
Tue, Jun 16, 2026
[Archive]
Volume 19, Issue 2 (2026)
J Med Edu Dev 2026, 19(2): 49-57 |
Back to browse issues page
Ethics code: IR.NUMS.REC.1401.022
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Andishmand Z, Babaei K, Moghadampasha A, Ali-Abadi T, Alinejad Mofrad S, Khaleghipour M et al . The effectiveness of Henderson's resilience model on self-efficacy and psychological distress among nursing students: a randomized controlled trial. J Med Edu Dev 2026; 19 (2) :49-57
URL: http://edujournal.zums.ac.ir/article-1-2594-en.html
URL: http://edujournal.zums.ac.ir/article-1-2594-en.html
Zahra Andishmand1, Kiana Babaei2, Azam Moghadampasha1, Tayyebeh Ali-Abadi *3, Samaneh Alinejad Mofrad4, Mostafa Khaleghipour5, Mehdi Bakaian6
1- Counseling center, Neyshabur University of Medical Sciences, Neyshabur, Iran
2- Department of Anesthesia, Neyshabur University of Medical Sciences, Neyshabur, iran
3- Department of Nursing, Neyshabur, University of Medical Sciences, Neyshabur, Iran ,tayebealiabadi@yahoo.com
4- School of Nursing, Faculty of Science, Medicine and Health, University of Wollongong, South Western Sydney Campus, Australia
5- Department of Anesthesia, Neyshabur University of Medical Sciences, Neyshabur, Iran.
6- Department of Psychiatric Nursing, Neyshabur University of Medical Sciences, Neyshabur, Iran.
2- Department of Anesthesia, Neyshabur University of Medical Sciences, Neyshabur, iran
3- Department of Nursing, Neyshabur, University of Medical Sciences, Neyshabur, Iran ,
4- School of Nursing, Faculty of Science, Medicine and Health, University of Wollongong, South Western Sydney Campus, Australia
5- Department of Anesthesia, Neyshabur University of Medical Sciences, Neyshabur, Iran.
6- Department of Psychiatric Nursing, Neyshabur University of Medical Sciences, Neyshabur, Iran.
Full-Text [PDF 643 kb]
(89 Downloads)
| Abstract (HTML) (220 Views)
Full-Text: (57 Views)
Abstract
Background & Objective: Nursing students often experience psychological distress, which can negatively affect their academic performance and well-being. Effective interventions that build resilience and self-efficacy are needed. Henderson's resilience model, which highlights the role of educational quality in fostering resilience, offers a useful framework. This study aimed to assess whether Henderson's resilience model could reduce psychological distress and improve academic self-efficacy and resilience in nursing students..
Materials & Methods: We carried out a single-blind (assessor-blinded) randomized controlled trial with 36 nursing students, who were stratified into intervention (n = 18) and control (n = 18) groups. After attrition (three withdrawals, one incomplete questionnaire), the final sample included 17 students in the intervention group and 15–16 in the control group. Outcomes were measured using the Nursing Student Academic Resilience Inventory, the College Academic Self-Efficacy Scale, and the Depression Anxiety Stress Scale. Data were analyzed using paired and independent t-tests (with Welch's correction where needed) and chi-square tests in SPSS version 18.
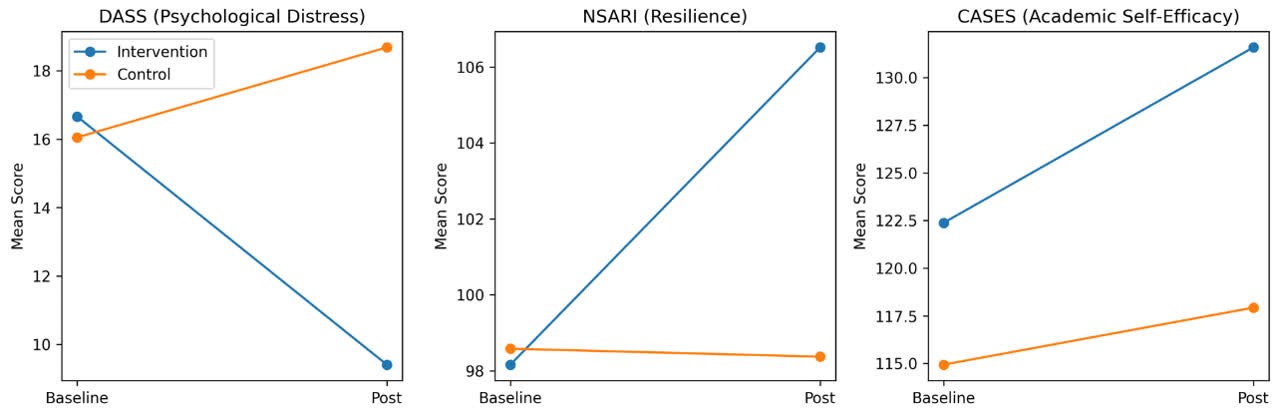
Results: Baseline scores did not differ significantly between groups. At post-test, the intervention group showed significantly lower psychological distress (DASS mean difference = -9.27, 95% CI = -15.88 to -2.66; Welch's t = -2.900, df = 22.91, p = 0.008; Cohen's d = 1.03) and higher resilience (NSARI mean difference = +8.15, 95% CI = 1.35 to 14.95; Welch's t = 2.446, df = 30.02, p = 0.021; Cohen's d = 0.85). Academic self-efficacy also improved significantly in the intervention group (CASES mean difference = +13.65, 95% CI = 2.61 to 24.69; Welch's t = 2.525, df = 29.96, p = 0.017; Cohen's d = 0.88).
