
Sun, Feb 1, 2026
[Archive]
Volume 18, Issue 2 (2025)
J Med Edu Dev 2025, 18(2): 70-79 |
Back to browse issues page

Ethics code: ESUTHP/C-MAC/RA/034/158
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Tamunosiki Chinawa A, Onyia J, Ossai E, Nwokoye I, Nwankwo O, Nzeduba C et al . Clinical students' perception of acute rheumatic fever and knowledge of vaccine development in the future: A cross-sectional study among medical students in Enugu State, Nigeria. J Med Edu Dev 2025; 18 (2) :70-79
URL: http://edujournal.zums.ac.ir/article-1-2330-en.html
URL: http://edujournal.zums.ac.ir/article-1-2330-en.html
Awoere Tamunosiki Chinawa1  , Jude Onyia2 , Edmund Ossai3 , Ikenna Nwokoye3 , Ogonna Nwankwo4 , Chiesonu Nzeduba4 , Josephat Chinawa *5
, Jude Onyia2 , Edmund Ossai3 , Ikenna Nwokoye3 , Ogonna Nwankwo4 , Chiesonu Nzeduba4 , Josephat Chinawa *5
, Jude Onyia2 , Edmund Ossai3 , Ikenna Nwokoye3 , Ogonna Nwankwo4 , Chiesonu Nzeduba4 , Josephat Chinawa *5
1- Department of Community Medicine, College of medicine ESUT, Enugu, Enugu State, Nigeria
2- College of Medicine, UNN, Enugu
3- College of Medicine, FETA, Abakaliki
4- College of Medicine, ESUT, ENUGU
5- College of Medicine, UNN, Enugu ,josephat.chinawa@unn.edu.ng
2- College of Medicine, UNN, Enugu
3- College of Medicine, FETA, Abakaliki
4- College of Medicine, ESUT, ENUGU
5- College of Medicine, UNN, Enugu ,
Keywords: medical students, acute rheumatic fever, perception, curriculum, knowledge, medical school, vaccination.
Full-Text [PDF 400 kb]
(451 Downloads)
| Abstract (HTML) (1120 Views)
Full-Text: (130 Views)
Abstract
Background & Objective: Acute rheumatic fever (ARF) is a major public health issue among children with increased morbidity and mortality. This study aimed to explore clinical medical students' perceptions and awareness of ARF and the potential for developing a future vaccine, as well as to document the factors associated with these views.
Materials & Methods: This cross-sectional study was conducted in two medical schools in the Enugu metropolis from July 2024 to October 2024. The study enrolled 341 clinical medical students from two medical schools in Southeast Nigeria. Data were collected using a validated interviewer-administered questionnaire. The questionnaire included 11 variables to assess the students' ARF knowledge. The maximum obtainable mark for each respondent was 29. Knowledge of ARF vaccination was assessed using eight variables.
Results: Most respondents (93.0 %) demonstrated awareness of ARF. Just over half (50.7 %) recognized sore throat as a symptom of ARF. Fifty-one point-three per cent of respondents demonstrated good knowledge of ARF. Most respondents (86.8%) knew vaccination could be an effective preventive measure against the disease if available. Fourth-year respondents were five times less likely to possess good knowledge of ARF compared to their sixth-year counterparts, with an Adjusted Odds Ratio (AOR) of 0.2 (95% Confidence Interval [CI]: 0.1-0.5). Respondents under 25 years old were three times less likely to intend to receive the ARF vaccine compared to those 25 years old and above (AOR = 0.3; 95%, CI: 0.1-0.9).
Conclusion: A considerable number of medical students were aware of the development of the ARF vaccine. This serves as a strong call to incorporate the teaching of ARF into the curriculum at all levels of medical education.
Materials & Methods
Design and setting(s)
This was a cross-sectional study conducted in two medical schools in Southeast Nigeria from 14 March 2024 to 24 October 2024. It involved clinical medical students in their fourth to sixth year of study drawn from two South-eastern Nigerian medical schools: Ebonyi State University, Abakaliki, and Enugu State University of Science and Technology, Enugu.
Participants and sampling
Three hundred forty-one clinical medical students from two medical schools in Southeast Nigeria were enrolled consecutively in the study. The students were recruited consecutively until the sample size was reached. Medical students in the clinical class who provided informed consent were included in the study. In contrast, medical students in the pre-clinical class and those without consent were excluded from this study. A two-stage sampling technique was used to select the medical students for inclusion in the study. Six accredited medical schools in southeast Nigeria have clinical medical students. Two medical students were selected out of the six using a simple random sampling technique of balloting. In the second stage, a list of all medical students in the clinical classes (fourth year to sixth year) was made. On each day of data collection, the number of medical students in the three classes in each of the two selected schools who were present served as the sampling frame. The sampling interval was determined by dividing the total number by the sample size of 170, which represented the estimated number of students from each selected school who would participate in the study. Therefore, every medical student was recruited for the study based on the seating arrangement of the students in the three classes on each day of data collection. On each occasion, the index student was selected using a simple random sampling technique of balloting. The formula obtained the sample size: n = Z2pq ÷ d2 [15].
A minimum sample size of 347 students was obtained using the formula above.
Tools/Instruments
The study used a validated interviewer-administered questionnaire. Ray et al. [16] adapted this questionnaire using a group of students aged 10-16 randomly selected from different schools. The questionnaire covers questions on knowledge of ARF and willingness to be vaccinated, defined as the preparedness or readiness to receive a vaccine after considering the efficacy, benefits, adverse effects, and barriers associated with receiving such a vaccine [17]. Knowledge of ARF was assessed using 11 variables.
Five items focused on symptoms, with each correct response scoring one and incorrect response scoring 0. The other six variables for the ARF assessment focused on the disease's prevalence, the age group most likely to be affected, impact, diagnosis, treatment options and prevention of the disease. For these six variables, a correct answer by any respondent attracted four marks, while an incorrect answer was scored zero. Thus, the maximum obtainable mark for each respondent was 29. Knowledge of rheumatic fever vaccination was assessed using eight variables. Each correct response from the respondents attracted a score of one, while incorrect responses were scored zero. The maximum score each respondent could obtain is eight.
