Approval was obtained from the Institutional Ethics Committee. Students were oriented to the OSVV through structured demonstrations.
Tools/Instruments
The OSVV questions, checklists, and feedback questionnaires were created by subject experts and reviewed by senior faculty and medical education experts before use. Mock OSVV sessions were run to assess clarity, feasibility, time allocation, and scoring patterns. Content validity was ensured by mapping questions to prescribed MBBS microbiology competencies across knowledge, skills, and attitudinal domains. Reliability was addressed through standardised checklists, uniform marking schemes, and examiner training. Standard setting was based on institutional and CBME guidelines, with the passing criterion set at 50% of the cumulative marks in practical and viva examinations. A pre-validated set of viva cards addressing recall and higher-order domains based on the Attitude, Ethics, and Communication Module (AETCOM) was prepared. AETCOM is a mandatory longitudinal module introduced by the National Medical Commission, India, for MBBS students. This module is designed to mentor competent, ethical, empathetic, and communicative MBBS students. Questions were based on core competencies as per the NMC. CBME curriculum topics include general microbiology, bacteriology, serology, parasitology, and applied microbiology. Questions covered cognitive domains from knowledge recall to application and higher-order reasoning (Table 1). The questions also addressed the AETCOM components in Microbiology, thus allowing the assessment of various soft skills like respect for and confidentiality of patients’ samples and reports.
Table 1. Structure, domains, and mark distribution of the OSVV in Microbiology

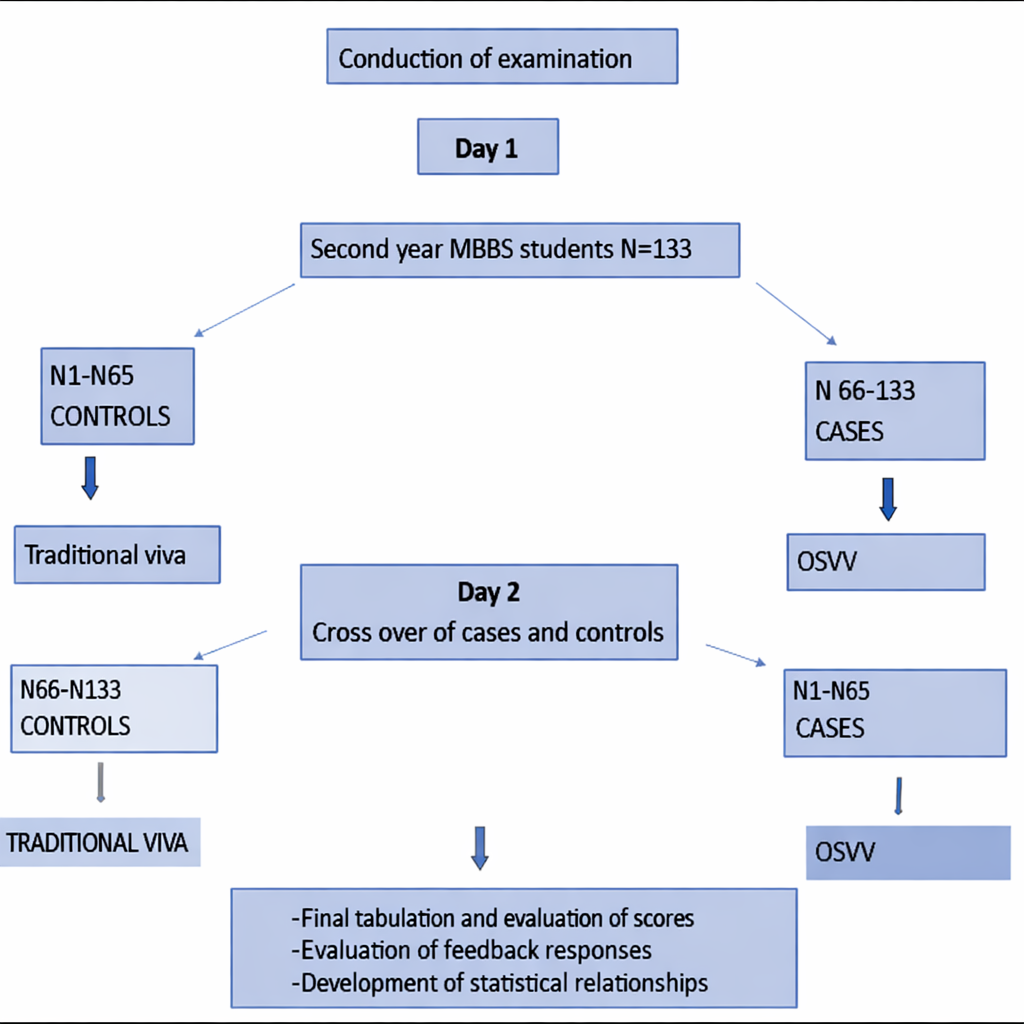
Figure 1. Flow diagram of the study methodology showing the crossover design and group allocation
Data collection methods
The students were assessed using two different formats of viva-voce examination in a crossover study design, where each student took part in both assessment formats at different times, thereby serving as their own control. Since students underwent assessment through a crossover design, all participants were exposed to both methods on separate occasions, which reduced inter-individual variability and improved comparability. Each student received five viva cards (totaling 25 marks) addressing different learning domains with varying difficulty levels, which included core microbiology topics (Figure 2). Students were given 8-10 minutes to answer the viva cards. Each student was assessed at a single station by a single examiner based on the five viva cards.