Conclusion: In this study, a structured 10‑week program based on Henderson's resilience model was associated with reduced psychological distress and improved resilience and academic self‑efficacy among nursing students. Larger, multi‑site trials with longer follow‑up are recommended to confirm these findings.
Introduction
Nursing students often experience high levels of psychological distress during their education [1]. According to a systematic review and meta-analysis, the prevalence of psychological distress among Asian nursing students is about 43% to 56% [2]. In Iran, several studies have shown that nursing students face various stressors, including poor communication, unclear training goals, fear of infectious diseases, academic burnout, difficulties in providing care, and dissatisfaction with their field of study [1, 3]. More recent findings also suggest that many students believe their academic performance was negatively affected by the COVID-19 pandemic [4, 5].
To help nursing students manage psychological distress and build clinical competence, effective strategies should be introduced early in their education [6]. Previous interventions—including cognitive behavioral therapy, mindfulness-based cognitive therapy, self-healing qigong, and electro-acupuncture—have been shown to reduce psychological distress [7–9]. However, few of these interventions focus on building personal strengths [6], whereas approaches that encourage positive emotions, constructive behaviors, and supportive social interactions may be more engaging and effective for students.
In positive psychology, resilience is a key concept for understanding how students adapt to educational challenges [10]. It is seen as a valuable way to help nursing students overcome difficulties and prepare for their professional roles [10]. Among healthcare professionals, resilience is widely viewed as essential for managing stress and improving well‑being [11]. As a result, it is considered a key component of nursing education—for both students and practicing nurses [12].
Research suggests that building psychological resilience among nursing students can improve educational outcomes, increase retention rates, and enhance the quality of patient care [13–15]. Ghods et al. [1] also recommended that educational leaders use resilience‑enhancing strategies to reduce professional burnout among nursing students. In addition, a recent literature review on resilience highlighted self‑efficacy as a key characteristic of resilient behavior in this population [10, 12].
Academic self‑efficacy refers to students' belief in their ability to successfully complete their educational program [16]. Evidence indicates a positive link between self‑efficacy and resilience in nursing students [17]. Moreover, prior studies have shown that self‑efficacy is a strong predictor of academic performance, ability to cope with educational challenges [18, 19], clinical performance, and psychological health [17]. Self‑efficacy is therefore seen as a key factor underlying different levels of resilience [10]. Cuartero et al. [20] also reported that higher resilience is associated with greater self‑efficacy, suggesting that boosting resilience may improve academic self‑efficacy in nursing students.
Among the various theoretical frameworks developed to build resilience [21, 22], Henderson's model focuses specifically on the quality of education. This framework highlights the importance of improving the educational environment, encouraging equality, and helping students gain the life skills and competencies needed for continuous learning. When these elements are strengthened, they serve as environmental protective factors for students [23].
Henderson's resilience model has been tested in various settings, such as industrial employment [24, 25]. However, studies looking at its impact on academic self‑efficacy and psychological distress among nursing students remain limited. To our knowledge, only a few investigations [26–28] have examined the effects of this model in nursing contexts. Moreover, empirical evidence on its effectiveness in academic settings is still limited, pointing to the need for further research [29].
While several resilience models exist—such as the Connor–Davidson framework [30] and the Penn Resilience Program [31]—Henderson's model is unique in its focus on educational quality and environmental protective factors [23]. Unlike individual-focused interventions, Henderson's approach targets the educational context itself, making it particularly suitable for nursing programs where systemic changes can help multiple student cohorts [32]. However, evidence of its effectiveness in nursing education remains limited.
Given the high prevalence of psychological distress among nursing students and the limitations of current interventions—which mainly focus on symptom reduction—there is a need for approaches that build resilience, self‑efficacy, and adaptive coping at the same time. Therefore, the present study aimed to assess whether Henderson's resilience model could reduce psychological distress and improve self‑efficacy and resilience in nursing students.
Materials & Methods
Design and setting(s)
This study was a single-blind (assessor-blinded), parallel‑group randomized controlled trial with a pre‑ and post‑test design. Participants were randomly allocated to either the intervention (Henderson's resilience program) or the waitlist control group. The trial was registered in the Iranian Registry of Clinical Trials (IRCT20160825029520N5), and sampling started after getting the IRCT registration code. The study was conducted between 2022-10-12 and 2022-12-21.