The questionnaire components related to socioeconomic status were developed using Principal Component Analysis (PCA) in STATA statistical software version 12. The eleven variables listed above served as inputs to the PCA. For the calculation of distribution cut points, quartiles were used. Each respondent was assigned the wealth index score of their family.
The quartiles were Q1 = Poorest, Q2 = The Very Poor, Q3 = The Poor, and Q4 = The Least Poor. The quartiles were further dichotomized into low socioeconomic class, comprising the poorest and very poor, and high socioeconomic class, comprising the poorest and least poor groups.
Cronbach's α was employed to assess the internal consistency of the questionnaire adapted from Ray et al. [18]. A score of 0.8 was achieved, indicating a satisfactory level of reliability. Additionally, Pearson's correlation coefficient was utilized to determine the test-retest reliability, with a score of 0.5 indicating a higher reliability.
Data collection methods
The questionnaires were distributed to the medical students during the didactic lecture period in the first and second semesters of the year of study.
Data analysis
Data entry and analysis were done using the Statistical Product and Service Solutions (IMB-SPSS) statistical software version 25. Continuous variables were represented using mean and standard deviation, while categorical variables were presented using frequencies and proportions. The mean knowledge score of ARF among the categories of independent variables was compared using the Student t-test when the groups were two and with analysis of variance if the groups were more than two.
The mean knowledge score of ARF vaccination among the categories of independent variables was compared using the Student t-test when the groups were two and with analysis of variance if the groups were more than two.
A p-value of <0.05 determined the level of statistical significance. A chi-square test and multivariate analysis through binary logistic regression were employed. Respondents who achieved a score of 50% or higher of the total possible score were considered to have good knowledge.
Results
Table 1 shows the socio-demographic characteristics of the respondents.
The mean ± SD of the age of the respondents was 24.3 ± 2.9 years. The highest proportion of the respondents, 67.2%, were under 25 years old, while the least proportion, 3.8%, were 30 years and above. A higher proportion of the respondents, 51.0%, were male. The majority of the respondents, 96.5%, were single. The highest proportion of the respondents, 64.2%, were in the fifth year of study, while the least proportion, 8.2%, were in the sixth year.
Table 1. Socio-demographic characteristics of respondents (n = 341)
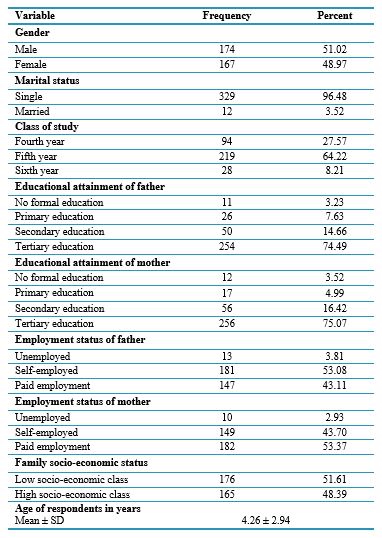
Abbreviation: SD, standard deviation.
Table 2 shows awareness of ARF and rheumatic fever vaccine among the respondents. The majority of the respondents, 93.0%, were aware of ARF. The major sources of information included health workers (82.3%), internet/social media (61.8%), and friends (42.3%). Less than one-fifth of the respondents, 17.9%, were aware of the ARF vaccine. The major sources of information on the ARF vaccine included health workers, 77.0%; internet/social media, 50.8%; and friends, 39.3%.
Table 2. Awareness of ARF and rheumatic fever vaccine among the respondents (n = 341)
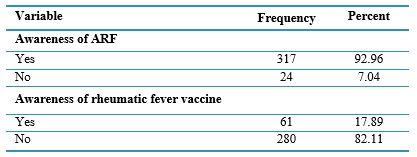
Note: Multiple responses encouraged.
Table 3 shows the respondents' knowledge of ARF and rheumatic fever vaccination. A higher proportion of the respondents, 88.9%, knew that shortness of breath is a symptom of rheumatic fever and rheumatic heart disease. A higher proportion of the respondents, 50.7%, knew that sore throat is a symptom of rheumatic fever. Most respondents, 56.0%, knew the age group 5-15 years were more likely to have rheumatic fever. A higher proportion of the respondents, 81.5%, knew that diagnosis is by history taking and past medical history of sore throat. The mean knowledge of ARF score was 14.8 ± 5.8. Most 86.8% of respondents knew vaccination could be a good measure to prevent diseases. The mean knowledge of ARF vaccination score was 4.5 ± 1.4. Less than half of the respondents, 45.7%, knew they were not in Nigeria's high-priority group for rheumatic fever vaccination. Less than one-tenth of the respondents, 8.5%, were aware of anyone who died from rheumatic fever. A minor proportion of the respondents, 5.6%, intend to receive vaccination for rheumatic fever when available. Table 4 shows the correlation matrix of variables, including the age of respondents, knowledge of ARF and knowledge of ARF vaccination. A very weak positive correlation existed between knowledge of ARF and rheumatic fever vaccination. Increases in ARF knowledge were associated with increases in ARF vaccination knowledge, and this relationship was statistically significant (n = 341, r = 0.141, p = 0.009). Table 5 and 6 compared mean scores of knowledge of ARF and
knowledge of ARF vaccination. The mean knowledge score of ARF was highest among the sixth-year students, 16.5 ± 5.9, and least among those in the fourth year, 11.6 ± 4.9, and the mean difference was statistically significant (F = 21.836, p < 0.001). The mean knowledge score for ARF was significantly higher among the respondents whose mothers had tertiary education, 15.1 ± 5.9 compared to those whose mothers had secondary education and below, 13.8 ± 5.1 (Student t = 1.990, p = 0.048). The mean knowledge score for ARF was higher among the respondents whose families were in the high socioeconomic class, 15.5 ± 5.6 compared to those in the low socioeconomic class. The mean difference was statistically significant (Student t = 2.374, p = 0.018). The mean knowledge score for rheumatic fever vaccination was significantly higher among respondents who perceived themselves as susceptible to ARF, with a score of 4.9 ± 1.2, compared to those who did not perceive themselves as susceptible, whose score was 4.4 ± 1.5 (Student t = 3.161, p = 0.002). The mean knowledge score for rheumatic fever vaccination was higher among the respondents who intend to receive rheumatic fever vaccination, 5.0 ± 1.3 when compared to those who did not intend to receive the vaccine, 4.4 ± 1.4 and the mean difference was found to be statistically significant, (Student t = 3.718, p < 0.001).