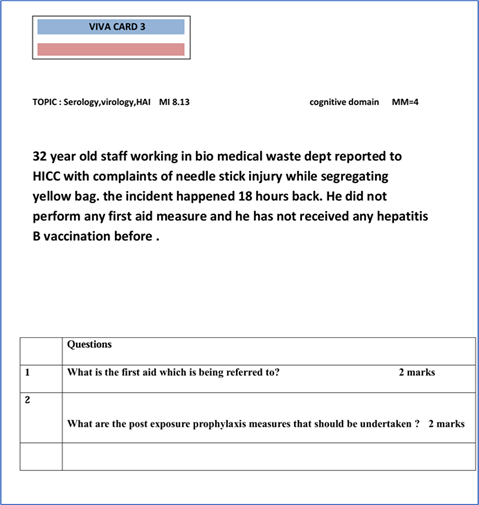
Table 2. Comparison of grand viva marks between the two assessment methods

Note: Unpaired t-test was used to compare the mean scores between the OSVV and traditional viva voce assessment methods.
Abbreviations: OSVV, objective structured viva voce; SD, standard deviation.
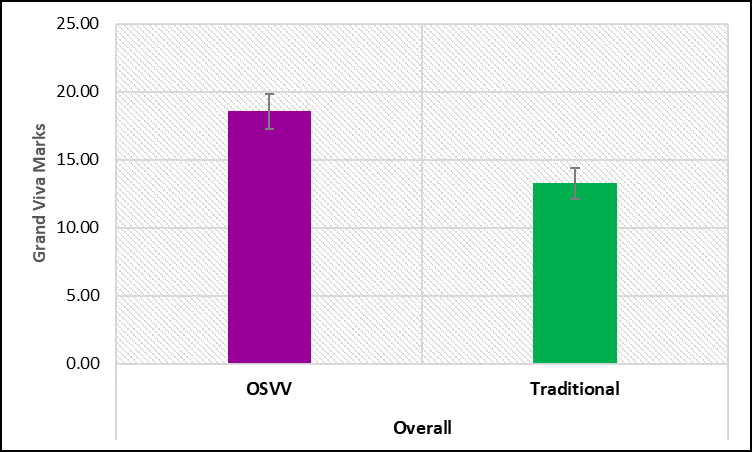
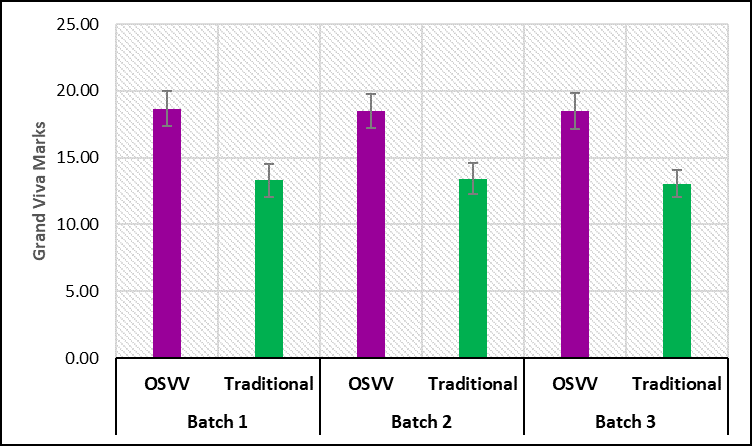
Figure 4: Comparison of batch-wise grand viva marks between two assessment methods
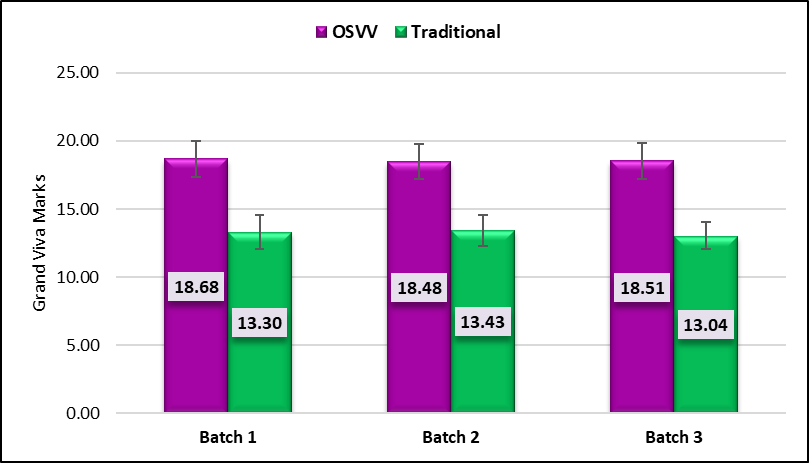
Figure 5: Comparison of grand viva marks among the batches for the two assessment methods
For the OSVV method, batch 1 scored a mean of 18.68 ± 1.31, batch 2 scored 18.48 ± 1.27, and batch 3 scored 18.51 ± 1.34, with an overall F-value of 0.31 and p = 0.734, indicating uniformity across batches. Similarly, for the traditional method, batch 1 had a mean of 13.30 ± 1.23, batch 2 scored 13.43 ± 1.15, and batch 3 scored 13.04 ± 1.00, with an F-value of 1.35 and p = 0.263, again showing no significant batch-wise variation. This suggests that both OSVV and traditional assessment methods provided consistent results across all three batches. The satisfaction index for various aspects of the OSVV reflected moderate levels of student satisfaction (Figure 6). The highest satisfaction was seen for the statement “Adequate time provided” with an index of 66.17, followed by “I realised what I know from the entire syllabus” (62.78) and “Questions are easy to understand as they are to the point and precise” (61.28). Other items, such as “All topics are covered” (60.15) and “OSVV is well organised” (63.16), also showed favourable responses. The lowest satisfaction was noted for the negatively worded item “OSVV is tiresome, confusing.” The item “OSVV will enhance my performance” had a satisfaction index of 59.21. The overall satisfaction index for OSVV was 59.53. The findings imply that while the OSVV is an acceptable and feasible assessment method, refinements in implementation and orientation may improve its overall acceptance and effectiveness. The faculty feedback on OSVV was collected item-wise to understand their perceptions regarding various aspects of the evaluation method (Figure 7). For the item “Examiner bias and luck factor is minimised in OSVV,” responses were balanced, with 3 faculty members agreeing and 3 strongly agreeing, indicating a consensus that OSVV improves objectivity. Regarding the “Uniformity of difficulty level ensured in the OSVV procedure,” 2 faculty members stayed neutral, while 4 agreed, suggesting a general positive perception with some reservations. When asked whether OSVV is more labour-intensive for faculty due to groundwork, all 6 faculty members agreed, reflecting a unanimous view of increased faculty effort in preparation. For the statement “OSVV lacks the flexibility factor,” opinions were mixed, with 3 neutral and 3 agreeing, indicating moderate concern over adaptability. On whether “OSVV procedure entailed minimal faculty-student interactivity,” 4 agreed and 2 strongly agreed, highlighting a perceived reduction in engagement.
