
Wed, Jul 29, 2026
[Archive]
Volume 15, Issue 47 (2022)
J Med Edu Dev 2022, 15(47): 27-35 |
Back to browse issues page

Ethics code: IR.ZUMS.REC.1399.393
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Mousavi S K, Kamali M. Clinical self-efficacy of final-year nursing students: A comparison of a 360-degree evaluation method with a conventional method. J Med Edu Dev 2022; 15 (47) :27-35
URL: http://edujournal.zums.ac.ir/article-1-1662-en.html
URL: http://edujournal.zums.ac.ir/article-1-1662-en.html

1- Zanjan University of Medical Sciences , kazemmoosavi69@gmail.com
2- Zanjan University of Medical Sciences
2- Zanjan University of Medical Sciences
Full-Text [PDF 948 kb]
(1947 Downloads)
| Abstract (HTML) (3779 Views)
Results
According to the results, the mean±SD age of the participants was obtained at 22.69±1.35 years, and female students made up the majority of the participants (64.6%). Most of them were in the seventh semester (52.3%) and had a grade point average (GPA) between 15 and 17. The demographic characteristics of the participants are listed based on experimental and control groups in Table 1. According to the Chi-square test results, no statistically significant difference was observed between the two groups in this regard (P>0.05).
In the first step, data normality was examined for accurate inferential analysis. For this purpose, Kolmogorov-Smirnov statistical test was employed, and the results showed that the data collected from the statistical point of view based on experimental and control groups had a normal distribution (P>0.05). Therefore, the use of parametric statistical tests to analyze the data was unimpeded.
According to the results, the mean±SD of clinical self-efficacy score before the 360-degree evaluation in the control group was 78.27±17.52 in the range of moderate level. Moreover, the mean scores of clinical self-efficacy in the control group were moderate in assessment and planning and weak in intervention and evaluation. After implementing the 360-degree evaluation method, the mean±SD score of clinical self-efficacy in the control group was determined at 79.66±18.60, meaning it was in the range of moderate level. Similar to pre-implementation scores, dimensions of assessment and planning were moderate, and dimensions of intervention and evaluation were in the weak range.
Comparison of the clinical self-efficacy before and after implementing the 360-degree evaluation method in the control group showed no statistically significant difference between the total scores and each of their dimensions. However, in line with the central hypothesis of the research on the effectiveness of the 360-degree assessment method on the self-efficacy of nursing students, the results of paired sample t-test showed that the total self-efficacy score in the experimental group increased by 10.46 points (Score before implementation: 79.09±13.61, score after implementation: 89.56±15.77). This score difference is statistically significant according to the significance coefficient obtained (P<0.05). On the other hand, investigating the changes in the scores before and after the clinical self-efficacy in the experimental group showed that only changes in the scores of implementation and evaluation were statistically significant (P<0.05) (Table 2).
Table1. Frequency and percentages of demographic characteristics based on experimental and control groups (Chi-square test)
* Chi-square
Full-Text: (1610 Views)
Abstract
Background & Objective: The use of traditional clinical evaluation methods is one of the most critical challenges in obtaining professional competence and self-efficacy in clinical performance. This study aims to investigate the clinical self-efficacy of final-year nursing students by comparing a 360-degree evaluation method with a conventional evaluation method.
Materials & Methods: This quasi-experimental study was conducted on 65 final-year nursing students at Abhar School of Nursing who were selected by census method and randomly divided into two control and experimental groups. In the beginning, the participants completed the clinical self-efficacy questionnaire then a briefing session was held for the experimental group. In the next step, a clinical evaluation of the experimental group was performed using the 360-degree standard form for two weeks. Furthermore, a routine evaluation method was used for the control group. At the end of the internship, both groups completed the clinical self-efficacy questionnaire again. Data were analyzed in SPSS software (version 25) using ANOVA, paired, and independent t-tests.
Results: It was shown that the total self-efficacy score of the students in the experimental group increased after implementing the 360-degree method (P=0.003). Moreover, the clinical self-efficacy scores in the control and experimental groups revealed that the scores in the experimental group were significantly higher than those in the control group (P=0.024).
Conclusion: According to these findings, the use of the 360-degree evaluation method positively promotes students' clinical performance self-efficacy. Therefore, it is suggested that educational managers consider this evaluation method more and more as a comprehensive, appropriate, and efficient method for clinical courses
Introduction
The deployment The World Health Organization has introduced evaluating and promoting nurses' clinical skills as two basic principles to ensure care quality (1). In other words, clinical skills development is the primary concern of nursing schools and care provider systems (2). From the perspective of educational experts, nurses' poor clinical skills and performance are attributed to the gap between their theoretical and practical knowledge. This issue has been considered an unsolvable and significant challenge in nursing for the past 50 years. It has caused nurses to have fewer chances of using the theoretical and practical knowledge gained during their studies after entering the clinical field. A few years after graduation, nurses are further away from their past academic reserves (3). Due to this reason, clinical education is a mandatory and essential period of nursing education (4). From the view of nursing education planners, clinical education is the primary basis of nursing education (5). They believe that the deep gap between theoretical and clinical education negatively impacts students' clinical performance and does not allow them to show their competence and skills (6).
