
Tue, Jul 28, 2026
[Archive]
Volume 19, Issue 1 (2026)
J Med Edu Dev 2026, 19(1): 92-96 |
Back to browse issues page

Ethics code: IR.ZUMS.REC.1401.160
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Karimkhanlooei G, Abdollahi Sabet S, Pashazadeh F. Self-directed learning readiness among medical students: an observational study. J Med Edu Dev 2026; 19 (1) :92-96
URL: http://edujournal.zums.ac.ir/article-1-2584-en.html
URL: http://edujournal.zums.ac.ir/article-1-2584-en.html

1- Department of English Language, Faculty of Medicine, Zanjan University of Medical Sciences, Zanjan, Iran
2- Department of Community Medicine, Faculty of Medicine, Zanjan University of Medical Sciences, Zanjan, Iran ,gitikarimkhanlooei@gmail.com
3- School of Medicine, Zanjan University of Medical Sciences, Zanjan, Iran
2- Department of Community Medicine, Faculty of Medicine, Zanjan University of Medical Sciences, Zanjan, Iran ,
3- School of Medicine, Zanjan University of Medical Sciences, Zanjan, Iran
Full-Text [PDF 444 kb]
(191 Downloads)
| Abstract (HTML) (480 Views)
Full-Text: (61 Views)
Abstract
Background & Objective: Self-Directed Learning (SDL) is essential for medical students to develop lifelong learning skills. This study aimed to evaluate SDL readiness and examine how demographic characteristics affect medical students at Zanjan University of Medical Sciences.
Materials & Methods: We used a cross-sectional design with 201 purposefully sampled medical students. Data were collected using Fisher’s 40-item validated SDL readiness instrument, available in Persian. We analyzed the data using SPSS version 26 with independent-samples t-tests and a one-way ANOVA. Statistical significance was set at p < 0.05.
Results: The mean SDL score was 160.88 ± 17.25, showing high readiness based on scale criteria. No differences in SDL scores were found between males and females (p = 0.448) or by educational level (p = 0.414). SDL scores were significantly lower for students aged 19–21 compared to those aged 22–23 (p = 0.014) or ≥ 24 years (p = 0.017).
Conclusion: Overall, SDL readiness is high and positively associated with age and maturity, rather than educational level or gender. This suggests teaching methods should be included in the curriculum to create environments where self-directed learning can thrive, particularly for younger medical students.
Introduction
Self-Directed Learning (SDL) is an active process in which individuals take responsibility for identifying their learning needs, setting goals, finding resources, choosing learning strategies, and evaluating outcomes [1]. In medical education, SDL has become fundamental to developing lifelong learning skills, as healthcare practitioners must adapt to rapid knowledge growth and changing practices [2, 3]. Given SDL’s essential role, assessing medical students' SDL readiness is a valuable research endeavor. Several studies have documented relationships between SDL and demographic variables, but findings have been inconsistent. Some studies show significant associations with age and gender [4, 5], while others find no connection [6, 7]. Regarding educational level, clarity is lacking. Some evidence suggests SDL readiness declines as students progress, while other evidence suggests no change [8, 9]. This inconsistency reveals a knowledge gap, especially in Iranian medical education, where cultural and curricular differences may shape the development of SDL skills. We conducted this study to address this gap. It provides context-specific data to guide local curriculum development and faculty training to encourage SDL. Understanding how age, gender, and educational level relate to SDL readiness in this setting helps educators design effective interventions. This study examined three demographic variables—age, gender, and educational level—simultaneously in a single cohort of Iranian medical students using a validated instrument to assess their combined effect on SDL readiness. The result is a detailed understanding of each variable’s relationship with readiness as they are assessed together, rather than separately. Previous studies have examined SDL in many contexts, but their applicability to this student population may be limited. For example, some studies examined Massive Open Online Course (MOOC) learners [10] or nursing students’ professional values [11], addressing different populations in different settings. Even research on practicing nurses and midwives [12] represents a different professional group with unique practice contexts, motivations, and experiences. This study fills a specific gap in the medical education environment of Iranian medical students. We sought to examine self-directed learning readiness and its relationship with age, gender, and educational level among medical students at Zanjan University of Medical Sciences.