Table 3. Knowledge of ARF and rheumatic fever vaccination among the respondents (n = 341)
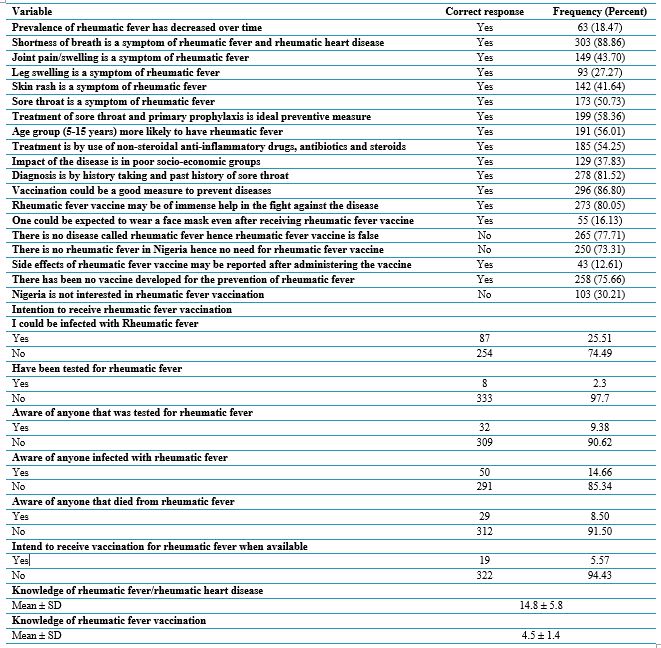
Abbreviation: SD, standard deviation.
Table 4. Correlation matrix of variables including age of respondents, knowledge of ARF and knowledge of rheumatic fever vaccination (n = 341)
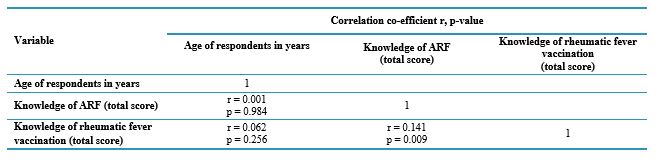
Abbreviations: r, correlation co-efficient; p-value, probability value.
Table 5. Comparison of mean scores of knowledge of ARF and knowledge of rheumatic fever vaccination (n = 341)
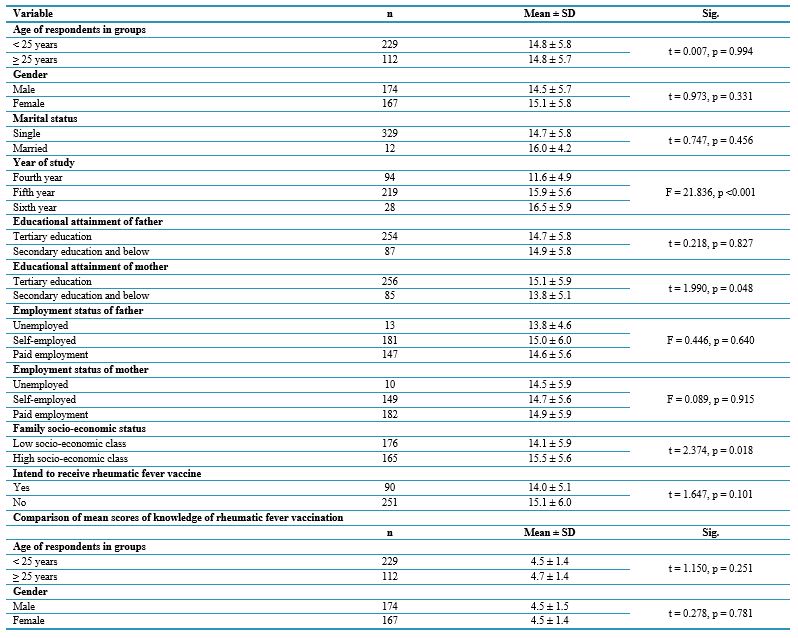
Abbreviations: t, t-test statistic; F, analysis of variance statistic; SD, standard deviation; n, number of participants; Sig., Significance; p, probability value.
Table 6. Comparison of mean scores of knowledge of ARF and knowledge of rheumatic fever vaccination (n = 341)
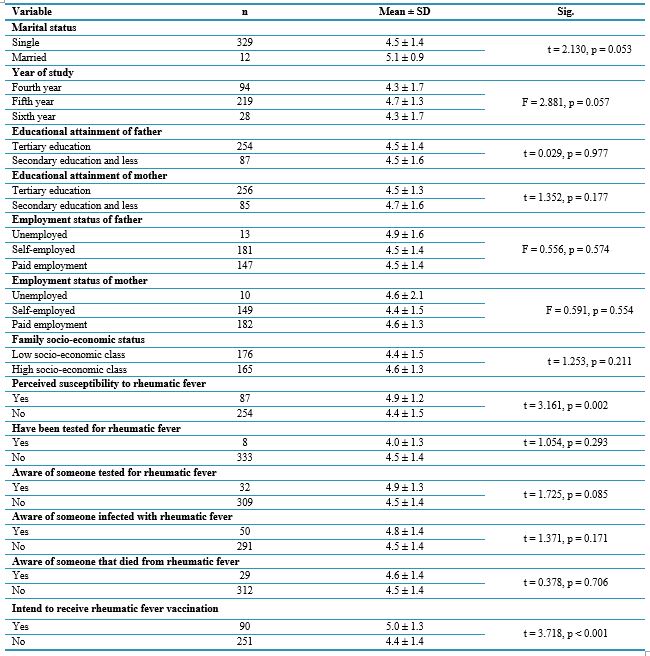
Abbreviations: t, t-test statistic; F, analysis of variance statistic; SD, standard deviation; n, number of participants; Sig., Significance; p, probability value.