The focus of nursing education, especially clinical education, is to cultivate self-efficacy and bring students to the highest level of learning (7). Self-efficacy refers to a person's judgment of his/her ability to perform a work or task successfully (8). In addition, it regulates the process of stress (9) and compatibility, followed by increasing self-confidence and a sense of well-being among nursing students (10).
The result of self-efficacy improvement is the training of scientifically aware and clinically capable nurses. In the long run, it will develop the quality of care services and increase patient satisfaction (11). Even though training nurses with high competence and self-efficacy in the clinic is the primary mission of nursing schools, there are challenges in achieving this goal. One of the most critical challenges is the nursing students' current clinical evaluation method (12).
Nowadays, evaluation is an integral part of the teaching-learning process related to and carried out with the training. The main focus of the evaluation process is learning guidance instead of the classification of students and their comparison (13). Despite the variety of evaluation methods used in the training process, the limited evaluation domains can still be considered the most significant weakness (14). Since, traditionally, the student is evaluated only by the relevant instructor, there is a possibility of bias and personal taste in the evaluation process. Due to the presence of a high number of students in the internship groups, it is complicated and, in some cases, impossible to assess students' clinical competence and self-efficacy at the same time using an evaluator (15).
In recent years, the 360-degree evaluation method has been considered to assess learners' performance in professional and communication skills (16). It can be included to mention the application of this method for health care training in the medical professions (17), physical examination of nursing students (18), and performance of midwifery students (19). Different evaluators are an essential feature of this evaluation method.
Usually, in addition to the teacher, the evaluation is done by peers, hospital ward officials, patients, and the individual (20). Therefore, one of the most important goals of using the 360-degree evaluation method is to examine the abilities and skills of students in communicating and interacting with the patient, the patient's family, peers, and staff (21). In the 360-degree evaluation method, the student is evaluated simultaneously by several people and from different angles, and the student's strengths and weaknesses are well revealed (9). The combination of these factors and limited research on applying this method in nursing led the researcher to plan this study to compare the effect of the 360-degree clinical skills evaluation with a conventional evaluation method on nursing students' self-efficacy.
Materials and Methods
Design and duration
This quasi-experimental study with a pretest and posttest design and a control group aimed to investigate the clinical self-efficacy of final-year nursing students by comparing a 360-degree evaluation method with a conventional evaluation method from February to December 2021.
Participants and Sampling
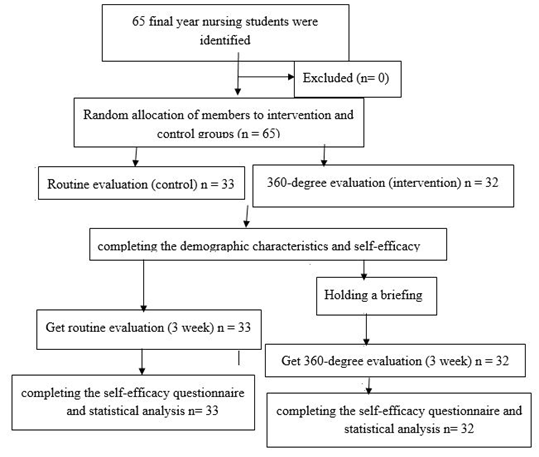
The participants of this study included all nursing students in the fourth year of nursing (seventh and eighth semesters) of Abhar School of Nursing and the research environment, internal medicine, surgery, and emergency educational centers of Al-Ghadir, Bu Ali Sina, and Emdadi hospitals. The sampling method was a census, and sample allocation was conducted in the form of control and experimental groups in a simple randomized manner based on the even or odd first digits to the right of the student's number. Based on the lottery, participants with even digits and holders of individual digits were assigned to the experimental and control groups. The willingness to participate in the study and passing at least 100 units of the total number of nursing undergraduate units were considered the inclusion criteria. On the other hand, non-participation and cancellation of attending the justification course were the criteria for the exclusion from the study (Figure 1).
Tools/Instruments
Data collection tools included demographic characteristics forms, standard 360-degree evaluation forms, and self-efficacy questionnaires in the clinical setting. The demographic characteristics questionnaire included age, gender, semester, grade point average, passed courses, and hospital units.