Participants and sampling
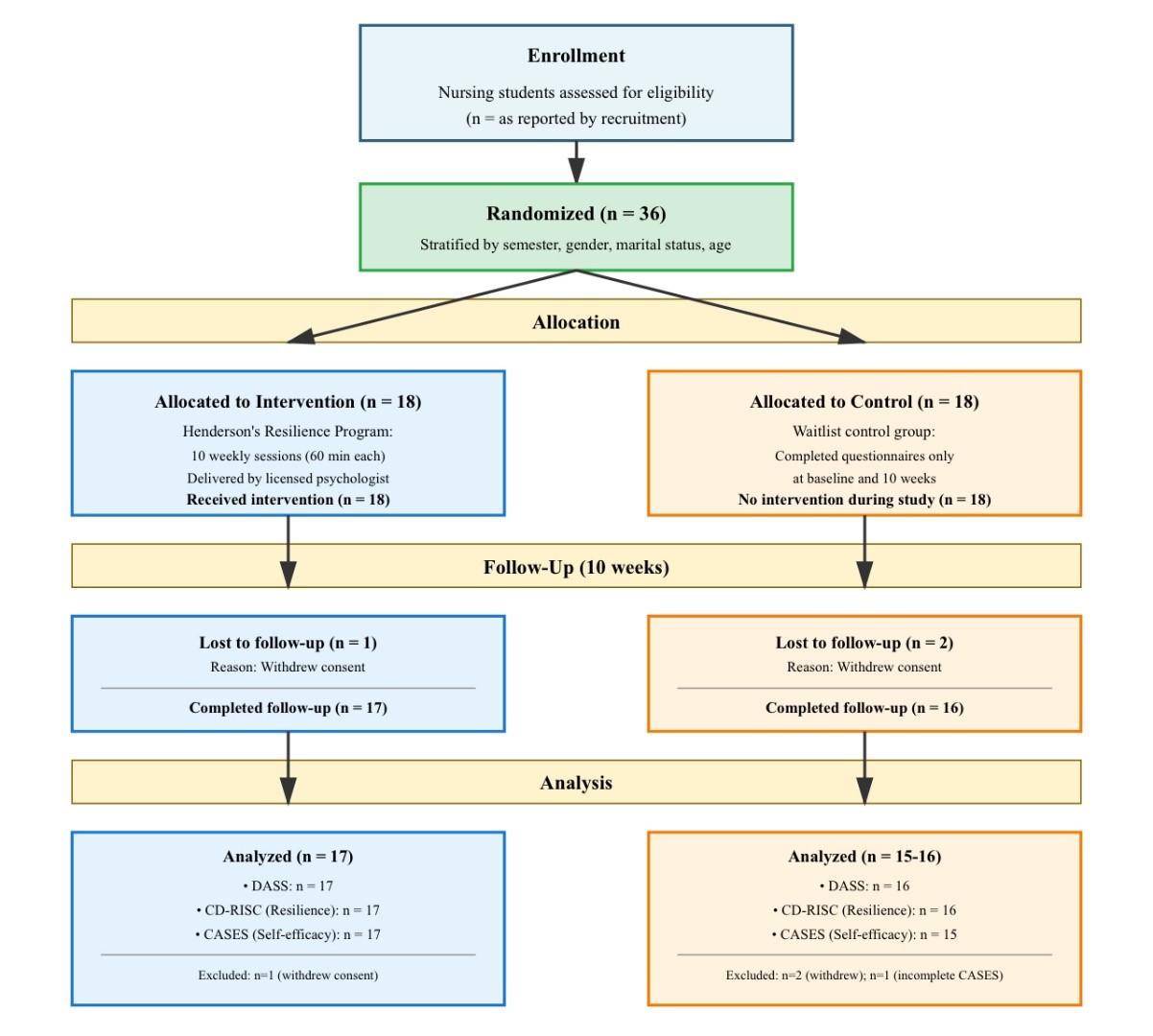
Participants were recruited from nursing students at Neyshabur University of Medical Sciences through university announcements and social media. Students who showed interest were screened for eligibility. Inclusion criteria were: (1) being a current nursing student, (2) willingness to participate, and (3) no severe depression or anxiety. Exclusion criteria were: (1) guest students from other universities, (2) history of major psychiatric disorders, and (3) prior participation in resilience‑related training within the past year. These criteria were chosen to ensure participant safety, sample homogeneity, and methodological validity. A total of 36 students were enrolled and randomly assigned to either the intervention (n = 18) or control (n = 18) group. Stratified randomization was carried out based on semester, gender, marital status, and age to ensure balanced distribution of key variables across groups. Within each stratum, the allocation sequence was generated using a computer‑generated random number list in Microsoft Excel. Allocation concealment was done using sequentially numbered, sealed, opaque envelopes prepared by an independent researcher who was not part of participant recruitment, intervention delivery, or data analysis. The research assistant in charge of enrolling participants opened the corresponding envelope only after baseline assessments were completed, so group assignment remained concealed until allocation. Because the nature of the intervention made it impossible to blind participants, the study used an assessor‑blinded design. Outcome assessors and data analysts were kept unaware of group assignments throughout the study. The intervention group took part in Henderson's resilience program [33], which included ten 60‑minute weekly sessions led by a licensed psychologist trained in resilience‑based interventions. The program covered self‑awareness, self‑esteem, communication skills, goal‑setting, decision‑making, problem‑solving, responsibility, anxiety management, spirituality, and recognition of risk and protective factors. Interactive methods such as lectures, discussions, brainstorming, storytelling, and role‑play were used. Fidelity was maintained through a structured manual and regular supervision by a senior clinical psychologist. Adherence to the protocol was tracked using attendance records and session supervision. The control group was placed on a waitlist, completed the same questionnaires at baseline and after 10 weeks, and later received one psychological session for ethical reasons. Sample size was calculated based on a conceptually similar psychological skills training study in university students [34]. With a 95% confidence interval (0.45–1.00), SD = 0.5, and effect size d = 0.73, and considering α = 0.05 and power = 80%, the minimum sample per group was 15. To account for possible attrition, 18 participants were recruited per group, giving a total of 36 students. During the 10-week follow-up, one participant in the intervention group (5.6%) withdrew consent and was excluded from all outcome analyses. In the control group, two participants (11.1%) withdrew during follow-up, and one additional participant did not complete the CASES questionnaire. As a result, the final sample for analysis was 𝑛 = 17 for the intervention group (all outcomes), 𝑛 = 16 for the control group (DASS-21 and NSARI), and
𝑛 = 15 for the control group (CASES). All exclusions occurred after randomization for reasons unrelated to the intervention, so a per-protocol analysis was carried out. Figure 1 shows the participant flow and reasons for attrition in a CONSORT diagram.