Discussion
This study aimed to explore the perception and awareness of ARF among clinical medical students and to document associated factors. A high level of awareness (93.3%) was noted among medical students. This may be attributed to the fact that most information on ARF was derived from health professionals. The level of awareness of ARF among medical students was significantly higher than that reported by Alnemari et al. [18] in Saudi Arabia, where a level of awareness of 55.2 % was reported in students in the College of Medicine and 33.3% in the College of Dentistry, 44.8% in the College of Pharmacy, 21.4% in the college of applied Medical sciences and 45.9% among college of nursing students. The present study's findings were higher than those of Nkoke et al. [19] and Chelo et al. [20]. The variation in awareness of ARF may be attributed to the differing medical curricula employed by the participating medical schools, the year of study of the medical students involved, and potentially the methodologies used by the authors. The study also showed that 56% of medical students know that ARF commonly affects children between the ages of 5 and 15 years. Similarly, only 41.6% noted that skin rash could trigger ARF. This was also similar to the study of Fakieha et al. [21], where 54.8% of the subjects knew that children aged 5 to 15 years old are susceptible to ARF. The association between skin rash (bacterial dermatitis) and ARF was noted in 46.1% of the reportage of Fakieha et al. [21]
The current study noted no association between gender and the perception of ARF. However, Fakieha et al. [21] noted gender as the only important factor affecting knowledge of ARF in their study. Other studies noted that females have better knowledge than males [22-29].
The study noted that fewer medical students (50.7%) knew that sore throat was a symptom of ARF. Concerning the association between bacterial sore throat and ARF, Kulik et al. [25] noted that over 79.5% of their subjects were aware of the link between a sore throat and ARF, which was also similar to the study of Manase et al. [26] where 73.1% of health workers were aware of this relationship between sore throat and ARF [25]. This poor awareness of the association between sore throat and ARF highlights the need for specific training and potential curriculum revisions.
Though 93.0% of the clinical medical students were aware of ARF, only a minor population had good knowledge of ARF in terms of epidemiology, spread and management. This indicates a serious and urgent need to intensify the dissemination of information on the epidemiology and spread of the diseases, especially among clinical medical students. This information should also be introduced to pre-clinical medical students to curb the militating effects of this disease. Besides, information on primary and secondary prevention and disease awareness should be provided in the early years of medical school [30].
It is noted in this study that students who were in the 6th year of study had more knowledge of ARF than those in a lower class. It is expedient to introduce the lecture on the awareness and prevention of ARF in the introductory class of the medical school. This finding contrasts with those of other studies [28–30]. Furthermore, students from high socioeconomic classes had a higher knowledge of ARF than those from a lower economic class. This finding was at variance with Machluf et al. [31], who documented the association of ARF with lower socioeconomic classes. The study showed that a major proportion of medical students (81.5%) were well-informed about the rising prevalence of ARF. Some studies have documented a rising prevalence of ARF, with 300,000–500,000 new cases diagnosed annually and approximately 230,000 related deaths [31].
About half (54.3%) of the medical students in the current study noted that the management of ARF includes using non-steroidal anti-inflammatory drugs, antibiotics and steroids. Fakieha et al. [21] corroborated the same results when they noted that 56.5% of their subjects were aware of using antibiotics to manage sore throat. Interestingly,
the current study found that 75.7% of the medical students recognized the non-availability of rheumatic fever vaccine, yet 78.9% were aware of the ongoing effort to develop such a vaccine. This good level of awareness could be explained by the correlational matrix, which showed a positive correlation between knowledge of ARF and knowledge of rheumatic fever vaccination.
Conclusion
There is a poor perception of ARF's clinical correlates and management among clinical medical students. Many medical students are aware of the development of an ARF vaccine. This is a clarion call to add the teaching of ARF to the curriculum at all levels in the medical school. This could reduce the burden and complications associated with the disease. Vigorous campaigns and changes in medical curricula, which should include lectures on ARF across all levels of medical school, may significantly increase the perception and management of ARF among medical students [45].
Ethical considerations
This was obtained from the Research and Ethics Committee of Enugu State University Teaching Hospital (Parklane) Enugu, Nigeria. Additionally, verbal informed consent was obtained from the participating medical students of the studied medical schools. The study adhered to established ethical principles and institutional guidelines throughout. The code for the approved work was ESUTHP/C-MAC/RA/034/158.
Artificial intelligence utilization for article writing
Not applicable.
Acknowledgment
We are grateful to the research assistant, Nnamdi, who helped in data entry.
Conflict of interest statement
The authors declare that they have no competing interests.
Author contributions
MC, ATC, OCN, ENO, ICN, JTO, NOO, and CNO conceived and designed this study, while JMC helped with the critical revision of the article. JMC and ENO also did the Data analysis/interpretation. All authors have read and approved the manuscript.
Funding
No organization funded this study. The authors personally covered all expenses incurred during the study.
Data availability statement
Data are, however, available from the authors upon reasonable request and with permission of the corresponding author.
Background & Objective: Acute rheumatic fever (ARF) is a major public health issue among children with increased morbidity and mortality. This study aimed to explore clinical medical students' perceptions and awareness of ARF and the potential for developing a future vaccine, as well as to document the factors associated with these views.
Materials & Methods: This cross-sectional study was conducted in two medical schools in the Enugu metropolis from July 2024 to October 2024. The study enrolled 341 clinical medical students from two medical schools in Southeast Nigeria. Data were collected using a validated interviewer-administered questionnaire. The questionnaire included 11 variables to assess the students' ARF knowledge. The maximum obtainable mark for each respondent was 29. Knowledge of ARF vaccination was assessed using eight variables.