The standard 360-degree evaluation forms were designed in 2016 by Saheb Al-Zamani et al. The questionnaires included such five areas as interpersonal and communication skills, teamwork/co-working, professional behavior, service commitment, and medical ethics. Each question was scored on a Likert scale from 0 to 5 and was given to the student, instructor, ward manager, ward nurses, peers, and patients to answer. In a study by Saheb al-Zamani et al., the correlation values between 360-degree evaluation scores and the mean scores of theoretical and clinical courses were 0.32 (P=0.005) and 0.448 (P=0.001), respectively. The correlation between the subtests was also significant, and the correlation of the related total score was significant and more robust than the relationship of each subtest with the total, indicating the optimal theoretical structure of the test. The reliability of the test was calculated by Cronbach's alpha coefficient of 0.78 (22). In this study, the reliability of the questionnaire was calculated using Cronbach's alpha of 0.92.
The self-efficacy questionnaire in clinical practice was designed by Cheraghi et al. in 2005 and has 37 questions based on four areas of the nursing process (Patient examination: 12 questions; Nursing Diagnosis and Care Planning: 9 questions; Program implementation: 10 questions; and Plan evaluation: 6 questions) on a five-point Likert scale from 0 to 100 (not at all 0-29, not sure 30-49, relatively sure 50-69, sure 70-89, and completely sure 90-100). Individual scores range from 37 to 185, and a score of 0 to 37, 37-74, 74-111, 111-148, and 148 and above indicates very poor self-efficacy, poor, moderate, good, and very good self-efficacy, respectively (23).
In a study conducted by Cheraghi et al., the concurrent validity of the "clinical practice self-efficacy" with the "general self-efficacy" tools represented their appropriate validity (P<0.01, r=0.73). Furthermore, Cronbach's alpha coefficient (α=0.96) showed the appropriate internal consistency of the final instrument, and Cronbach's alpha coefficient for the four domains was calculated between 0.90 and 0.92. The retest with a two-week interval showed good instrument stability (r=0.94) (24). In a study conducted by Salimi et al., they determined the validity of the questionnaire through content validity and its reliability by the internal matching method. Cronbach's alpha coefficient was calculated at 0.83, indicating the optimal reliability of the instrument (25). The reliability of this questionnaire in the present study was calculated using Cronbach's alpha method as 0.89.
Data collection methods
After obtaining approval and permission to research from the Ethics Committee of Zanjan University of Medical Sciences, Zanjan, Iran, the researchers were referred to the educational center to explain the goals and method of research. They provided sufficient assurance about the confidentiality of information after obtaining permission from the center's managers and introducing themselves. Subsequently, the researchers divided the participants into experimental and control groups. After obtaining written consent and completing the demographic characteristics and self-efficacy questionnaire in clinical practice, the researchers reassured the students in both groups that this study was merely a research project and that attendance in either group had no effect on the instructor's evaluation score.
At the beginning of the study, a two-hour briefing session about the evaluation method was planned and conducted for the experimental group. At the end of the session, a 360-degree evaluation educational pamphlet prepared by library study and benefited from the opinions of 10 faculty members of Zanjan and Abhar School of Nursing and Midwifery was provided to this group. In addition to students, researchers gave this pamphlet to other evaluators (ward officials, nurses, clinical instructors, and patients). They gave them oral explanations of how to work and complete the questionnaire. During two skill internship units (18 days), teachers, peers, hospital ward officials, patients, and other nurses evaluated students daily in three educational and medical centers of internal medicine, surgery, and emergency wards. During this period, no intervention was applied to the control group, and the instructor continued to evaluate as usual. At the end of the internship, both control and experimental groups completed the self-efficacy questionnaires in clinical practice.
Data analysis
Data analysis was performed after collecting data and entering the latest version of SPSS software, using descriptive statistics (frequency, percentage, and mean±SD) and inferential statistics (ANOVA, paired, and independent t-test).
Background & Objective: The use of traditional clinical evaluation methods is one of the most critical challenges in obtaining professional competence and self-efficacy in clinical performance. This study aims to investigate the clinical self-efficacy of final-year nursing students by comparing a 360-degree evaluation method with a conventional evaluation method.
Materials & Methods: This quasi-experimental study was conducted on 65 final-year nursing students at Abhar School of Nursing who were selected by census method and randomly divided into two control and experimental groups. In the beginning, the participants completed the clinical self-efficacy questionnaire then a briefing session was held for the experimental group. In the next step, a clinical evaluation of the experimental group was performed using the 360-degree standard form for two weeks. Furthermore, a routine evaluation method was used for the control group. At the end of the internship, both groups completed the clinical self-efficacy questionnaire again. Data were analyzed in SPSS software (version 25) using ANOVA, paired, and independent t-tests.
Results: It was shown that the total self-efficacy score of the students in the experimental group increased after implementing the 360-degree method (P=0.003). Moreover, the clinical self-efficacy scores in the control and experimental groups revealed that the scores in the experimental group were significantly higher than those in the control group (P=0.024).