Materials & Methods
Design and setting(s)
This cross-sectional study was conducted from September 23, 2022, to March 20, 2023, among two hundred and one medical students at Zanjan University of Medical Sciences, Zanjan, Iran.
Participants and sampling
Sample size was based on Nadi’s study [13] using the formula ‘n = Z²σ² ÷ d²’, with σ = 7.6 and d = 0.1σ, yielding 201 participants. At the time of the study, 962 students were enrolled across four educational levels. We included 201 participants using quota sampling proportional to student numbers at each level.
Tools/Instruments
We used the Persian version of the Self-Directed Learning Scale developed by Fisher and colleagues [14]. This 40-item instrument assesses attitudes, skills, and attributes that determine SDL readiness. Nadi et al [13] reported a Cronbach’s alpha of 0.913, Spearman-Brown coefficient of 0.899, Guttman coefficient of 0.898, and test-retest reliability of 0.861 for the Persian version. The questionnaire measures three dimensions: self-management (items 1-13), desire to learn (items 14-25), and self-control (items 26-40). Items are scored on a scale of 1 to 5.
Data collection methods
We provided students with a detailed explanation of the research procedures.
After obtaining consent, we distributed questionnaires. Students were informed that responses would be anonymous and that results would be reported without identifying information.
Data analysis
We analyzed data using SPSS version 26, with p < 0.05 considered statistically significant. Qualitative variables were described using frequencies and percentages; quantitative variables were summarized using means and standard deviations. We used independent sample t-tests for two-group comparisons and one-way ANOVA for multi-group comparisons.
Results
A total of 201 students participated: 117 (58.2%) females and 84 (41.8%) males. The sample represented four educational levels (Table 1). Mean age was 24.15 ± 2.77 years (range: 18-31 years).
Table 1. Demographic characteristics of the students

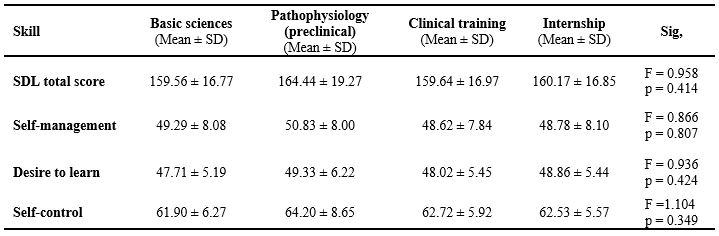
No statistically significant differences were observed in total SDL score or its three dimensions between male and female students (p > 0.05 for all comparisons) (Table 3). Similarly, SDL scores across the four educational levels showed no significant differences in total score or subscales (p > 0.05) (Table 4).
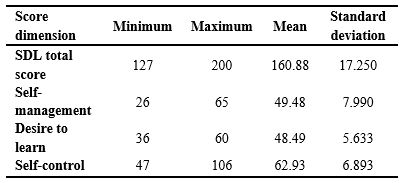
Table 2. Descriptive statistics for self-directed learning scores
Abbreviations: SDL, self-directed learning.
Table 3. Comparison of self-directed learning scores by gender
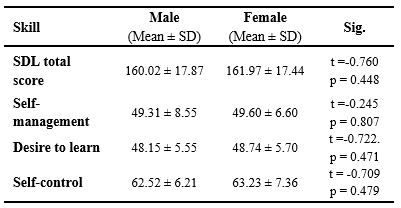
Table 4. Self-directed learning scores by educational level
Note: One-way ANOVA test was used for group comparisons.
Abbreviations: SD, standard deviation; Sig. statistical significance p, probability; SDL, self-directed learning.