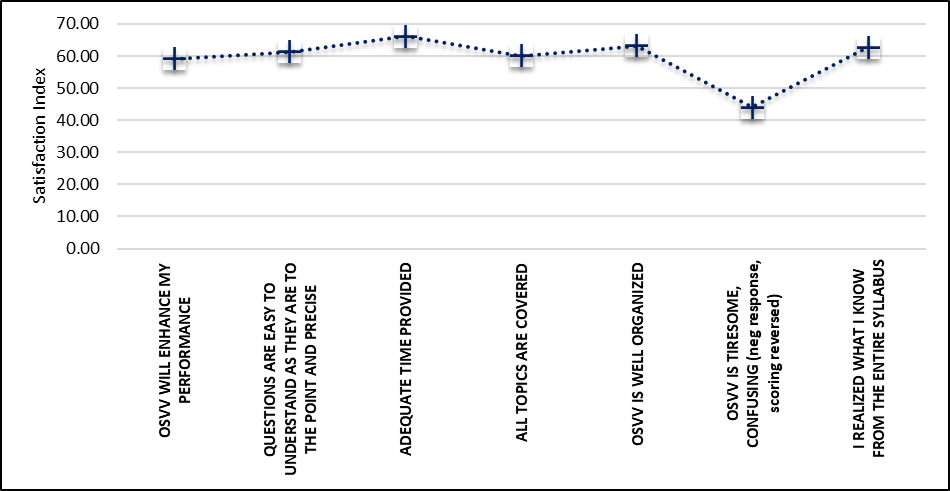
Figure 6. Item-wise and overall satisfaction index of the OSVV method
Discussion
Assessment is an integral part of the curriculum, which plays a vital role in the learning process. Assessment has a direct influence on learning, as it determines whether a learner has attained the required level of competency. Over time, assessment has evolved into a dynamic process, becoming more robust, reliable, valid, fair, and grounded in evidence-based practices [6]. An oral examination fosters professional interaction between the assessor and the student, aiming to evaluate core competencies, particularly higher-order cognitive skills such as analysis, evaluation, and synthesis. Overall, the difference in average marks obtained by the students in the OSVV method and the conventional method was statistically significant (p <0.001). The students gained higher marks in OSVV, indicating it to be significantly more effective than the traditional method in student performance evaluation. Across all batches, OSVV consistently outperformed the traditional assessment method with statistically significant differences.
Rathod et al evaluated OSVV as an assessment tool in periodontology and found it to be a reliable, objective and convenient tool [7]. OSVV formats of examination are a very convenient and feasible method of assessment that reduces subjective bias [8.] A study carried out by Marya Ahsan et al 9 to assess the reliability of OSVV over traditional viva examination among second-year Pharmacology students, concluded that a moderate positive correlation (r = 0.442; P = 0.001) was seen between marks scored in structured viva and theory examination. OSVV examination may be considered more reliable and fairer in comparison to a traditional viva examination. Hence, it may be preferred over the traditional viva examination [9]. The ANOVA analysis of grand viva marks across batches revealed no statistically significant difference in performance between the groups.
This suggests that both OSVV and traditional assessment methods provided consistent results across all three batches. Although many previous studies pointed out that traditional vivas are not consistently reliable due to subjectivity and examiner bias, with different candidates often receiving different questions or levels of prompting, leading to inconsistent results. Although the traditional viva is prone to a significant “halo effect,” where an examiner’s overall judgment of a candidate’s competence may be biased by external appearance or other irrelevant attributes, no statistically significant difference was observed between the scores awarded in the OSVV and traditional viva [10-11]. This could be attributed to the expert panel of examiners, who maintained uniformity in both the questions and the level of difficulty.
Feedback from examiners and students reflected the OSVV acceptability among them. Since all the students were exposed to similar types of questions with the same difficulty level, they felt that the checklist system was a fair and unbiased method, with luck playing an insignificant role in the assessment. Desai et al concluded that, from the students' viewpoint, OSVV is a more accurate and objective method of practical viva examination [12]. It is accurate, trustworthy, and less subjective. Feedback from students also revealed that OSVV is more organised, curtails the examiner's bias and permits equal chances to each student. OSVV is beneficial in upgrading students’ performance.
Based on faculty perceptions regarding drawbacks of OSVV, teachers opined that prefixed questions provide less flexibility to students on topics they aren't well-versed in. Traditional viva provides a greater opportunity to score in areas where students are confident. All six faculty members agreed that OSVV is labour-intensive, reflecting a unanimous view of increased faculty effort in preparation. In resource-limited settings, examiners, time, expenses and intensive manpower required for preparation of stations are challenging for the faculty [13-15].