Conclusion: According to these findings, the use of the 360-degree evaluation method positively promotes students' clinical performance self-efficacy. Therefore, it is suggested that educational managers consider this evaluation method more and more as a comprehensive, appropriate, and efficient method for clinical courses
Introduction
The deployment The World Health Organization has introduced evaluating and promoting nurses' clinical skills as two basic principles to ensure care quality (1). In other words, clinical skills development is the primary concern of nursing schools and care provider systems (2). From the perspective of educational experts, nurses' poor clinical skills and performance are attributed to the gap between their theoretical and practical knowledge. This issue has been considered an unsolvable and significant challenge in nursing for the past 50 years. It has caused nurses to have fewer chances of using the theoretical and practical knowledge gained during their studies after entering the clinical field. A few years after graduation, nurses are further away from their past academic reserves (3). Due to this reason, clinical education is a mandatory and essential period of nursing education (4). From the view of nursing education planners, clinical education is the primary basis of nursing education (5). They believe that the deep gap between theoretical and clinical education negatively impacts students' clinical performance and does not allow them to show their competence and skills (6).
The focus of nursing education, especially clinical education, is to cultivate self-efficacy and bring students to the highest level of learning (7). Self-efficacy refers to a person's judgment of his/her ability to perform a work or task successfully (8). In addition, it regulates the process of stress (9) and compatibility, followed by increasing self-confidence and a sense of well-being among nursing students (10).
The result of self-efficacy improvement is the training of scientifically aware and clinically capable nurses. In the long run, it will develop the quality of care services and increase patient satisfaction (11). Even though training nurses with high competence and self-efficacy in the clinic is the primary mission of nursing schools, there are challenges in achieving this goal. One of the most critical challenges is the nursing students' current clinical evaluation method (12).
Nowadays, evaluation is an integral part of the teaching-learning process related to and carried out with the training. The main focus of the evaluation process is learning guidance instead of the classification of students and their comparison (13). Despite the variety of evaluation methods used in the training process, the limited evaluation domains can still be considered the most significant weakness (14). Since, traditionally, the student is evaluated only by the relevant instructor, there is a possibility of bias and personal taste in the evaluation process. Due to the presence of a high number of students in the internship groups, it is complicated and, in some cases, impossible to assess students' clinical competence and self-efficacy at the same time using an evaluator (15).
In recent years, the 360-degree evaluation method has been considered to assess learners' performance in professional and communication skills (16). It can be included to mention the application of this method for health care training in the medical professions (17), physical examination of nursing students (18), and performance of midwifery students (19). Different evaluators are an essential feature of this evaluation method.
Usually, in addition to the teacher, the evaluation is done by peers, hospital ward officials, patients, and the individual (20). Therefore, one of the most important goals of using the 360-degree evaluation method is to examine the abilities and skills of students in communicating and interacting with the patient, the patient's family, peers, and staff (21). In the 360-degree evaluation method, the student is evaluated simultaneously by several people and from different angles, and the student's strengths and weaknesses are well revealed (9). The combination of these factors and limited research on applying this method in nursing led the researcher to plan this study to compare the effect of the 360-degree clinical skills evaluation with a conventional evaluation method on nursing students' self-efficacy.
Materials and Methods
Design and duration
This quasi-experimental study with a pretest and posttest design and a control group aimed to investigate the clinical self-efficacy of final-year nursing students by comparing a 360-degree evaluation method with a conventional evaluation method from February to December 2021.
Participants and Sampling
The participants of this study included all nursing students in the fourth year of nursing (seventh and eighth semesters) of Abhar School of Nursing and the research environment, internal medicine, surgery, and emergency educational centers of Al-Ghadir, Bu Ali Sina, and Emdadi hospitals. The sampling method was a census, and sample allocation was conducted in the form of control and experimental groups in a simple randomized manner based on the even or odd first digits to the right of the student's number. Based on the lottery, participants with even digits and holders of individual digits were assigned to the experimental and control groups. The willingness to participate in the study and passing at least 100 units of the total number of nursing undergraduate units were considered the inclusion criteria. On the other hand, non-participation and cancellation of attending the justification course were the criteria for the exclusion from the study (Figure 1).
Tools/Instruments
Data collection tools included demographic characteristics forms, standard 360-degree evaluation forms, and self-efficacy questionnaires in the clinical setting. The demographic characteristics questionnaire included age, gender, semester, grade point average, passed courses, and hospital units.