Results: Most respondents (93.0 %) demonstrated awareness of ARF. Just over half (50.7 %) recognized sore throat as a symptom of ARF. Fifty-one point-three per cent of respondents demonstrated good knowledge of ARF. Most respondents (86.8%) knew vaccination could be an effective preventive measure against the disease if available. Fourth-year respondents were five times less likely to possess good knowledge of ARF compared to their sixth-year counterparts, with an Adjusted Odds Ratio (AOR) of 0.2 (95% Confidence Interval [CI]: 0.1-0.5). Respondents under 25 years old were three times less likely to intend to receive the ARF vaccine compared to those 25 years old and above (AOR = 0.3; 95%, CI: 0.1-0.9).
Conclusion: A considerable number of medical students were aware of the development of the ARF vaccine. This serves as a strong call to incorporate the teaching of ARF into the curriculum at all levels of medical education.
Introduction
The incidence of cardiovascular diseases in children is increasing [1-4]. Acute Rheumatic Fever (ARF) is one of the acquired heart diseases with a global burden in Sub-Saharan Africa [1, 2]. Accurate documentation of the epidemiology of ARF and its clinical features in Africa will help to improve diagnosis and enhance secondary prevention [3, 4]. The prevalence of ARF has shown fluctuations over time [5-9]. For instance, over the last 2 decades, the global prevalence rate has increased, and it is projected that by 2030, the rate may increase to 559.88 per 100,000 people [5]. In North-Central Nigeria, ARF prevalence is 21.6 per 1000, with a male preponderance [6]. The morbidity and mortality associated with ARF in 2015 were estimated at 319,400 cases [6]. Some studies have documented that the effective implementation of surveillance and advocacy programs in the control of ARF is constrained by limited access to primary health care. This is caused by the high cost of microbiological diagnosis of ARF using Anti-Streptolysin O (ASO) titer and throat swabs and the low index of suspicion by physicians coupled with a lack of awareness in the community [10-12]. It is important to note that since Group A Streptococcus (GAS) infections can be prevented with a vaccine developed against organisms that cause sepsis, arthritis, or pyoderma, there is a possibility that such a vaccine could also prevent all manifestations of GAS-related diseases [13]. Vaccination is considered the most effective strategy for reducing the incidence of ARF and curbing the rising prevalence of GAS-related diseases [14]. However, there has been no breakthrough in the clinical trial and development of vaccines. Sheel et al. [14] outlined a framework for vaccine development, emphasizing clinical trial design optimization, phase-specific development strategies and regulatory requirements for vaccine registration [14]. Poor perception and paucity of awareness of the cause, course, morbidity and mortality of ARF among clinical medical students could also contribute to the spread of the disease. A thorough assessment of the level of perception of ARF among clinical students is crucial in reducing the spread of the disease among this population. This study, therefore, aimed to document clinical students' perceptions of ARF and identify associated factors. Furthermore, the study investigated medical students' knowledge and perspectives on the potential for future vaccine development against ARF.Materials & Methods
Design and setting(s)
This was a cross-sectional study conducted in two medical schools in Southeast Nigeria from 14 March 2024 to 24 October 2024. It involved clinical medical students in their fourth to sixth year of study drawn from two South-eastern Nigerian medical schools: Ebonyi State University, Abakaliki, and Enugu State University of Science and Technology, Enugu.
Participants and sampling
Three hundred forty-one clinical medical students from two medical schools in Southeast Nigeria were enrolled consecutively in the study. The students were recruited consecutively until the sample size was reached. Medical students in the clinical class who provided informed consent were included in the study. In contrast, medical students in the pre-clinical class and those without consent were excluded from this study. A two-stage sampling technique was used to select the medical students for inclusion in the study. Six accredited medical schools in southeast Nigeria have clinical medical students. Two medical students were selected out of the six using a simple random sampling technique of balloting. In the second stage, a list of all medical students in the clinical classes (fourth year to sixth year) was made. On each day of data collection, the number of medical students in the three classes in each of the two selected schools who were present served as the sampling frame. The sampling interval was determined by dividing the total number by the sample size of 170, which represented the estimated number of students from each selected school who would participate in the study. Therefore, every medical student was recruited for the study based on the seating arrangement of the students in the three classes on each day of data collection. On each occasion, the index student was selected using a simple random sampling technique of balloting. The formula obtained the sample size: n = Z2pq ÷ d2 [15].
A minimum sample size of 347 students was obtained using the formula above.
Tools/Instruments
The study used a validated interviewer-administered questionnaire. Ray et al. [16] adapted this questionnaire using a group of students aged 10-16 randomly selected from different schools. The questionnaire covers questions on knowledge of ARF and willingness to be vaccinated, defined as the preparedness or readiness to receive a vaccine after considering the efficacy, benefits, adverse effects, and barriers associated with receiving such a vaccine [17]. Knowledge of ARF was assessed using 11 variables.
Five items focused on symptoms, with each correct response scoring one and incorrect response scoring 0. The other six variables for the ARF assessment focused on the disease's prevalence, the age group most likely to be affected, impact, diagnosis, treatment options and prevention of the disease. For these six variables, a correct answer by any respondent attracted four marks, while an incorrect answer was scored zero. Thus, the maximum obtainable mark for each respondent was 29. Knowledge of rheumatic fever vaccination was assessed using eight variables. Each correct response from the respondents attracted a score of one, while incorrect responses were scored zero. The maximum score each respondent could obtain is eight.
The questionnaire components related to socioeconomic status were developed using Principal Component Analysis (PCA) in STATA statistical software version 12. The eleven variables listed above served as inputs to the PCA. For the calculation of distribution cut points, quartiles were used. Each respondent was assigned the wealth index score of their family.
The quartiles were Q1 = Poorest, Q2 = The Very Poor, Q3 = The Poor, and Q4 = The Least Poor. The quartiles were further dichotomized into low socioeconomic class, comprising the poorest and very poor, and high socioeconomic class, comprising the poorest and least poor groups.
Cronbach's α was employed to assess the internal consistency of the questionnaire adapted from Ray et al. [18]. A score of 0.8 was achieved, indicating a satisfactory level of reliability. Additionally, Pearson's correlation coefficient was utilized to determine the test-retest reliability, with a score of 0.5 indicating a higher reliability.
Data collection methods
The questionnaires were distributed to the medical students during the didactic lecture period in the first and second semesters of the year of study.