A novel aspect of our study was the inclusion of questions about higher-order cognitive domains, such as assessment of clinical decision-making and reasoning. The purpose was to expose the students to clinical microbiology and real patient scenarios. Traditional viva examinations largely assess recall-based knowledge; however, competency-based curricula require evaluation of higher cognitive domains along with soft skills such as attitude, ethics, and communication. These attributes are frequently underassessed even during practical exercises. Incorporating case-based scenarios addressing aspects such as respect for patient samples, confidentiality of reports, and privileged communication enables a more comprehensive assessment. Initiating the viva with simple recall questions helps reduce student anxiety and build confidence, while a structured progression toward higher-order questions facilitates sustained engagement and performance throughout the examination.
The implications of this study extend beyond Microbiology to other disciplines within medical education, where viva voce examinations remain a critical component of evaluation [16]. By promoting uniformity and fairness, OSVV can serve as a model for reforms in assessment strategies that aim to balance knowledge recall with higher-order thinking and professional competencies [17]. Furthermore, as CBME gains wider acceptance, structured assessment tools like OSVV will play an essential role in aligning examinations with curricular outcomes [18-19].
This study has certain limitations. First, it was conducted within a single department; therefore, similar studies across multiple disciplines are required to generate more comprehensive and generalizable data. Second, although conducting the structured viva on a single day would have minimised the risk of contamination, the examination was spread over two days due to the availability of only six faculty members. Nevertheless, potential contamination was mitigated by using different sets of questions on each day.
Conclusion
The present study underscores the growing importance of adopting structured and objective assessment methods in medical education. Traditional viva voce, though widely practised, often suffers from variability in examiner approach, subjective bias, and inconsistent grading, which compromise both the fairness and reliability of student evaluation. In contrast, OSVV demonstrated clear advantages by minimising subjectivity, enhancing standardisation, and ensuring a more transparent evaluation process. The significant improvement in student performance scores under the OSVV format, coupled with reduced inter-batch variation, validates it as a better assessment tool compared to the traditional method.
Equally important is the positive feedback received from both students and faculty, which reflects the acceptability and practicality of OSVV in routine academic practice. Students appreciated the clarity, fairness, and structured nature of the assessment, while faculty members valued its ability to comprehensively test different cognitive domains and communication skills without compromising on rigor.
These findings collectively suggest that OSVV not only enhances the objectivity of evaluation but also contributes to better student learning experiences by aligning assessment with modern educational principles. The implications of this study extend beyond microbiology to other disciplines within medical education where viva voce examinations remain a critical component of evaluation. By promoting uniformity and fairness, OSVV can serve as a model for reforms in assessment strategies that aim to balance knowledge recall with higher-order thinking and professional competencies. Furthermore, as CBME gains wider acceptance, structured assessment tools like OSVV will play an essential role in aligning examinations with curricular outcomes. However, successful implementation of OSVV requires institutional support, adequate faculty training, and development of validated question banks that encompass core knowledge as well as clinical and ethical dimensions.
Future research should explore the long-term impact of OSVV on student performance, confidence, and skill application in real clinical settings. Comparative studies across multiple institutions and specialties will further strengthen the evidence base for widespread adoption. OSVV represents a progressive step toward enhancing the quality of medical assessments. Its integration into the assessment framework has the potential to foster fairness, transparency, and competency in future healthcare professionals, ultimately contributing to the advancement of medical education and patient care.
Ethical considerations
This study was approved by the Institutional Ethics Committee of Dr. KNS Memorial Institute of Medical Sciences, Barabanki, Uttar Pradesh, India (approval code: 0256/24). Informed consent was obtained from all participants prior to their inclusion in the study.
Artificial intelligence utilization for article writing
Artificial intelligence tools were not utilised in the preparation of this manuscript.
Acknowledgment
The authors would like to thank all the students and faculty members who participated in this study.
Conflict of interest statement
The authors declare that they have no competing interests.
Author contributions
MR was responsible for the conceptualisation and methodology of the study, as well as data collection, formal analysis, and preparation of the original draft. SS contributed to the supervision and validation of the work, along with reviewing and editing the manuscript. Both authors have read and approved the final manuscript.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Data availability statement
The datasets used and analysed during the current study are available from the corresponding author upon reasonable request.
Background & Objective: Inconsistent evaluation with traditional viva voce undermines the reliability and validity of assessments. Objective Structured Viva Voce (OSVV) with standardized scoring ensures objective evaluation, less examiner bias, and subjectivity. This study aimed to compare the effectiveness of OSVV and traditional viva voce in assessing student performance.
Materials & Methods: This educational interventional study was carried out on 133 second-year Bachelor of Medicine and Bachelor of Surgery (MBBS) students. A pre-validated collection of viva cards, targeting recall and higher-order cognitive domains, was developed based on the Attitude, Ethics, and Communication (AETCOM) Module. The students were evaluated through two types of viva voce examinations using a crossover study design. Evaluation was done by comparing student scores using both methods, followed by a feedback questionnaire.
Results: There was a statistically significant difference (p < 0.001) in student scores, with higher average marks with the OSVV versus the traditional approach. The comparatively lower inter-batch variation in OSVV (F-value = 0.31, p-value = 0.734) highlights its greater consistency and unbiasedness in evaluation across different batches. Among the students, the overall satisfaction index was 59.53, suggesting a generally positive perception of OSVV. Faculty feedback indicated that OSVV can be used as a superior alternative to the traditional approach as an assessment tool.
Conclusion: The study highlights OSVV as a superior alternative to traditional viva, reducing bias and enhancing fairness. It demonstrated significant improvement in student performance and consistency. OSVV represents a progressive reform ensuring fairness, transparency, and competency in MBBS graduate assessments.