The standard 360-degree evaluation forms were designed in 2016 by Saheb Al-Zamani et al. The questionnaires included such five areas as interpersonal and communication skills, teamwork/co-working, professional behavior, service commitment, and medical ethics. Each question was scored on a Likert scale from 0 to 5 and was given to the student, instructor, ward manager, ward nurses, peers, and patients to answer. In a study by Saheb al-Zamani et al., the correlation values between 360-degree evaluation scores and the mean scores of theoretical and clinical courses were 0.32 (P=0.005) and 0.448 (P=0.001), respectively. The correlation between the subtests was also significant, and the correlation of the related total score was significant and more robust than the relationship of each subtest with the total, indicating the optimal theoretical structure of the test. The reliability of the test was calculated by Cronbach's alpha coefficient of 0.78 (22). In this study, the reliability of the questionnaire was calculated using Cronbach's alpha of 0.92.
The self-efficacy questionnaire in clinical practice was designed by Cheraghi et al. in 2005 and has 37 questions based on four areas of the nursing process (Patient examination: 12 questions; Nursing Diagnosis and Care Planning: 9 questions; Program implementation: 10 questions; and Plan evaluation: 6 questions) on a five-point Likert scale from 0 to 100 (not at all 0-29, not sure 30-49, relatively sure 50-69, sure 70-89, and completely sure 90-100). Individual scores range from 37 to 185, and a score of 0 to 37, 37-74, 74-111, 111-148, and 148 and above indicates very poor self-efficacy, poor, moderate, good, and very good self-efficacy, respectively (23).
In a study conducted by Cheraghi et al., the concurrent validity of the "clinical practice self-efficacy" with the "general self-efficacy" tools represented their appropriate validity (P<0.01, r=0.73). Furthermore, Cronbach's alpha coefficient (α=0.96) showed the appropriate internal consistency of the final instrument, and Cronbach's alpha coefficient for the four domains was calculated between 0.90 and 0.92. The retest with a two-week interval showed good instrument stability (r=0.94) (24). In a study conducted by Salimi et al., they determined the validity of the questionnaire through content validity and its reliability by the internal matching method. Cronbach's alpha coefficient was calculated at 0.83, indicating the optimal reliability of the instrument (25). The reliability of this questionnaire in the present study was calculated using Cronbach's alpha method as 0.89.
Data collection methods
After obtaining approval and permission to research from the Ethics Committee of Zanjan University of Medical Sciences, Zanjan, Iran, the researchers were referred to the educational center to explain the goals and method of research. They provided sufficient assurance about the confidentiality of information after obtaining permission from the center's managers and introducing themselves. Subsequently, the researchers divided the participants into experimental and control groups. After obtaining written consent and completing the demographic characteristics and self-efficacy questionnaire in clinical practice, the researchers reassured the students in both groups that this study was merely a research project and that attendance in either group had no effect on the instructor's evaluation score.
At the beginning of the study, a two-hour briefing session about the evaluation method was planned and conducted for the experimental group. At the end of the session, a 360-degree evaluation educational pamphlet prepared by library study and benefited from the opinions of 10 faculty members of Zanjan and Abhar School of Nursing and Midwifery was provided to this group. In addition to students, researchers gave this pamphlet to other evaluators (ward officials, nurses, clinical instructors, and patients). They gave them oral explanations of how to work and complete the questionnaire. During two skill internship units (18 days), teachers, peers, hospital ward officials, patients, and other nurses evaluated students daily in three educational and medical centers of internal medicine, surgery, and emergency wards. During this period, no intervention was applied to the control group, and the instructor continued to evaluate as usual. At the end of the internship, both control and experimental groups completed the self-efficacy questionnaires in clinical practice.
Data analysis
Data analysis was performed after collecting data and entering the latest version of SPSS software, using descriptive statistics (frequency, percentage, and mean±SD) and inferential statistics (ANOVA, paired, and independent t-test).
Figure 1. CONSORT flow diagram
Results
According to the results, the mean±SD age of the participants was obtained at 22.69±1.35 years, and female students made up the majority of the participants (64.6%). Most of them were in the seventh semester (52.3%) and had a grade point average (GPA) between 15 and 17. The demographic characteristics of the participants are listed based on experimental and control groups in Table 1. According to the Chi-square test results, no statistically significant difference was observed between the two groups in this regard (P>0.05).
In the first step, data normality was examined for accurate inferential analysis. For this purpose, Kolmogorov-Smirnov statistical test was employed, and the results showed that the data collected from the statistical point of view based on experimental and control groups had a normal distribution (P>0.05). Therefore, the use of parametric statistical tests to analyze the data was unimpeded.
According to the results, the mean±SD of clinical self-efficacy score before the 360-degree evaluation in the control group was 78.27±17.52 in the range of moderate level. Moreover, the mean scores of clinical self-efficacy in the control group were moderate in assessment and planning and weak in intervention and evaluation. After implementing the 360-degree evaluation method, the mean±SD score of clinical self-efficacy in the control group was determined at 79.66±18.60, meaning it was in the range of moderate level. Similar to pre-implementation scores, dimensions of assessment and planning were moderate, and dimensions of intervention and evaluation were in the weak range.