Tools/Instruments
Outcomes were measured using three validated instruments. A summary of each tool is provided below, and further details are available in the referenced sources.
1. Nursing Student Academic Resilience Inventory: The NSARI is a 24‑item scale that measures academic resilience in nursing students. Each item is rated on a 5‑point Likert scale ranging from 1 (compeletely disagree) to 5 (compeletly agree). Total scores range from 1 to 120 with higher scores indicating greater resilience. The NSARI has been designed and validated in Iranian nursing student, with reported Cronbach's α range of 0.63 to 0.78 [35].
2. College Academic Self‑Efficacy Scale (CASES): The CASES consists of 33 items assessing students’ beliefs in their academic capabilities. Items are scored on a 5-point Likert scale, with anchors ranging from 1 = very little to 5 = very much. Total scores range from 33 to 165, and higher scores reflect stronger academic self-efficacy. The Persian version of the CASES has demonstrated acceptable internal consistency in previous studies, with Cronbach’s 𝛼 values reported to be highly reliable (e.g., 𝛼 = 0.91) [36–38].
3. Depression Anxiety Stress Scale (DASS‑21): The DASS-21 is a 21-item instrument designed to measure negative emotional states across three subscales: depression, anxiety, and stress. Each item is rated on a 4-point Likert scale from 0 (never) to 3 (all of the time). Scores for each subscale are summed and multiplied by 2, with possible subscale scores ranging from 0 to 84. Higher scores indicate greater psychological distress. The Persian version of the DASS-21 has shown strong psychometric properties, with Cronbach’sα
Data were collected at baseline (pre‑intervention) and again after the 10‑week intervention period (post‑intervention).
Data collection methods
Data were collected at two time points: at first week (pre-test) and after the intervention (post‑test, week 10). All questionnaires were administered in a quiet classroom at the university in paper‑and‑pencil format. Participants completed the questionnaires individually in the presence of a research assistant, who provided standardized instructions and answered any questions. Completion time for the full set of questionnaires was approximately 20 minutes . To ensure confidentiality, participants placed completed questionnaires in sealed envelopes before returning them to the research assistant. Data were checked for completeness at the time of collection, and participants were asked to complete any missing items if they wished. No incentives were offered for participation.
Data analysis
Data were analyzed using Statistical Package for Social Sciences (SPSS) version 18. Descriptive statistics (mean, standard deviation, frequency, and percentage) were reported for all variables. The normality of continuous variables was checked using the Kolmogorov–Smirnov test, and homogeneity of variance was tested using Levene's test. Inferential analyses included paired‑samples t‑tests for within‑group comparisons (pre‑ to post‑test changes) and independent‑samples t‑tests for between‑group comparisons at post‑test. Where Levene's test showed unequal variances between groups, Welch's correction was used. Chi‑square tests (or Fisher's exact test when expected cell counts were < 5) were used for categorical variables. Effect sizes and 95% confidence intervals were calculated for all main outcomes.
Results
A total of 36 nursing students were enrolled and randomized; 18 were allocated to the Henderson resilience program (intervention) and 18 to the waitlist control group. A few participants had missing data at post-test. Baseline demographic characteristics did not differ significantly between groups (sex:
As shown in Figure 1, among the 36 randomized participants, three withdrew consent during follow-up (intervention:

Note: Chi-square tests were used for categorical variables and independent t-tests for age comparisons. Fisher’s exact test was applied where expected cell counts were less than 5 (i.e., Marital status).
Abbreviations: n, number of participants; SD, standard deviation; χ², Chi-square test; EFT, Fisher’s exact test; t, independent t-test; p, probability value.

Note: Between-group comparisons were performed using independent t-tests with Welch's correction where Levene's test indicated unequal variances. Mean difference represents intervention minus control. Cohen's d was calculated using pooled standard deviation. Statistical significance was set at p < 0.05.