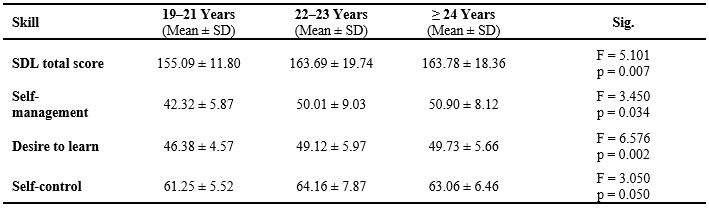
Table 5. Self-directed learning scores by age group
Discussion
This study examined self-directed learning readiness among medical students at Zanjan University of Medical Sciences. A total SDL score of 160.88 indicates high readiness for self-directed learning, consistent with benchmarks set by Fisher et al. [14] and Bhandari et al. [2]. A key finding is that SDL readiness varies considerably by age. Students aged 19–21 had significantly lower total and subscale SDL scores than older students. This finding aligns with Knowles’s andragogy theory, which suggests individuals become more self-directed as they age [1]. Age-related improvements may reflect greater cognitive maturity, increased life experience, and clearer professional identity, contributing to greater responsibility and proactivity in learning. Importantly, this age effect was independent of educational level, as no significant differences emerged across the four educational stages. This indicates that developmental maturation, rather than formal curriculum alone, is key to developing SDL competence. This contrasts with Premkumar et al. [10] and Malekian et al. [15], who found no age effect, suggesting contextual and cultural factors may influence the relationship. Unlike age, we found no significant gender differences in SDL readiness. This aligns with Premkumar et al. [10] and Malekian et al. [15] but contrasts with Lee et al. [12] and Arabshahi et al. [16], who reported gender differences. The absence of gender differences may reflect an equitable learning environment for both sexes in this setting. The lack of differences across educational levels is also consistent with Arabshahi et al. [16] and suggests that progression from preclinical to clinical training did not inherently improve SDL readiness in our sample. This raises the possibility that more deliberate, structured instructional approaches may be needed to develop these skills across the curriculum, rather than relying solely on clinical immersion. The strong self-control scores are notable and may result from students’ ability to manage learning within the provided structure. The literature supports the idea that SDL is effective only when learners can manage their own learning [17]. Faculty play a crucial role. As noted by Murad et al. [18], educators must shift from traditional teaching roles to facilitators for SDL to occur. Faculty development is needed to help educators guide learners in identifying learning needs and designing appropriate strategies.
This study, like any research, has limitations. The use of self-reported data may be subject to social desirability bias. Additionally, as a cross-sectional design, data collected at a single time point cannot establish causality or track longitudinal changes in SDL readiness. Finally, the single-institution setting limits the generalizability of the findings to other curricular structures or cultural contexts.
Conclusion
This study demonstrates that medical students at Zanjan University of Medical Sciences possess a high overall readiness for SDL. A key finding is that SDL readiness is significantly influenced by age and maturity, with students aged 19–21 years showing lower scores compared to their older peers, independent of their educational level or gender.
This suggests that cognitive and experiential development plays a more central role in fostering SDL than formal curricular progression alone. These results highlight the need for educational strategies that are responsive to students' developmental stages. Integrating structured support for younger learners—such as guided goal-setting, mentorship, and scaffolded reflective practices—could help bridge the readiness gap and promote lifelong learning competencies across all phases of medical training. By intentionally nurturing SDL skills early in the curriculum, institutions can better prepare future physicians to adapt independently to evolving clinical knowledge and practices.
Ethical considerations
The study received ethical approval (IR.ZUMS.REC.1401.160) from the Ethics Committee of Zanjan University of Medical Sciences. Students received detailed explanations of research procedures. After providing informed consent, they completed anonymous questionnaires. Results were reported without identifying information.
Artificial intelligence utilization for article writing
The authors did not use any artificial intelligence tools for writing, data analysis, or content generation in the preparation of this manuscript. The authors confirm they have reviewed and take full responsibility for the entire content of this publication.