Comparison of the clinical self-efficacy before and after implementing the 360-degree evaluation method in the control group showed no statistically significant difference between the total scores and each of their dimensions. However, in line with the central hypothesis of the research on the effectiveness of the 360-degree assessment method on the self-efficacy of nursing students, the results of paired sample t-test showed that the total self-efficacy score in the experimental group increased by 10.46 points (Score before implementation: 79.09±13.61, score after implementation: 89.56±15.77). This score difference is statistically significant according to the significance coefficient obtained (P<0.05). On the other hand, investigating the changes in the scores before and after the clinical self-efficacy in the experimental group showed that only changes in the scores of implementation and evaluation were statistically significant (P<0.05) (Table 2).
Table1. Frequency and percentages of demographic characteristics based on experimental and control groups (Chi-square test)
| P-value* | Control | Experimental | Variable | |
| 0.510 | 13 (39.4%) | 10 (31.2%) | Male | Gender |
| 20 (60.6%) | 22 (68.8%) | Female | ||
| 0.891 | 17 (51.5%) | 17 (53.1%) | 7th | Semester |
| 16 (48.5%) | 15 (46.9%) | 8th | ||
| 0.746 | 4 (12.1%) | 3 (9.4%) | <15 | Grade Point Average |
| 16 (48.5%) | 18 (56.3%) | 15-17 | ||
| 11 (33.3%) | 9 (28.1%) | 17-19 | ||
| 2 (6.1%) | 2 (6.3%) | >19 | ||
| 0.702 | 18 (54.5%) | 15 (46.9%) | <100 | Passed course |
| 15 (45.5%) | 17 (53.1%) | >100 | ||
| 0.911 | 15 (43.75%) | 14 (43.7%) | Non- intensive | Hospital units |
| 18 (56.25%) | 18 (56.3%) | Intensive | ||
* Chi-square
The scores of the experimental group before the 360-degree evaluation were almost similar to those of the control group. The results showed that the experimental group's clinical self-efficacy Mean±SD score before implementation was 79.09±13.61. Their scores in assessment and planning were at a moderate level, and dimensions of intervention and evaluation were in the weak range. A comparison of the clinical self-efficacy scores in the control and experimental groups before implementing the 360-degree evaluation showed no statistically significant difference between the total scores and their dimensions. Nevertheless, comparing the clinical self-efficacy scores in the control and experimental groups after implementing a 360-degree evaluation to the independent sample t-test showed a statistically significant difference.
In other words, the mean±SD of the clinical self-efficacy score of the experimental group after implementing the 360-degree evaluation was significantly higher than that of the control group. On the other hand, it was understood that the scores of self-efficacy after the implementation in the experimental group in terms of assessment, intervention, and evaluation dimensions were increased, compared to the control group, and these changes were statistically significant (P<0.05; Table 2).
In other words, the mean±SD of the clinical self-efficacy score of the experimental group after implementing the 360-degree evaluation was significantly higher than that of the control group. On the other hand, it was understood that the scores of self-efficacy after the implementation in the experimental group in terms of assessment, intervention, and evaluation dimensions were increased, compared to the control group, and these changes were statistically significant (P<0.05; Table 2).
Table 2. The results of the independent sample t-test and paired t-test to compare the mean score of the clinical self-efficacy in the control and experimental groups
| Self-efficacy | Time Group |
Before 360 (Mean & SD) |
After 360 (Mean & SD) |
T** (P-value) |
| Assessment |
Control | 31.33 ± 6.49 | 31.48 ± 6.77 | -0.091 (0.729) |
| Experimental | 31.81 ± 5.65 | 33.11 ± 6.06 | -0.73 (0.179) | |
| T* (P-value) | -0.32 (0.616) | -1.08 (0.048) |
| Planning |
Control | 18.97 ± 3.43 | 19.89 ± 4.01 | -0.479 (0.286) |
| Experimental | 19.09 ± 2.72 | 20.26 ± 3.17 | -0.66 (0.202) | |
| T* (P-value) | -0.15 (0.929) | -0.42 (0.334) |
| Intervention |
Control | 17.10 ± 3.89 | 17.38 ± 3.93 | -0.265 (0.470) |
| Experimental | 17.06 ± 3.21 | 22.07 ± 3.51 | -2.84 (0.018) | |
| T* (P-value) | 0.045 (0.964) | -5.15 (<0.001) |
| Evaluation |
Control | 10.87 ± 3.71 | 10.91± 3.89 | -0.053 (0.543) |
| Experimental | 11.13 ± 2.03 | 14.12 ± 3.03 | -1.69 (0.044) | |
| T* (P-value) | -0.35 (0.587) | -3.73 (0.002) |
| Total |
Control | 78.27 ± 17.52 | 79.66 ± 18.60 | - 0.888 (0.381) |
| Experimental | 79.09 ± 13.61 | 89.56 ± 15.77 | -5.926 (0.003) | |
| T* (P-value) | -0.210 (0.834) | -2.310 (0.024) |
* Independent sample t test, ** Pair t test
Discussion
This study aimed to investigate the clinical self-efficacy of final-year nursing students by comparing a 360-degree evaluation method with a conventional evaluation method. There was no significant difference between the experimental and control groups in demographic characteristics. The statistically significant difference in self-efficacy scores in clinical performance between the control and experimental groups was attributed to the use of the 360-degree evaluation method, and it was not affected by demographic characteristics. According to the study's findings, the mean self-efficacy score in the clinical performance of participants in both groups before the intervention was moderate. In line with the present study, the study conducted by Soleimani et al. showed that nursing students in both groups had moderate clinical self-efficacy before receiving the intervention (26).