Abbreviations: DASS, depression anxiety stress scale; NSARI, Nursing Student Academic Resilience Inventory; CASES, college academic self-efficacy scale; n, number of participants; SD, standard deviation; CI, confidence interval; t, Welch's t-test statistic; df, degrees of freedom; p, probability value.
Discussion
The aim of this study was to assess whether Henderson's resilience model could reduce psychological distress and improve self‑efficacy and resilience among nursing students. Our findings showed that the intervention significantly improved academic self‑efficacy and resilience while reducing psychological distress. These results are consistent with previous research showing the benefits of positive psychology‑based interventions [6, 26]. The findings also suggest that resilience may help nursing students adapt to stressful environments in both education and practice [10, 11, 40, 41], although larger studies are needed to confirm this relationship.
The observed improvements in self‑efficacy in the intervention group are consistent with findings from Peng et al. [42], who showed that resilience training improved medical students' confidence in their academic abilities. These results also align with recent meta‑analytic evidence on resilience interventions in higher education students [43]. However, direct comparisons should be made cautiously given differences in sample characteristics, intervention duration, and outcome measures across studies. Similarly, Akbari [26] reported that resilience‑based interventions reduced aggression and increased happiness among nursing students. Together, these findings suggest that resilience training may not only improve mental health but also support professional growth and academic performance in students. The positive effects of Henderson's resilience model may be explained by several mechanisms, including goal‑setting, problem‑solving, recognition of strengths, and realistic self‑evaluation. These strategies may help students regulate their emotions, use adaptive coping, and build greater confidence when facing academic challenges [44, 45]. However, our study did not directly test these mediating pathways. Future research should include qualitative feedback from participants or mediation analyses to better explain how resilience training works.This study has several limitations. First, the sample size was relatively small and taken from a single institution, limiting the generalizability of the findings. Second, due to sample attrition and incomplete questionnaires, the analyses were carried out per‑protocol rather than intention‑to‑treat, which may slightly overestimate intervention effects. Third, the study did not include long‑term follow‑up; therefore, the durability of the observed improvements remains unknown. Finally, mediators and process variables were not measured, limiting conclusions about the mechanisms behind changes in resilience and self‑efficacy.
Conclusion
This pilot randomized controlled trial provides preliminary evidence that Henderson's resilience model may help reduce psychological distress and improve resilience and academic self‑efficacy in nursing students. These findings suggest that resilience‑based educational interventions could support students in managing academic and professional demands. However, broader claims about integrating this model into nursing curricula should be made cautiously. Future research should use larger, multi‑site samples, apply Intention-to-Treat analyses, include follow‑up assessments, and evaluate potential mediators to better understand how resilience interventions work. Longitudinal studies and cost‑effectiveness analyses are also recommended before
large‑scale implementation.
Ethical considerations
The study protocol was approved by the Ethics Committee of Neyshabur University of Medical Sciences (Approval Code: IR.NUMS.REC.1401.022). Written informed consent was got from all participants before enrollment. Participation was voluntary, responses were confidential, and students could withdraw at any time without any penalty.
Artificial intelligence utilization for article writing
This manuscript was prepared without the direct use of generative artificial intelligence tools for writing or editing. AI‑based software was only used for language editing and grammar checking. All content, interpretations, and conclusions were developed by the authors. The authors followed ethical guidelines for the responsible use of AI in academic writing.
Acknowledgment
The authors would like to thank the nursing students who participated in this study for their time and commitment. They are also grateful for the funding of this study, provided by Neyshabur University of Medical Sciences.
Conflict of interest statement
The authors declare that there is no conflict of interest related to this paper.
Author contributions
HJ and SA conceptualized and designed the study; SA collected and curated data; AF performed the study and visualization; all authors added to writing, reviewing, editing, and validation, with HJ supervising.
Funding
This study was supported by Neyshabur University of Medical Sciences. No external funding or special equipment was received.
Data availability statement
The datasets generated and analyzed during the current study are available from the corresponding author upon reasonable request.
Background & Objective: Nursing students often experience psychological distress, which can negatively affect their academic performance and well-being. Effective interventions that build resilience and self-efficacy are needed. Henderson's resilience model, which highlights the role of educational quality in fostering resilience, offers a useful framework. This study aimed to assess whether Henderson's resilience model could reduce psychological distress and improve academic self-efficacy and resilience in nursing students..
Materials & Methods: We carried out a single-blind (assessor-blinded) randomized controlled trial with 36 nursing students, who were stratified into intervention (n = 18) and control (n = 18) groups. After attrition (three withdrawals, one incomplete questionnaire), the final sample included 17 students in the intervention group and 15–16 in the control group. Outcomes were measured using the Nursing Student Academic Resilience Inventory, the College Academic Self-Efficacy Scale, and the Depression Anxiety Stress Scale. Data were analyzed using paired and independent t-tests (with Welch's correction where needed) and chi-square tests in SPSS version 18.
Results: Baseline scores did not differ significantly between groups. At post-test, the intervention group showed significantly lower psychological distress (DASS mean difference = -9.27, 95% CI = -15.88 to -2.66; Welch's t = -2.900, df = 22.91, p = 0.008; Cohen's d = 1.03) and higher resilience (NSARI mean difference = +8.15, 95% CI = 1.35 to 14.95; Welch's t = 2.446, df = 30.02, p = 0.021; Cohen's d = 0.85). Academic self-efficacy also improved significantly in the intervention group (CASES mean difference = +13.65, 95% CI = 2.61 to 24.69; Welch's t = 2.525, df = 29.96, p = 0.017; Cohen's d = 0.88).