Data analysis
Data entry and analysis were done using the Statistical Product and Service Solutions (IMB-SPSS) statistical software version 25. Continuous variables were represented using mean and standard deviation, while categorical variables were presented using frequencies and proportions. The mean knowledge score of ARF among the categories of independent variables was compared using the Student t-test when the groups were two and with analysis of variance if the groups were more than two.
The mean knowledge score of ARF vaccination among the categories of independent variables was compared using the Student t-test when the groups were two and with analysis of variance if the groups were more than two.
A p-value of <0.05 determined the level of statistical significance. A chi-square test and multivariate analysis through binary logistic regression were employed. Respondents who achieved a score of 50% or higher of the total possible score were considered to have good knowledge.
Results
Table 1 shows the socio-demographic characteristics of the respondents.
The mean ± SD of the age of the respondents was 24.3 ± 2.9 years. The highest proportion of the respondents, 67.2%, were under 25 years old, while the least proportion, 3.8%, were 30 years and above. A higher proportion of the respondents, 51.0%, were male. The majority of the respondents, 96.5%, were single. The highest proportion of the respondents, 64.2%, were in the fifth year of study, while the least proportion, 8.2%, were in the sixth year.
Table 1. Socio-demographic characteristics of respondents (n = 341)
Abbreviation: SD, standard deviation.
Table 2 shows awareness of ARF and rheumatic fever vaccine among the respondents. The majority of the respondents, 93.0%, were aware of ARF. The major sources of information included health workers (82.3%), internet/social media (61.8%), and friends (42.3%). Less than one-fifth of the respondents, 17.9%, were aware of the ARF vaccine. The major sources of information on the ARF vaccine included health workers, 77.0%; internet/social media, 50.8%; and friends, 39.3%.
Table 2. Awareness of ARF and rheumatic fever vaccine among the respondents (n = 341)
Note: Multiple responses encouraged.
Table 3 shows the respondents' knowledge of ARF and rheumatic fever vaccination. A higher proportion of the respondents, 88.9%, knew that shortness of breath is a symptom of rheumatic fever and rheumatic heart disease. A higher proportion of the respondents, 50.7%, knew that sore throat is a symptom of rheumatic fever. Most respondents, 56.0%, knew the age group 5-15 years were more likely to have rheumatic fever. A higher proportion of the respondents, 81.5%, knew that diagnosis is by history taking and past medical history of sore throat. The mean knowledge of ARF score was 14.8 ± 5.8. Most 86.8% of respondents knew vaccination could be a good measure to prevent diseases. The mean knowledge of ARF vaccination score was 4.5 ± 1.4. Less than half of the respondents, 45.7%, knew they were not in Nigeria's high-priority group for rheumatic fever vaccination. Less than one-tenth of the respondents, 8.5%, were aware of anyone who died from rheumatic fever. A minor proportion of the respondents, 5.6%, intend to receive vaccination for rheumatic fever when available. Table 4 shows the correlation matrix of variables, including the age of respondents, knowledge of ARF and knowledge of ARF vaccination. A very weak positive correlation existed between knowledge of ARF and rheumatic fever vaccination. Increases in ARF knowledge were associated with increases in ARF vaccination knowledge, and this relationship was statistically significant (n = 341, r = 0.141, p = 0.009). Table 5 and 6 compared mean scores of knowledge of ARF and
knowledge of ARF vaccination. The mean knowledge score of ARF was highest among the sixth-year students, 16.5 ± 5.9, and least among those in the fourth year, 11.6 ± 4.9, and the mean difference was statistically significant (F = 21.836, p < 0.001). The mean knowledge score for ARF was significantly higher among the respondents whose mothers had tertiary education, 15.1 ± 5.9 compared to those whose mothers had secondary education and below, 13.8 ± 5.1 (Student t = 1.990, p = 0.048). The mean knowledge score for ARF was higher among the respondents whose families were in the high socioeconomic class, 15.5 ± 5.6 compared to those in the low socioeconomic class. The mean difference was statistically significant (Student t = 2.374, p = 0.018). The mean knowledge score for rheumatic fever vaccination was significantly higher among respondents who perceived themselves as susceptible to ARF, with a score of 4.9 ± 1.2, compared to those who did not perceive themselves as susceptible, whose score was 4.4 ± 1.5 (Student t = 3.161, p = 0.002). The mean knowledge score for rheumatic fever vaccination was higher among the respondents who intend to receive rheumatic fever vaccination, 5.0 ± 1.3 when compared to those who did not intend to receive the vaccine, 4.4 ± 1.4 and the mean difference was found to be statistically significant, (Student t = 3.718, p < 0.001).
Table 3. Knowledge of ARF and rheumatic fever vaccination among the respondents (n = 341)
Abbreviation: SD, standard deviation.
Table 4. Correlation matrix of variables including age of respondents, knowledge of ARF and knowledge of rheumatic fever vaccination (n = 341)
Abbreviations: r, correlation co-efficient; p-value, probability value.
Table 5. Comparison of mean scores of knowledge of ARF and knowledge of rheumatic fever vaccination (n = 341)
Abbreviations: t, t-test statistic; F, analysis of variance statistic; SD, standard deviation; n, number of participants; Sig., Significance; p, probability value.
Table 6. Comparison of mean scores of knowledge of ARF and knowledge of rheumatic fever vaccination (n = 341)
Abbreviations: t, t-test statistic; F, analysis of variance statistic; SD, standard deviation; n, number of participants; Sig., Significance; p, probability value.