Salimi et al. (25) and Bahador et al. (27) in their descriptive-analytical studies, reported the mean self-efficacy score in nursing students at 106 and 107, respectively, indicating a moderate level of clinical self-efficacy. Moreover, Pourteimour et al. showed that more than 53% of nursing students had moderate self-efficacy (28). Contrary to the present findings, the rate of clinical self-efficacy of nursing students has been reported at a high level in the studies conducted by Albagawi et al. (29) and Motahhari et al. (30) and also at a low level in the studies by Zhang et al. (31) and Kassem (32).
Considering several factors affecting nursing students' self-efficacy, it can be said that achieving different results of levels of self-efficacy in various studies is predictable and unavoidable, and factors, such as an academic semester, type of internship, and instructor can affect the self-efficacy of nursing students.
On the other hand, the current research showed that the mean total self-efficacy score in clinical practice before the intervention in the control and experimental groups was not significantly different. The two groups were homogeneous in terms of this variable. However, the self-efficacy results in clinical performance after the intervention increased dramatically in the experimental group, indicating the positive effect of 360-degree evaluation. Consistent with these findings, Samadi et al. showed that the 360-degree evaluation improved undergraduate students' clinical skills (8). Cormack et al. stated that using this method has improved clinical competence in master nursing students (33). Baradaran et al. also pointed out that the use of 360-degree evaluation increased the clinical performance of midwifery students (19).
In addition, Mousavi et al. considered this method helpful in evaluating the clinical skills of undergraduate operating room students (34). In this regard, in their study, Sadeghi et al. stated that using the 360-degree evaluation method could provide more information about nursing students' clinical performance using the views of different evaluators (16).
This study aimed to investigate the clinical self-efficacy of final-year nursing students by comparing a 360-degree evaluation method with a conventional evaluation method. There was no significant difference between the experimental and control groups in demographic characteristics. The statistically significant difference in self-efficacy scores in clinical performance between the control and experimental groups was attributed to the use of the 360-degree evaluation method, and it was not affected by demographic characteristics. According to the study's findings, the mean self-efficacy score in the clinical performance of participants in both groups before the intervention was moderate. In line with the present study, the study conducted by Soleimani et al. showed that nursing students in both groups had moderate clinical self-efficacy before receiving the intervention (26).
Salimi et al. (25) and Bahador et al. (27) in their descriptive-analytical studies, reported the mean self-efficacy score in nursing students at 106 and 107, respectively, indicating a moderate level of clinical self-efficacy. Moreover, Pourteimour et al. showed that more than 53% of nursing students had moderate self-efficacy (28). Contrary to the present findings, the rate of clinical self-efficacy of nursing students has been reported at a high level in the studies conducted by Albagawi et al. (29) and Motahhari et al. (30) and also at a low level in the studies by Zhang et al. (31) and Kassem (32).
Considering several factors affecting nursing students' self-efficacy, it can be said that achieving different results of levels of self-efficacy in various studies is predictable and unavoidable, and factors, such as an academic semester, type of internship, and instructor can affect the self-efficacy of nursing students.
On the other hand, the current research showed that the mean total self-efficacy score in clinical practice before the intervention in the control and experimental groups was not significantly different. The two groups were homogeneous in terms of this variable. However, the self-efficacy results in clinical performance after the intervention increased dramatically in the experimental group, indicating the positive effect of 360-degree evaluation. Consistent with these findings, Samadi et al. showed that the 360-degree evaluation improved undergraduate students' clinical skills (8). Cormack et al. stated that using this method has improved clinical competence in master nursing students (33). Baradaran et al. also pointed out that the use of 360-degree evaluation increased the clinical performance of midwifery students (19).
In addition, Mousavi et al. considered this method helpful in evaluating the clinical skills of undergraduate operating room students (34). In this regard, in their study, Sadeghi et al. stated that using the 360-degree evaluation method could provide more information about nursing students' clinical performance using the views of different evaluators (16).