Acknowledgment
The authors sincerely thank the medical students of Zanjan University of Medical Sciences for their participation in this study. We are also grateful to the university’s Vice-Chancellor for Education and the Faculty of Medicine for their administrative support and facilitation of data collection.
Our appreciation extends to the colleagues who provided valuable feedback during the preparation of this manuscript. Finally, we acknowledge the developers of the Self-Directed Learning Readiness Scale (SDLRS) for their instrument, which made this assessment possible.
Conflict of interest statement
The authors declare no actual or perceived conflicts of interest.
Author contributions
SAS contributed to conception, design, data analysis, manuscript revision, and journal correspondence as the corresponding author. FP contributed to data collection and manuscript drafting. GK contributed to conception, manuscript drafting, and revision.
Funding
This research received no specific grant from public, commercial, or not-for-profit funding agencies.
Data availability statement
Data belong to ZUMS and are available from the corresponding author upon reasonable request.
Background & Objective: Self-Directed Learning (SDL) is essential for medical students to develop lifelong learning skills. This study aimed to evaluate SDL readiness and examine how demographic characteristics affect medical students at Zanjan University of Medical Sciences.
Materials & Methods: We used a cross-sectional design with 201 purposefully sampled medical students. Data were collected using Fisher’s 40-item validated SDL readiness instrument, available in Persian. We analyzed the data using SPSS version 26 with independent-samples t-tests and a one-way ANOVA. Statistical significance was set at p < 0.05.
Results: The mean SDL score was 160.88 ± 17.25, showing high readiness based on scale criteria. No differences in SDL scores were found between males and females (p = 0.448) or by educational level (p = 0.414). SDL scores were significantly lower for students aged 19–21 compared to those aged 22–23 (p = 0.014) or ≥ 24 years (p = 0.017).
Conclusion: Overall, SDL readiness is high and positively associated with age and maturity, rather than educational level or gender. This suggests teaching methods should be included in the curriculum to create environments where self-directed learning can thrive, particularly for younger medical students.
Introduction
Materials & Methods
Design and setting(s)
This cross-sectional study was conducted from September 23, 2022, to March 20, 2023, among two hundred and one medical students at Zanjan University of Medical Sciences, Zanjan, Iran.
Participants and sampling
Sample size was based on Nadi’s study [13] using the formula ‘n = Z²σ² ÷ d²’, with σ = 7.6 and d = 0.1σ, yielding 201 participants. At the time of the study, 962 students were enrolled across four educational levels. We included 201 participants using quota sampling proportional to student numbers at each level.
Tools/Instruments
We used the Persian version of the Self-Directed Learning Scale developed by Fisher and colleagues [14]. This 40-item instrument assesses attitudes, skills, and attributes that determine SDL readiness. Nadi et al [13] reported a Cronbach’s alpha of 0.913, Spearman-Brown coefficient of 0.899, Guttman coefficient of 0.898, and test-retest reliability of 0.861 for the Persian version. The questionnaire measures three dimensions: self-management (items 1-13), desire to learn (items 14-25), and self-control (items 26-40). Items are scored on a scale of 1 to 5.
Data collection methods
We provided students with a detailed explanation of the research procedures.
After obtaining consent, we distributed questionnaires. Students were informed that responses would be anonymous and that results would be reported without identifying information.
Data analysis
We analyzed data using SPSS version 26, with p < 0.05 considered statistically significant. Qualitative variables were described using frequencies and percentages; quantitative variables were summarized using means and standard deviations. We used independent sample t-tests for two-group comparisons and one-way ANOVA for multi-group comparisons.
Results
A total of 201 students participated: 117 (58.2%) females and 84 (41.8%) males. The sample represented four educational levels (Table 1). Mean age was 24.15 ± 2.77 years (range: 18-31 years).
Table 1. Demographic characteristics of the students
Note: Data are presented as mean ± standard deviation for age and as frequency (percentage) for gender.