Discussion
This study aimed to explore the perception and awareness of ARF among clinical medical students and to document associated factors. A high level of awareness (93.3%) was noted among medical students. This may be attributed to the fact that most information on ARF was derived from health professionals. The level of awareness of ARF among medical students was significantly higher than that reported by Alnemari et al. [18] in Saudi Arabia, where a level of awareness of 55.2 % was reported in students in the College of Medicine and 33.3% in the College of Dentistry, 44.8% in the College of Pharmacy, 21.4% in the college of applied Medical sciences and 45.9% among college of nursing students. The present study's findings were higher than those of Nkoke et al. [19] and Chelo et al. [20]. The variation in awareness of ARF may be attributed to the differing medical curricula employed by the participating medical schools, the year of study of the medical students involved, and potentially the methodologies used by the authors. The study also showed that 56% of medical students know that ARF commonly affects children between the ages of 5 and 15 years. Similarly, only 41.6% noted that skin rash could trigger ARF. This was also similar to the study of Fakieha et al. [21], where 54.8% of the subjects knew that children aged 5 to 15 years old are susceptible to ARF. The association between skin rash (bacterial dermatitis) and ARF was noted in 46.1% of the reportage of Fakieha et al. [21]
The current study noted no association between gender and the perception of ARF. However, Fakieha et al. [21] noted gender as the only important factor affecting knowledge of ARF in their study. Other studies noted that females have better knowledge than males [22-29].
The study noted that fewer medical students (50.7%) knew that sore throat was a symptom of ARF. Concerning the association between bacterial sore throat and ARF, Kulik et al. [25] noted that over 79.5% of their subjects were aware of the link between a sore throat and ARF, which was also similar to the study of Manase et al. [26] where 73.1% of health workers were aware of this relationship between sore throat and ARF [25]. This poor awareness of the association between sore throat and ARF highlights the need for specific training and potential curriculum revisions.
Though 93.0% of the clinical medical students were aware of ARF, only a minor population had good knowledge of ARF in terms of epidemiology, spread and management. This indicates a serious and urgent need to intensify the dissemination of information on the epidemiology and spread of the diseases, especially among clinical medical students. This information should also be introduced to pre-clinical medical students to curb the militating effects of this disease. Besides, information on primary and secondary prevention and disease awareness should be provided in the early years of medical school [30].
It is noted in this study that students who were in the 6th year of study had more knowledge of ARF than those in a lower class. It is expedient to introduce the lecture on the awareness and prevention of ARF in the introductory class of the medical school. This finding contrasts with those of other studies [28–30]. Furthermore, students from high socioeconomic classes had a higher knowledge of ARF than those from a lower economic class. This finding was at variance with Machluf et al. [31], who documented the association of ARF with lower socioeconomic classes. The study showed that a major proportion of medical students (81.5%) were well-informed about the rising prevalence of ARF. Some studies have documented a rising prevalence of ARF, with 300,000–500,000 new cases diagnosed annually and approximately 230,000 related deaths [31].
About half (54.3%) of the medical students in the current study noted that the management of ARF includes using non-steroidal anti-inflammatory drugs, antibiotics and steroids. Fakieha et al. [21] corroborated the same results when they noted that 56.5% of their subjects were aware of using antibiotics to manage sore throat. Interestingly,
the current study found that 75.7% of the medical students recognized the non-availability of rheumatic fever vaccine, yet 78.9% were aware of the ongoing effort to develop such a vaccine. This good level of awareness could be explained by the correlational matrix, which showed a positive correlation between knowledge of ARF and knowledge of rheumatic fever vaccination.
Conclusion
There is a poor perception of ARF's clinical correlates and management among clinical medical students. Many medical students are aware of the development of an ARF vaccine. This is a clarion call to add the teaching of ARF to the curriculum at all levels in the medical school. This could reduce the burden and complications associated with the disease. Vigorous campaigns and changes in medical curricula, which should include lectures on ARF across all levels of medical school, may significantly increase the perception and management of ARF among medical students [45].
Ethical considerations
This was obtained from the Research and Ethics Committee of Enugu State University Teaching Hospital (Parklane) Enugu, Nigeria. Additionally, verbal informed consent was obtained from the participating medical students of the studied medical schools. The study adhered to established ethical principles and institutional guidelines throughout. The code for the approved work was ESUTHP/C-MAC/RA/034/158.
Artificial intelligence utilization for article writing
Not applicable.
Acknowledgment
We are grateful to the research assistant, Nnamdi, who helped in data entry.
Conflict of interest statement
The authors declare that they have no competing interests.
Author contributions
MC, ATC, OCN, ENO, ICN, JTO, NOO, and CNO conceived and designed this study, while JMC helped with the critical revision of the article. JMC and ENO also did the Data analysis/interpretation. All authors have read and approved the manuscript.
Funding
No organization funded this study. The authors personally covered all expenses incurred during the study.
Data availability statement
Data are, however, available from the authors upon reasonable request and with permission of the corresponding author.