Conclusion: In this study, a structured 10‑week program based on Henderson's resilience model was associated with reduced psychological distress and improved resilience and academic self‑efficacy among nursing students. Larger, multi‑site trials with longer follow‑up are recommended to confirm these findings.
Introduction
To help nursing students manage psychological distress and build clinical competence, effective strategies should be introduced early in their education [6]. Previous interventions—including cognitive behavioral therapy, mindfulness-based cognitive therapy, self-healing qigong, and electro-acupuncture—have been shown to reduce psychological distress [7–9]. However, few of these interventions focus on building personal strengths [6], whereas approaches that encourage positive emotions, constructive behaviors, and supportive social interactions may be more engaging and effective for students.
In positive psychology, resilience is a key concept for understanding how students adapt to educational challenges [10]. It is seen as a valuable way to help nursing students overcome difficulties and prepare for their professional roles [10]. Among healthcare professionals, resilience is widely viewed as essential for managing stress and improving well‑being [11]. As a result, it is considered a key component of nursing education—for both students and practicing nurses [12].
Research suggests that building psychological resilience among nursing students can improve educational outcomes, increase retention rates, and enhance the quality of patient care [13–15]. Ghods et al. [1] also recommended that educational leaders use resilience‑enhancing strategies to reduce professional burnout among nursing students. In addition, a recent literature review on resilience highlighted self‑efficacy as a key characteristic of resilient behavior in this population [10, 12].
Academic self‑efficacy refers to students' belief in their ability to successfully complete their educational program [16]. Evidence indicates a positive link between self‑efficacy and resilience in nursing students [17]. Moreover, prior studies have shown that self‑efficacy is a strong predictor of academic performance, ability to cope with educational challenges [18, 19], clinical performance, and psychological health [17]. Self‑efficacy is therefore seen as a key factor underlying different levels of resilience [10]. Cuartero et al. [20] also reported that higher resilience is associated with greater self‑efficacy, suggesting that boosting resilience may improve academic self‑efficacy in nursing students.
Among the various theoretical frameworks developed to build resilience [21, 22], Henderson's model focuses specifically on the quality of education. This framework highlights the importance of improving the educational environment, encouraging equality, and helping students gain the life skills and competencies needed for continuous learning. When these elements are strengthened, they serve as environmental protective factors for students [23].
Henderson's resilience model has been tested in various settings, such as industrial employment [24, 25]. However, studies looking at its impact on academic self‑efficacy and psychological distress among nursing students remain limited. To our knowledge, only a few investigations [26–28] have examined the effects of this model in nursing contexts. Moreover, empirical evidence on its effectiveness in academic settings is still limited, pointing to the need for further research [29].
While several resilience models exist—such as the Connor–Davidson framework [30] and the Penn Resilience Program [31]—Henderson's model is unique in its focus on educational quality and environmental protective factors [23]. Unlike individual-focused interventions, Henderson's approach targets the educational context itself, making it particularly suitable for nursing programs where systemic changes can help multiple student cohorts [32]. However, evidence of its effectiveness in nursing education remains limited.
Given the high prevalence of psychological distress among nursing students and the limitations of current interventions—which mainly focus on symptom reduction—there is a need for approaches that build resilience, self‑efficacy, and adaptive coping at the same time. Therefore, the present study aimed to assess whether Henderson's resilience model could reduce psychological distress and improve self‑efficacy and resilience in nursing students.
Materials & Methods
Design and setting(s)
This study was a single-blind (assessor-blinded), parallel‑group randomized controlled trial with a pre‑ and post‑test design. Participants were randomly allocated to either the intervention (Henderson's resilience program) or the waitlist control group. The trial was registered in the Iranian Registry of Clinical Trials (IRCT20160825029520N5), and sampling started after getting the IRCT registration code. The study was conducted between 2022-10-12 and 2022-12-21.