Introduction
Viva voce complements theory and practical examinations. It helps in the comprehensive assessment of students' capabilities in examinations. It involves face-to-face interaction where the examiner probes the student’s understanding, reasoning, and critical thinking skills. Viva voce aims to assess discernment and the student's ability to comprehend knowledge, think quickly, and demonstrate eloquent professional etiquette [1]. Our institute conducts undergraduate MBBS assessments using the traditional viva-voce, typically during the later phase of the practical examination. However, it is frequently observed that this conventional method lacks consistency, as the outcomes are often influenced by the examiner’s mood and personal biases. Conventional viva voce is traditionally conducted by different examiners depending on their availability on the day of the examination, thereby introducing additional variability in assessment. Examiner judgment may be affected by personal preferences, variations in their method of questioning, emphasis on specific content areas, and several other confounding factors.
Despite adequate knowledge, students may be unable to respond effectively due to limited recall time or intimidating behavior during the viva voce, resulting in heightened stress. Examiners may experience fatigue, lack of interest, or time constraints, which can influence the conduct of the assessment. The lack of standardisation results in considerable variability in question content and difficulty among examiners, frequently leading to incomplete coverage of the syllabus. Consequently, such variability may compromise the fairness of student assessment.
The examination largely emphasizes recall of knowledge, often restricted to core topics preferred by individual examiners. Owing to the lack of a structured format, higher-order cognitive domains such as application, reasoning, problem-solving, analysis, and synthesis are not adequately assessed. Additionally, domains such as ethics and professional attitude receive little attention in the traditional viva. Essential microbiology competencies, including respectful handling of patient samples and maintenance of patient confidentiality, are seldom evaluated. To achieve these objectives, we need an assessment tool that demonstrates validity, reliability, feasibility, and a positive professional educational impact. In an effort to address existing discrepancies in assessment practices, we sought to make the process more viable, uniform, transparent, and effective by implementing a structured viva voce examination. As assessment is a core component of Competency-Based Medical Education (CBME), the adoption of innovative assessment methods such as the OSVV in our institute is expected to overcome the limitations associated with conventional assessment approaches. Thus, this study was designed to study whether OSVV would be a better tool in assessing the performance of the students during examinations.
OSVV provides a uniform, preformed assessment framework with questionnaires and standardised scoring, ensuring objective evaluation consistently [2]. This reduces variability and minimises examiner bias and subjectivity, significantly improving the reliability and validity of assessments. OSVV helps assess specific competencies by framing questions with learning objectives and desired outcomes [3]. Students’ logical medical analysis, problem-solving capacities, and communication skills are evaluated [3]. OSVV provides more constructive appraisals to the students about their performance. Increasing evidence indicates that OSVV can assess students’ achievements in course outcomes beyond simple knowledge recall, encompassing problem-solving, critical thinking, decision-making, professionalism, ethics, and interpersonal skills [4, 5]. There is a paucity of data on the assessment of higher-order cognitive and affective domains through structured viva in the subject of microbiology. Some comparative studies conducted in the evaluation of student performance through traditional and structured viva only address the questions testing the simple recall of knowledge. Studies assessing the affective domain are also limited. 17 We included specific scenario-based questions integrated into the structured viva to probe a student's ethical judgment and professional attitudes, which fall under the higher levels of the affective domain. Thus, this study was designed to investigate whether OSVV would be a more effective tool in assessing student performance and to evaluate higher domains of learning through a structured viva in microbiology.
Materials & Methods
Design and setting(s)
This was an educational interventional study. This study was conducted at the Department of Microbiology, Dr. KNS Memorial Institute of Medical Sciences, over a duration of six months. The study duration was from January 2025 to June 2025.
Participants and sampling
A total of 133 second-year MBBS students were enrolled in the study. Convenience sampling was used: all second-year MBBS students willing to take part were included, while those not willing were excluded. Approval was obtained from the Institutional Ethics Committee. Students were oriented to the OSVV through structured demonstrations.
Tools/Instruments
The OSVV questions, checklists, and feedback questionnaires were created by subject experts and reviewed by senior faculty and medical education experts before use. Mock OSVV sessions were run to assess clarity, feasibility, time allocation, and scoring patterns. Content validity was ensured by mapping questions to prescribed MBBS microbiology competencies across knowledge, skills, and attitudinal domains. Reliability was addressed through standardised checklists, uniform marking schemes, and examiner training. Standard setting was based on institutional and CBME guidelines, with the passing criterion set at 50% of the cumulative marks in practical and viva examinations. A pre-validated set of viva cards addressing recall and higher-order domains based on the Attitude, Ethics, and Communication Module (AETCOM) was prepared. AETCOM is a mandatory longitudinal module introduced by the National Medical Commission, India, for MBBS students. This module is designed to mentor competent, ethical, empathetic, and communicative MBBS students. Questions were based on core competencies as per the NMC. CBME curriculum topics include general microbiology, bacteriology, serology, parasitology, and applied microbiology. Questions covered cognitive domains from knowledge recall to application and higher-order reasoning (Table 1). The questions also addressed the AETCOM components in Microbiology, thus allowing the assessment of various soft skills like respect for and confidentiality of patients’ samples and reports.
Table 1. Structure, domains, and mark distribution of the OSVV in Microbiology
Note: Descriptive statistics were used to present the structure and marks distribution of the OSVV examination.
Abbreviations: OSVV, objective structured viva voce; AETCOM, attitude, ethics and communication module.
We ensured the equivalence of question difficulty between the OSVV question sets used on Day 1 and Day 2 through a systematic review process. A panel of examiners compared the viva cards from both days to confirm uniformity in content coverage, cognitive level, and degree of difficulty, thereby maintaining consistency across examination days (Figure 1). Questions were grouped by difficulty, and two separate sets of cards with similar difficulty levels were made for Day 1 and Day 2. Although the questions for the traditional viva differed in content, they were carefully blueprint-matched and calibrated to ensure an equal level of difficulty across days and between assessment formats.