Abbreviations: n, number; SD, standard deviation.
Overall and dimension-specific SDL scores are presented in Table 2. Total SDL scores showed high readiness.Abbreviations: n, number; SD, standard deviation.
No statistically significant differences were observed in total SDL score or its three dimensions between male and female students (p > 0.05 for all comparisons) (Table 3). Similarly, SDL scores across the four educational levels showed no significant differences in total score or subscales (p > 0.05) (Table 4).
Table 2. Descriptive statistics for self-directed learning scores
Abbreviations: SDL, self-directed learning.
Table 3. Comparison of self-directed learning scores by gender
Note: An independent samples t-test was used for group comparisons.
Abbreviations: SD, standard deviation; Sig. statistical significance p, probability; SDL, self-directed learning.
Participants were categorized into three age groups: 19–21 years, 22–23 years, and ≥ 24 years. SDL score comparisons across these groups are shown in Table 5. Total SDL scores differed significantly by age group (p = 0.007). Post-hoc analysis (Tukey HSD) showed that the 19–21-year-old group had significantly lower scores than both the 22–23-year-old (p = 0.014) and the ≥ 24-year-old groups (p = 0.017), with no difference between the older groups (p = 1.00). Similar patterns emerged for SDL dimensions. For self-management (p = 0.034), the 19–21-year-old group scored lower than the ≥ 24-year-old group (p = 0.033). For desire to learn (p = 0.002), the youngest group scored lower than the 22–23-year-old (p = 0.012) and ≥ 24-year-old or older groups (p = 0.002). For self-control (p = 0.050), the 19–21-year-old group scored lower than the 22–23-year-old group (p = 0.039).
Abbreviations: SD, standard deviation; Sig. statistical significance p, probability; SDL, self-directed learning.
Participants were categorized into three age groups: 19–21 years, 22–23 years, and ≥ 24 years. SDL score comparisons across these groups are shown in Table 5. Total SDL scores differed significantly by age group (p = 0.007). Post-hoc analysis (Tukey HSD) showed that the 19–21-year-old group had significantly lower scores than both the 22–23-year-old (p = 0.014) and the ≥ 24-year-old groups (p = 0.017), with no difference between the older groups (p = 1.00). Similar patterns emerged for SDL dimensions. For self-management (p = 0.034), the 19–21-year-old group scored lower than the ≥ 24-year-old group (p = 0.033). For desire to learn (p = 0.002), the youngest group scored lower than the 22–23-year-old (p = 0.012) and ≥ 24-year-old or older groups (p = 0.002). For self-control (p = 0.050), the 19–21-year-old group scored lower than the 22–23-year-old group (p = 0.039).
Table 4. Self-directed learning scores by educational level
Note: One-way ANOVA test was used for group comparisons.
Abbreviations: SD, standard deviation; Sig. statistical significance p, probability; SDL, self-directed learning.
Table 5. Self-directed learning scores by age group
Note: One-way ANOVA test was used for group comparisons.
Abbreviations: SD, standard deviation; Sig. statistical significance p, probability; SDL, self-directed learning.
Abbreviations: SD, standard deviation; Sig. statistical significance p, probability; SDL, self-directed learning.