Participants and sampling
Participants were recruited from nursing students at Neyshabur University of Medical Sciences through university announcements and social media. Students who showed interest were screened for eligibility. Inclusion criteria were: (1) being a current nursing student, (2) willingness to participate, and (3) no severe depression or anxiety. Exclusion criteria were: (1) guest students from other universities, (2) history of major psychiatric disorders, and (3) prior participation in resilience‑related training within the past year. These criteria were chosen to ensure participant safety, sample homogeneity, and methodological validity. A total of 36 students were enrolled and randomly assigned to either the intervention (n = 18) or control (n = 18) group. Stratified randomization was carried out based on semester, gender, marital status, and age to ensure balanced distribution of key variables across groups. Within each stratum, the allocation sequence was generated using a computer‑generated random number list in Microsoft Excel. Allocation concealment was done using sequentially numbered, sealed, opaque envelopes prepared by an independent researcher who was not part of participant recruitment, intervention delivery, or data analysis. The research assistant in charge of enrolling participants opened the corresponding envelope only after baseline assessments were completed, so group assignment remained concealed until allocation. Because the nature of the intervention made it impossible to blind participants, the study used an assessor‑blinded design. Outcome assessors and data analysts were kept unaware of group assignments throughout the study. The intervention group took part in Henderson's resilience program [33], which included ten 60‑minute weekly sessions led by a licensed psychologist trained in resilience‑based interventions. The program covered self‑awareness, self‑esteem, communication skills, goal‑setting, decision‑making, problem‑solving, responsibility, anxiety management, spirituality, and recognition of risk and protective factors. Interactive methods such as lectures, discussions, brainstorming, storytelling, and role‑play were used. Fidelity was maintained through a structured manual and regular supervision by a senior clinical psychologist. Adherence to the protocol was tracked using attendance records and session supervision. The control group was placed on a waitlist, completed the same questionnaires at baseline and after 10 weeks, and later received one psychological session for ethical reasons. Sample size was calculated based on a conceptually similar psychological skills training study in university students [34]. With a 95% confidence interval (0.45–1.00), SD = 0.5, and effect size d = 0.73, and considering α = 0.05 and power = 80%, the minimum sample per group was 15. To account for possible attrition, 18 participants were recruited per group, giving a total of 36 students. During the 10-week follow-up, one participant in the intervention group (5.6%) withdrew consent and was excluded from all outcome analyses. In the control group, two participants (11.1%) withdrew during follow-up, and one additional participant did not complete the CASES questionnaire. As a result, the final sample for analysis was 𝑛 = 17 for the intervention group (all outcomes), 𝑛 = 16 for the control group (DASS-21 and NSARI), and
𝑛 = 15 for the control group (CASES). All exclusions occurred after randomization for reasons unrelated to the intervention, so a per-protocol analysis was carried out. Figure 1 shows the participant flow and reasons for attrition in a CONSORT diagram.
Tools/Instruments
Outcomes were measured using three validated instruments. A summary of each tool is provided below, and further details are available in the referenced sources.
1. Nursing Student Academic Resilience Inventory: The NSARI is a 24‑item scale that measures academic resilience in nursing students. Each item is rated on a 5‑point Likert scale ranging from 1 (compeletely disagree) to 5 (compeletly agree). Total scores range from 1 to 120 with higher scores indicating greater resilience. The NSARI has been designed and validated in Iranian nursing student, with reported Cronbach's α range of 0.63 to 0.78 [35].
2. College Academic Self‑Efficacy Scale (CASES): The CASES consists of 33 items assessing students’ beliefs in their academic capabilities. Items are scored on a 5-point Likert scale, with anchors ranging from 1 = very little to 5 = very much. Total scores range from 33 to 165, and higher scores reflect stronger academic self-efficacy. The Persian version of the CASES has demonstrated acceptable internal consistency in previous studies, with Cronbach’s 𝛼 values reported to be highly reliable (e.g., 𝛼 = 0.91) [36–38].
3. Depression Anxiety Stress Scale (DASS‑21): The DASS-21 is a 21-item instrument designed to measure negative emotional states across three subscales: depression, anxiety, and stress. Each item is rated on a 4-point Likert scale from 0 (never) to 3 (all of the time). Scores for each subscale are summed and multiplied by 2, with possible subscale scores ranging from 0 to 84. Higher scores indicate greater psychological distress. The Persian version of the DASS-21 has shown strong psychometric properties, with Cronbach’s
Data were collected at baseline (pre‑intervention) and again after the 10‑week intervention period (post‑intervention).
Data collection methods
Data were collected at two time points: at first week (pre-test) and after the intervention (post‑test, week 10). All questionnaires were administered in a quiet classroom at the university in paper‑and‑pencil format. Participants completed the questionnaires individually in the presence of a research assistant, who provided standardized instructions and answered any questions. Completion time for the full set of questionnaires was approximately 20 minutes . To ensure confidentiality, participants placed completed questionnaires in sealed envelopes before returning them to the research assistant. Data were checked for completeness at the time of collection, and participants were asked to complete any missing items if they wished. No incentives were offered for participation.
Data analysis
Data were analyzed using Statistical Package for Social Sciences (SPSS) version 18. Descriptive statistics (mean, standard deviation, frequency, and percentage) were reported for all variables. The normality of continuous variables was checked using the Kolmogorov–Smirnov test, and homogeneity of variance was tested using Levene's test. Inferential analyses included paired‑samples t‑tests for within‑group comparisons (pre‑ to post‑test changes) and independent‑samples t‑tests for between‑group comparisons at post‑test. Where Levene's test showed unequal variances between groups, Welch's correction was used. Chi‑square tests (or Fisher's exact test when expected cell counts were < 5) were used for categorical variables. Effect sizes and 95% confidence intervals were calculated for all main outcomes.
Results
A total of 36 nursing students were enrolled and randomized; 18 were allocated to the Henderson resilience program (intervention) and 18 to the waitlist control group. A few participants had missing data at post-test. Baseline demographic characteristics did not differ significantly between groups (sex:
As shown in Figure 1, among the 36 randomized participants, three withdrew consent during follow-up (intervention:
Note: Chi-square tests were used for categorical variables and independent t-tests for age comparisons. Fisher’s exact test was applied where expected cell counts were less than 5 (i.e., Marital status).