Abbreviations: OSVV, objective structured viva voce; AETCOM, attitude, ethics and communication module.
Figure 1. Flow diagram of the study methodology showing the crossover design and group allocation
Data collection methods
The students were assessed using two different formats of viva-voce examination in a crossover study design, where each student took part in both assessment formats at different times, thereby serving as their own control. Since students underwent assessment through a crossover design, all participants were exposed to both methods on separate occasions, which reduced inter-individual variability and improved comparability. Each student received five viva cards (totaling 25 marks) addressing different learning domains with varying difficulty levels, which included core microbiology topics (Figure 2). Students were given 8-10 minutes to answer the viva cards. Each student was assessed at a single station by a single examiner based on the five viva cards.
Figure 2. Sample viva card assessing higher cognitive and attitudinal domains
Evaluation was carried out by comparing student scores using both methods, followed by a feedback questionnaire. The examination was run over two days. Students were randomly divided into two groups of 66 each: the traditional viva voce group (controls) and the OSVV group (cases). Each group was further split into three batches of about 22 students, with each faculty member assessing one batch. On Day 1, participants in the case group underwent the OSVV, whereas the control group underwent the traditional viva voce. On Day 2, a crossover was implemented: students who had taken the OSVV on Day 1 were assessed by the traditional viva, and those who had taken the traditional viva on Day 1 were assessed using the OSVV. Faculty members ran the structured viva-voce using a predefined checklist. In the OSVV, student responses were evaluated using standardised scoring rubrics aligned with the checklist, with marks given for predefined key points, clarity of explanation, and communication skills. This ensured uniform assessment, reduced examiner bias, and improved objectivity and reliability of the evaluation process. In each OSVV set, five questions were assessed, with marks given for each question individually and the final score obtained by summing the individual scores (Table 1). In the traditional viva-voce, students were evaluated at the end of the examination. Each examiner independently assessed the student within an equal time frame, and the final score was derived by averaging the marks awarded by the examiners. Questions asked, responses given, and scores awarded were recorded simultaneously by the examiners to allow for structured constructive feedback at the end of the examination. Feedback forms with a pre-structured questionnaire were given to students after the OSVV on both days. Feedback was also collected from examiners using a separate questionnaire. Data were gathered using mark sheets and structured feedback questionnaires. Pre-validated viva cards and checklists were used for the OSVV, along with pre-validated structured questionnaires given to students and observers to get feedback.
Data analysis
The data were analyzed to compare student scores between the OSVV and traditional viva voce methods using the unpaired t-test. An ANOVA analysis was performed to check for significant differences in performance across different batches. A satisfaction index was calculated from the student feedback questionnaires to evaluate their perception of the OSVV method. Descriptive statistics were used to summarize faculty feedback.
Results
Comparing grand viva marks (maximum 25) between the two assessment methods showed a clear difference. The OSVV method gave a higher mean score of 18.56 ± 1.30, whereas the traditional method recorded a lower mean of 13.26 ± 1.13. The mean difference between the two methods was 5.30, and statistical analysis using the unpaired t-test showed a highly significant difference with a t-value of 42.75 and a p-value < 0.001, indicating that the OSVV method was significantly more effective than the traditional method in student performance evaluation (Table 2, Figure 3).
Data analysis
The data were analyzed to compare student scores between the OSVV and traditional viva voce methods using the unpaired t-test. An ANOVA analysis was performed to check for significant differences in performance across different batches. A satisfaction index was calculated from the student feedback questionnaires to evaluate their perception of the OSVV method. Descriptive statistics were used to summarize faculty feedback.
Results
Comparing grand viva marks (maximum 25) between the two assessment methods showed a clear difference. The OSVV method gave a higher mean score of 18.56 ± 1.30, whereas the traditional method recorded a lower mean of 13.26 ± 1.13. The mean difference between the two methods was 5.30, and statistical analysis using the unpaired t-test showed a highly significant difference with a t-value of 42.75 and a p-value < 0.001, indicating that the OSVV method was significantly more effective than the traditional method in student performance evaluation (Table 2, Figure 3).
Table 2. Comparison of grand viva marks between the two assessment methods
Note: Unpaired t-test was used to compare the mean scores between the OSVV and traditional viva voce assessment methods.
Abbreviations: OSVV, objective structured viva voce; SD, standard deviation.