Discussion
This study examined self-directed learning readiness among medical students at Zanjan University of Medical Sciences. A total SDL score of 160.88 indicates high readiness for self-directed learning, consistent with benchmarks set by Fisher et al. [14] and Bhandari et al. [2]. A key finding is that SDL readiness varies considerably by age. Students aged 19–21 had significantly lower total and subscale SDL scores than older students. This finding aligns with Knowles’s andragogy theory, which suggests individuals become more self-directed as they age [1]. Age-related improvements may reflect greater cognitive maturity, increased life experience, and clearer professional identity, contributing to greater responsibility and proactivity in learning. Importantly, this age effect was independent of educational level, as no significant differences emerged across the four educational stages. This indicates that developmental maturation, rather than formal curriculum alone, is key to developing SDL competence. This contrasts with Premkumar et al. [10] and Malekian et al. [15], who found no age effect, suggesting contextual and cultural factors may influence the relationship. Unlike age, we found no significant gender differences in SDL readiness. This aligns with Premkumar et al. [10] and Malekian et al. [15] but contrasts with Lee et al. [12] and Arabshahi et al. [16], who reported gender differences. The absence of gender differences may reflect an equitable learning environment for both sexes in this setting. The lack of differences across educational levels is also consistent with Arabshahi et al. [16] and suggests that progression from preclinical to clinical training did not inherently improve SDL readiness in our sample. This raises the possibility that more deliberate, structured instructional approaches may be needed to develop these skills across the curriculum, rather than relying solely on clinical immersion. The strong self-control scores are notable and may result from students’ ability to manage learning within the provided structure. The literature supports the idea that SDL is effective only when learners can manage their own learning [17]. Faculty play a crucial role. As noted by Murad et al. [18], educators must shift from traditional teaching roles to facilitators for SDL to occur. Faculty development is needed to help educators guide learners in identifying learning needs and designing appropriate strategies.
This study, like any research, has limitations. The use of self-reported data may be subject to social desirability bias. Additionally, as a cross-sectional design, data collected at a single time point cannot establish causality or track longitudinal changes in SDL readiness. Finally, the single-institution setting limits the generalizability of the findings to other curricular structures or cultural contexts.
Conclusion
This study demonstrates that medical students at Zanjan University of Medical Sciences possess a high overall readiness for SDL. A key finding is that SDL readiness is significantly influenced by age and maturity, with students aged 19–21 years showing lower scores compared to their older peers, independent of their educational level or gender.
This suggests that cognitive and experiential development plays a more central role in fostering SDL than formal curricular progression alone. These results highlight the need for educational strategies that are responsive to students' developmental stages. Integrating structured support for younger learners—such as guided goal-setting, mentorship, and scaffolded reflective practices—could help bridge the readiness gap and promote lifelong learning competencies across all phases of medical training. By intentionally nurturing SDL skills early in the curriculum, institutions can better prepare future physicians to adapt independently to evolving clinical knowledge and practices.
Ethical considerations
The study received ethical approval (IR.ZUMS.REC.1401.160) from the Ethics Committee of Zanjan University of Medical Sciences. Students received detailed explanations of research procedures. After providing informed consent, they completed anonymous questionnaires. Results were reported without identifying information.
Artificial intelligence utilization for article writing
The authors did not use any artificial intelligence tools for writing, data analysis, or content generation in the preparation of this manuscript. The authors confirm they have reviewed and take full responsibility for the entire content of this publication.
Acknowledgment
The authors sincerely thank the medical students of Zanjan University of Medical Sciences for their participation in this study. We are also grateful to the university’s Vice-Chancellor for Education and the Faculty of Medicine for their administrative support and facilitation of data collection.
Our appreciation extends to the colleagues who provided valuable feedback during the preparation of this manuscript. Finally, we acknowledge the developers of the Self-Directed Learning Readiness Scale (SDLRS) for their instrument, which made this assessment possible.
Conflict of interest statement
The authors declare no actual or perceived conflicts of interest.
Author contributions
SAS contributed to conception, design, data analysis, manuscript revision, and journal correspondence as the corresponding author. FP contributed to data collection and manuscript drafting. GK contributed to conception, manuscript drafting, and revision.
Funding
This research received no specific grant from public, commercial, or not-for-profit funding agencies.
Data availability statement
Data belong to ZUMS and are available from the corresponding author upon reasonable request.
Article Type : Orginal Research |
Subject:
Medical Education
Received: 2025/09/9 | Accepted: 2025/12/11 | Published: 2026/01/1
Received: 2025/09/9 | Accepted: 2025/12/11 | Published: 2026/01/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