Abbreviations: n, number of participants; SD, standard deviation; χ², Chi-square test; EFT, Fisher’s exact test; t, independent t-test; p, probability value.
Figure 1. Flow chart illustrating how to select, and randomize participants.
Specifically, post-intervention psychological distress was significantly lower in the intervention group compared to the control group (mean difference = -9.27, 95% CI = -15.88 to -2.66; Welch’s
Table 2. Pre- and post-intervention scores (mean ± SD) and between-group comparisonsNote: Between-group comparisons were performed using independent t-tests with Welch's correction where Levene's test indicated unequal variances. Mean difference represents intervention minus control. Cohen's d was calculated using pooled standard deviation. Statistical significance was set at p < 0.05.
Abbreviations: DASS, depression anxiety stress scale; NSARI, Nursing Student Academic Resilience Inventory; CASES, college academic self-efficacy scale; n, number of participants; SD, standard deviation; CI, confidence interval; t, Welch's t-test statistic; df, degrees of freedom; p, probability value.
Figure 2. Changes in psychological distress (DASS‑21), resilience (NSARI), and academic self‑efficacy (CASES) from pre‑test to post‑test in the intervention and control groups.
Discussion
The aim of this study was to assess whether Henderson's resilience model could reduce psychological distress and improve self‑efficacy and resilience among nursing students. Our findings showed that the intervention significantly improved academic self‑efficacy and resilience while reducing psychological distress. These results are consistent with previous research showing the benefits of positive psychology‑based interventions [6, 26]. The findings also suggest that resilience may help nursing students adapt to stressful environments in both education and practice [10, 11, 40, 41], although larger studies are needed to confirm this relationship.
The observed improvements in self‑efficacy in the intervention group are consistent with findings from Peng et al. [42], who showed that resilience training improved medical students' confidence in their academic abilities. These results also align with recent meta‑analytic evidence on resilience interventions in higher education students [43]. However, direct comparisons should be made cautiously given differences in sample characteristics, intervention duration, and outcome measures across studies. Similarly, Akbari [26] reported that resilience‑based interventions reduced aggression and increased happiness among nursing students. Together, these findings suggest that resilience training may not only improve mental health but also support professional growth and academic performance in students. The positive effects of Henderson's resilience model may be explained by several mechanisms, including goal‑setting, problem‑solving, recognition of strengths, and realistic self‑evaluation. These strategies may help students regulate their emotions, use adaptive coping, and build greater confidence when facing academic challenges [44, 45]. However, our study did not directly test these mediating pathways. Future research should include qualitative feedback from participants or mediation analyses to better explain how resilience training works.This study has several limitations. First, the sample size was relatively small and taken from a single institution, limiting the generalizability of the findings. Second, due to sample attrition and incomplete questionnaires, the analyses were carried out per‑protocol rather than intention‑to‑treat, which may slightly overestimate intervention effects. Third, the study did not include long‑term follow‑up; therefore, the durability of the observed improvements remains unknown. Finally, mediators and process variables were not measured, limiting conclusions about the mechanisms behind changes in resilience and self‑efficacy.
Conclusion
This pilot randomized controlled trial provides preliminary evidence that Henderson's resilience model may help reduce psychological distress and improve resilience and academic self‑efficacy in nursing students. These findings suggest that resilience‑based educational interventions could support students in managing academic and professional demands. However, broader claims about integrating this model into nursing curricula should be made cautiously. Future research should use larger, multi‑site samples, apply Intention-to-Treat analyses, include follow‑up assessments, and evaluate potential mediators to better understand how resilience interventions work. Longitudinal studies and cost‑effectiveness analyses are also recommended before
large‑scale implementation.
Ethical considerations
The study protocol was approved by the Ethics Committee of Neyshabur University of Medical Sciences (Approval Code: IR.NUMS.REC.1401.022). Written informed consent was got from all participants before enrollment. Participation was voluntary, responses were confidential, and students could withdraw at any time without any penalty.
Artificial intelligence utilization for article writing
This manuscript was prepared without the direct use of generative artificial intelligence tools for writing or editing. AI‑based software was only used for language editing and grammar checking. All content, interpretations, and conclusions were developed by the authors. The authors followed ethical guidelines for the responsible use of AI in academic writing.
Acknowledgment
The authors would like to thank the nursing students who participated in this study for their time and commitment. They are also grateful for the funding of this study, provided by Neyshabur University of Medical Sciences.
Conflict of interest statement
The authors declare that there is no conflict of interest related to this paper.
Author contributions
HJ and SA conceptualized and designed the study; SA collected and curated data; AF performed the study and visualization; all authors added to writing, reviewing, editing, and validation, with HJ supervising.
Funding
This study was supported by Neyshabur University of Medical Sciences. No external funding or special equipment was received.
Data availability statement
The datasets generated and analyzed during the current study are available from the corresponding author upon reasonable request.
Article Type : Orginal Research |
Subject:
Medical Education
Received: 2025/09/17 | Accepted: 2026/02/22 | Published: 2026/04/1
Received: 2025/09/17 | Accepted: 2026/02/22 | Published: 2026/04/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