Figure 3: Comparison of grand viva marks between the two assessment methods
Comparing grand viva marks between OSVV and the traditional assessment method across all three batches showed consistently higher performance with OSVV. In batch 1, the OSVV group had a mean score of 18.68 ± 1.31, while the traditional method scored 13.30 ± 1.23, with a mean difference of 5.39 (Figure 4). The unpaired t-test gave a t-value of 26.12 with a p-value < 0.001, indicating a highly significant difference. Similarly, for batch 2, students assessed through OSVV got a mean score of 18.48 ± 1.27 compared to 13.43 ± 1.15 with the traditional method, with a mean difference of 5.05, which was statistically significant (t = 23.96, p < 0.001). In batch 3, OSVV students achieved a mean score of 18.51 ± 1.34, whereas those assessed traditionally scored 13.04 ± 1.00, resulting in a mean difference of 5.47. This difference was again highly significant (t = 24.18, p < 0.001). Thus, across all batches, OSVV consistently outperformed the traditional assessment method with statistically significant differences. The ANOVA analysis of grand viva marks across batches showed no statistically significant difference in performance between the groups (Figure 5).Figure 4: Comparison of batch-wise grand viva marks between two assessment methods
Figure 5: Comparison of grand viva marks among the batches for the two assessment methods
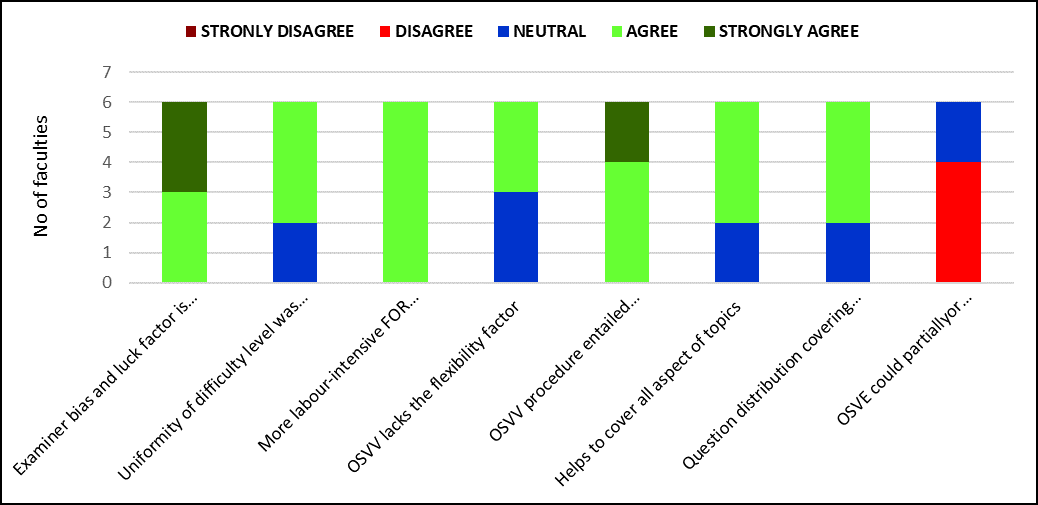
For the OSVV method, batch 1 scored a mean of 18.68 ± 1.31, batch 2 scored 18.48 ± 1.27, and batch 3 scored 18.51 ± 1.34, with an overall F-value of 0.31 and p = 0.734, indicating uniformity across batches. Similarly, for the traditional method, batch 1 had a mean of 13.30 ± 1.23, batch 2 scored 13.43 ± 1.15, and batch 3 scored 13.04 ± 1.00, with an F-value of 1.35 and p = 0.263, again showing no significant batch-wise variation. This suggests that both OSVV and traditional assessment methods provided consistent results across all three batches. The satisfaction index for various aspects of the OSVV reflected moderate levels of student satisfaction (Figure 6). The highest satisfaction was seen for the statement “Adequate time provided” with an index of 66.17, followed by “I realised what I know from the entire syllabus” (62.78) and “Questions are easy to understand as they are to the point and precise” (61.28). Other items, such as “All topics are covered” (60.15) and “OSVV is well organised” (63.16), also showed favourable responses. The lowest satisfaction was noted for the negatively worded item “OSVV is tiresome, confusing.” The item “OSVV will enhance my performance” had a satisfaction index of 59.21. The overall satisfaction index for OSVV was 59.53. The findings imply that while the OSVV is an acceptable and feasible assessment method, refinements in implementation and orientation may improve its overall acceptance and effectiveness. The faculty feedback on OSVV was collected item-wise to understand their perceptions regarding various aspects of the evaluation method (Figure 7). For the item “Examiner bias and luck factor is minimised in OSVV,” responses were balanced, with 3 faculty members agreeing and 3 strongly agreeing, indicating a consensus that OSVV improves objectivity. Regarding the “Uniformity of difficulty level ensured in the OSVV procedure,” 2 faculty members stayed neutral, while 4 agreed, suggesting a general positive perception with some reservations. When asked whether OSVV is more labour-intensive for faculty due to groundwork, all 6 faculty members agreed, reflecting a unanimous view of increased faculty effort in preparation. For the statement “OSVV lacks the flexibility factor,” opinions were mixed, with 3 neutral and 3 agreeing, indicating moderate concern over adaptability. On whether “OSVV procedure entailed minimal faculty-student interactivity,” 4 agreed and 2 strongly agreed, highlighting a perceived reduction in engagement.
Figure 6. Item-wise and overall satisfaction index of the OSVV method
Figure 7. Faculty feedback on OSVV
Discussion
Assessment is an integral part of the curriculum, which plays a vital role in the learning process. Assessment has a direct influence on learning, as it determines whether a learner has attained the required level of competency. Over time, assessment has evolved into a dynamic process, becoming more robust, reliable, valid, fair, and grounded in evidence-based practices [6]. An oral examination fosters professional interaction between the assessor and the student, aiming to evaluate core competencies, particularly higher-order cognitive skills such as analysis, evaluation, and synthesis. Overall, the difference in average marks obtained by the students in the OSVV method and the conventional method was statistically significant (p <0.001). The students gained higher marks in OSVV, indicating it to be significantly more effective than the traditional method in student performance evaluation. Across all batches, OSVV consistently outperformed the traditional assessment method with statistically significant differences.
Rathod et al evaluated OSVV as an assessment tool in periodontology and found it to be a reliable, objective and convenient tool [7]. OSVV formats of examination are a very convenient and feasible method of assessment that reduces subjective bias [8.] A study carried out by Marya Ahsan et al 9 to assess the reliability of OSVV over traditional viva examination among second-year Pharmacology students, concluded that a moderate positive correlation (r = 0.442; P = 0.001) was seen between marks scored in structured viva and theory examination. OSVV examination may be considered more reliable and fairer in comparison to a traditional viva examination. Hence, it may be preferred over the traditional viva examination [9]. The ANOVA analysis of grand viva marks across batches revealed no statistically significant difference in performance between the groups.