Article Type : Orginal Research |
Subject:
Medical Education
Received: 2024/11/9 | Accepted: 2025/05/21 | Published: 2025/07/13
Received: 2024/11/9 | Accepted: 2025/05/21 | Published: 2025/07/13
References
1. Chinawa AT, Chinawa JM. Compendium of cardiac diseases among children presenting in tertiary institutions in southern Nigeria: a rising trend. Libyan Journal of Medicine. 2021;16(1):1966217. [DOI]
2. Chinawa JM, Eze JC, Obi I, et al. Synopsis of congenital cardiac disease among children attending university of Nigeria teaching hospital Ituku Ozalla, Enugu. BMC Research Notes. 2013;6:1-6. [DOI]
3. Chinawa JM, Obu HA, Eke CB, Eze JC. Pattern and clinical profile of children with complex cardiac anomaly at university of Nigeria teaching hospital, Ituku-Ozalla, Enugu State. Nigeria. Nigeria Journal of Clinical Practice. 2013;16(4):462-7. [DOI]
4. Josephat M. Chinawa, Fortune A. Ujunwa. Medical and social outcomes in the management of cardiac diseases in children. Common Pediatric Diseases: Current Challenges. 2023;2(1):130. [DOI]
5. Watkins DA, Johnson CO, Colquhoun SM, et al. Global, regional, and national burden of rheumatic heart disease 1990-2015. New England Journal of Medicine. 2017;377(8):713-722. [DOI]
6. Marijon E, Ou P, Celermajer DS, et al. Prevalence of rheumatic heart disease detected by echocardiographic screening. New England Journal of Medicine. 2007;357(5):470-6 [DOI]
7. Beaton A, Okello E, Lwabi P, Mondo C, McCarter R, Sable C. Echocardiography screening for rheumatic heart disease in Ugandan schoolchildren. Circulation. 2012;125(25):3127-32. [DOI]
8. Nkereuwem E, Ige OO, Yilgwan C, Jobe M, Erhart A, Bode-Thomas F. Prevalence of rheumatic heart disease in North-Central Nigeria: a school-based cross-sectional pilot study. Tropical Medicine and International Health. 2020;25(11):1408-1415. [DOI]
9. Susy Kotit, David I. W. Phillips, Ahmed Afifi, Magdi Yacoub. The “Cairo Accord”- Towards the Eradication of RHD: An Update Frontiers. Frontiers in Cardiovascular Medicine. 2021;8:690227. [DOI]
10. Nkoke C, Luchuo EB, Jingi A, Makoge, C. Rheumatic heart disease awareness in the south west region of Cameroon: a hospital based survey in a Sub-Saharan African setting. PLoS ONE. 2018;13(9): e0203864. [DOI]
11. Musuku J, Lungu JC, Machila, E et al. Epidemiology of pharyngitis as reported by Zambian school children and their families: implications for demand-side interventions to prevent rheumatic heart disease. BMC Infectious Diseases. 2017;17(1):473. [DOI]
12. Kotby AA, Habeeb NM, Ezz El Elarab S. Antistreptolysin O titer in health and disease: levels and significance. Pediatric Reports. 2012; 2;4(1): e8. [DOI]
13. Animasahun BA, Madise Wobo AD, Itiola AY, Adekunle MO, Kusimo OY, Thomas FB. The burden of rheumatic heart disease among children in Lagos: how are we fairing? Pan African Medical Journal. 2018; 29:150 [DOI]
14. Sheel M, Moreland NJ, Fraser JD, Carapetis J. Development of group A Streptococcal vaccine: an unmet global health need. Expert Review of Vaccines. 2016;15(2):227-38. [DOI]
15. Israel GD. Sampling the evidence of extension program impact. Gainesville, FL: University of Florida cooperative extension service, institute of food and agriculture sciences, EDIS; 1992. [Online]. Available from: [Accessed: Apr.12, 2025] [DOI]
16. Ray M, Guha S, Ray M, et al. A questionnaire survey for improving awareness of rheumatic heart disease among school-aged children in India. Indian Heart Journal. 2020;72(5):410-5. [DOI]
17. Zhong BL, Luo W, Li HM, et al. Knowledge, attitudes, and practices towards Covid-19 among Chinese residents during the rapid rise period of the Covid-19 outbreak: a quick online cross-sectional survey. International Journal of Biological Science. 2020;16:1745-52. [DOI]
18. Alnemari W, Bakry S, Albagami S, et al. Awareness and knowledge of rheumatic heart disease among medical students comparing to other health specialties students in Umm Al-Qura University, Makkah city, KSA: Analytic cross-sectional study. Medical Science. 2022;26(121):1-7 [DOI]
19. Nkoke C, Luchuo EB, Jingi AM, Makoge C, Hamadou B, Dzudie A. Rheumatic heart disease awareness in the South West region of Cameroon: a hospital based survey in a Sub-Saharan African setting. PLoS One. 2018;25;13(9):e0203864 [DOI]
20. Chelo D, Tasha L, Tamdja A, et al. Assessment of knowledge, attitudes and practices (KAP) on rheumatic heart disease among senior medical students in Cameroon. World Journal of Cardiovascular Disease. 2020;10(6):363-78. [DOI]
21. Fakieha AY, Zafer DO, Alkalash SH et al. Knowledge and attitude of rheumatic fever and rheumatic heart disease among the Makkah city population, Saudi Arabia. Cureus. 2024;2;16(1):e51539. [DOI]
22. Almadhi AA, Alshammri MR, Altamimi NO, et al. Rheumatic fever and rheumatic heart disease-related knowledge, attitude, and practice in Saudi Arabia. Cureus. 2021;13(11):e19997. [DOI]
23. Mougrabi MM, Aljuaid RS, Alrabie AD, Althumali NK, Alkhaldi LH, Alotaibi WD. Awareness of rheumatic fever and rheumatic heart disease among the population in Taif, Saudi Arabia 2020. Journal of Family Medicine and Primary Care. 2021;10(8):3056-63 [DOI]
24. Sayed AK, Se'eda H, Eltewacy NK, et al. Awareness of rheumatic heart disease in Egypt: a national multicenter study. Journal of Cardiovascular Development and Disease. 2021;4;8(9):108. [DOI]
25. Kulik E, Stuart B, Willcox M. Predictors of rheumatic fever in sore throat patients: a systematic review and meta-analysis. Transaction of the Royal Society of Tropical Medicine and Hygiene. 2022;4;116(4):286-297 [DOI]
26. 26. Manase M. Awareness of rheumatic heart disease prevention among primary health care providers and people age nine years and above in Kinondoni municipality. MSc. Dissertation. Dar Esalam; Tanzania. 2011. [Online]. Available from: [Accessed: Apr.12, 2025]. [DOI]
27. Carapetis JR, Beaton A, Cunningham MW, et al. Acute rheumatic fever and rheumatic heart disease. Nat Rev Dis Primers. 2016; 14;2:15084 [DOI]
28. Vaz LE, Kleinman KP, Lakoma MD, et al. Prevalence of parental misconceptions about antibiotic use. Pediatrics. 2015;136(2):221-31. [DOI]
29. María MR. Awareness of rheumatic heart disease prevention among primary health care providers and people aged nine years and above in Kinondoni municipality. Dar Esalam; Tanzania. [Online]. Available from: [Accessed: Apr.12, 2025]. [DOI]
30. Yadeta D, Hailu A, Haileamlak A, et al. Prevalence of rheumatic heart disease among school children in Ethiopia: a multisite echocardiography-based screening. International Journal of Cardiology. 2016;15; 221:260-3. [DOI]
31. Machluf Y, Chaiter Y, Farkash R, Sebbag A, Fink DL. Rheumatic fever in large cohort of adolescents in Israel. Frontiers in Medicine (Lausanne). 2020;6:328 [DOI]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