This suggests that both OSVV and traditional assessment methods provided consistent results across all three batches. Although many previous studies pointed out that traditional vivas are not consistently reliable due to subjectivity and examiner bias, with different candidates often receiving different questions or levels of prompting, leading to inconsistent results. Although the traditional viva is prone to a significant “halo effect,” where an examiner’s overall judgment of a candidate’s competence may be biased by external appearance or other irrelevant attributes, no statistically significant difference was observed between the scores awarded in the OSVV and traditional viva [10-11]. This could be attributed to the expert panel of examiners, who maintained uniformity in both the questions and the level of difficulty.
Feedback from examiners and students reflected the OSVV acceptability among them. Since all the students were exposed to similar types of questions with the same difficulty level, they felt that the checklist system was a fair and unbiased method, with luck playing an insignificant role in the assessment. Desai et al concluded that, from the students' viewpoint, OSVV is a more accurate and objective method of practical viva examination [12]. It is accurate, trustworthy, and less subjective. Feedback from students also revealed that OSVV is more organised, curtails the examiner's bias and permits equal chances to each student. OSVV is beneficial in upgrading students’ performance.
Based on faculty perceptions regarding drawbacks of OSVV, teachers opined that prefixed questions provide less flexibility to students on topics they aren't well-versed in. Traditional viva provides a greater opportunity to score in areas where students are confident. All six faculty members agreed that OSVV is labour-intensive, reflecting a unanimous view of increased faculty effort in preparation. In resource-limited settings, examiners, time, expenses and intensive manpower required for preparation of stations are challenging for the faculty [13-15].
A novel aspect of our study was the inclusion of questions about higher-order cognitive domains, such as assessment of clinical decision-making and reasoning. The purpose was to expose the students to clinical microbiology and real patient scenarios. Traditional viva examinations largely assess recall-based knowledge; however, competency-based curricula require evaluation of higher cognitive domains along with soft skills such as attitude, ethics, and communication. These attributes are frequently underassessed even during practical exercises. Incorporating case-based scenarios addressing aspects such as respect for patient samples, confidentiality of reports, and privileged communication enables a more comprehensive assessment. Initiating the viva with simple recall questions helps reduce student anxiety and build confidence, while a structured progression toward higher-order questions facilitates sustained engagement and performance throughout the examination.
The implications of this study extend beyond Microbiology to other disciplines within medical education, where viva voce examinations remain a critical component of evaluation [16]. By promoting uniformity and fairness, OSVV can serve as a model for reforms in assessment strategies that aim to balance knowledge recall with higher-order thinking and professional competencies [17]. Furthermore, as CBME gains wider acceptance, structured assessment tools like OSVV will play an essential role in aligning examinations with curricular outcomes [18-19].
This study has certain limitations. First, it was conducted within a single department; therefore, similar studies across multiple disciplines are required to generate more comprehensive and generalizable data. Second, although conducting the structured viva on a single day would have minimised the risk of contamination, the examination was spread over two days due to the availability of only six faculty members. Nevertheless, potential contamination was mitigated by using different sets of questions on each day.
Conclusion
The present study underscores the growing importance of adopting structured and objective assessment methods in medical education. Traditional viva voce, though widely practised, often suffers from variability in examiner approach, subjective bias, and inconsistent grading, which compromise both the fairness and reliability of student evaluation. In contrast, OSVV demonstrated clear advantages by minimising subjectivity, enhancing standardisation, and ensuring a more transparent evaluation process. The significant improvement in student performance scores under the OSVV format, coupled with reduced inter-batch variation, validates it as a better assessment tool compared to the traditional method.
Equally important is the positive feedback received from both students and faculty, which reflects the acceptability and practicality of OSVV in routine academic practice. Students appreciated the clarity, fairness, and structured nature of the assessment, while faculty members valued its ability to comprehensively test different cognitive domains and communication skills without compromising on rigor.
These findings collectively suggest that OSVV not only enhances the objectivity of evaluation but also contributes to better student learning experiences by aligning assessment with modern educational principles. The implications of this study extend beyond microbiology to other disciplines within medical education where viva voce examinations remain a critical component of evaluation. By promoting uniformity and fairness, OSVV can serve as a model for reforms in assessment strategies that aim to balance knowledge recall with higher-order thinking and professional competencies. Furthermore, as CBME gains wider acceptance, structured assessment tools like OSVV will play an essential role in aligning examinations with curricular outcomes. However, successful implementation of OSVV requires institutional support, adequate faculty training, and development of validated question banks that encompass core knowledge as well as clinical and ethical dimensions.
Future research should explore the long-term impact of OSVV on student performance, confidence, and skill application in real clinical settings. Comparative studies across multiple institutions and specialties will further strengthen the evidence base for widespread adoption. OSVV represents a progressive step toward enhancing the quality of medical assessments. Its integration into the assessment framework has the potential to foster fairness, transparency, and competency in future healthcare professionals, ultimately contributing to the advancement of medical education and patient care.
Ethical considerations
This study was approved by the Institutional Ethics Committee of Dr. KNS Memorial Institute of Medical Sciences, Barabanki, Uttar Pradesh, India (approval code: 0256/24). Informed consent was obtained from all participants prior to their inclusion in the study.
Artificial intelligence utilization for article writing
Artificial intelligence tools were not utilised in the preparation of this manuscript.
Acknowledgment
The authors would like to thank all the students and faculty members who participated in this study.
Conflict of interest statement
The authors declare that they have no competing interests.
Author contributions
MR was responsible for the conceptualisation and methodology of the study, as well as data collection, formal analysis, and preparation of the original draft. SS contributed to the supervision and validation of the work, along with reviewing and editing the manuscript. Both authors have read and approved the final manuscript.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Data availability statement
The datasets used and analysed during the current study are available from the corresponding author upon reasonable request.
Article Type : Orginal Research |
Subject:
Medical Education
Received: 2025/10/23 | Accepted: 2026/02/22 | Published: 2026/04/1
Received: 2025/10/23 | Accepted: 2026/02/22 | Published: 2026/04/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