According to the findings of another study, the student’s clinical self-efficacy scores were compared in the experimental and control groups after the intervention. The most remarkable improvement in clinical self-efficacy was in the two dimensions of implementation and evaluation of the care program. González-Gil et al. also described 360-degree evaluation as an innovative, motivational, and integrated approach to nursing students' clinical competence. Accordingly, being patient-centered is one of the essential features of this method; therefore, it can better evaluate the implementation and evaluation of the care program (35). Furthermore, in the experimental group before and after the intervention, changes in the dimensions of the patient's assessment and care program planning of the dimensions of clinical self-efficacy were insignificant. The findings of this section can be attributed to the type of student internship during the research. In this way, since the internship was a skill type, students' activities mainly included implementing and evaluating the care program. Therefore, the evaluation focused on clinical practices, and evaluators have less considered the dimensions of patient assessment and care planning.
One of the strengths of this study was the use of a standard checklist for the 360-degree evaluation of students. The most important limitation of the present study was the short duration of the intervention. Therefore, it is suggested that this method be implemented in at least one semester to further illustrate its strengths and drawbacks in future studies. On the other hand, it is recommended that the effectiveness of the 360-degree evaluation on the other clinical variables, including clinical belonging and clinical competence of nursing students, be investigated in future studies.
Conclusion
The present study shows that using the 360-degree evaluation method promotes self-efficacy in the clinical performance of fourth-year nursing students. This method can be used as a suitable evaluation method in the clinical environment. The quality of clinical performance of health care providers, especially nurses, one of the leading and most influential health system members, is an essential concern in any country. Therefore, training efficient and skilled nurses is a particular educational goal requiring a complete, comprehensive, and accurate training program. In this regard, the best training programs without a good evaluation plan will lose their effectiveness to a large extent. In the meantime, the evaluation of self-efficacy in nursing students' clinical performance as the most important expectation of the health system should be considered by educational planners.
Ethical considerations
This study was approved by the Research Ethics Committee of Zanjan University of Medical Sciences (IR.ZUMS.REC.1399.393). Ethical considerations, including confidentiality of participants' information, informed consent of the participants, explanation of the research goals, voluntary participation in the research, permission to leave the study at any time, and trusteeship in using literature, were considered in this study.
Acknowledgments
This study was retrieved from the research project approved by Zanjan University of Medical Sciences, Zanjan, Iran, in 2020. The authors appreciate the support of Zanjan University of Medical Sciences for this research project, the hospitals where the research is conducted, and especially the esteemed evaluators participating in the research.
Conflicts of interest
There are no conflicts of interest.
Funding
Nil.
One of the strengths of this study was the use of a standard checklist for the 360-degree evaluation of students. The most important limitation of the present study was the short duration of the intervention. Therefore, it is suggested that this method be implemented in at least one semester to further illustrate its strengths and drawbacks in future studies. On the other hand, it is recommended that the effectiveness of the 360-degree evaluation on the other clinical variables, including clinical belonging and clinical competence of nursing students, be investigated in future studies.
Conclusion
The present study shows that using the 360-degree evaluation method promotes self-efficacy in the clinical performance of fourth-year nursing students. This method can be used as a suitable evaluation method in the clinical environment. The quality of clinical performance of health care providers, especially nurses, one of the leading and most influential health system members, is an essential concern in any country. Therefore, training efficient and skilled nurses is a particular educational goal requiring a complete, comprehensive, and accurate training program. In this regard, the best training programs without a good evaluation plan will lose their effectiveness to a large extent. In the meantime, the evaluation of self-efficacy in nursing students' clinical performance as the most important expectation of the health system should be considered by educational planners.
Ethical considerations
This study was approved by the Research Ethics Committee of Zanjan University of Medical Sciences (IR.ZUMS.REC.1399.393). Ethical considerations, including confidentiality of participants' information, informed consent of the participants, explanation of the research goals, voluntary participation in the research, permission to leave the study at any time, and trusteeship in using literature, were considered in this study.
Acknowledgments
This study was retrieved from the research project approved by Zanjan University of Medical Sciences, Zanjan, Iran, in 2020. The authors appreciate the support of Zanjan University of Medical Sciences for this research project, the hospitals where the research is conducted, and especially the esteemed evaluators participating in the research.
Conflicts of interest
There are no conflicts of interest.
Funding
Nil.
Article Type : Orginal Research |
Subject:
Education
Received: 2022/07/28 | Accepted: 2022/12/6 | Published: 2022/12/19
Received: 2022/07/28 | Accepted: 2022/12/6 | Published: 2022/12/19
References
1. Ghorbani S, Heshmati Nabavi F, Heidarian Miri H, Mazlom S R, Akbari Rad S A, Mohebbi T. Evaluation of clinical competence of novice nurses from the perspective of head nurses, a cross-sectional descriptive study in mashhad university of medical sciences in 2019. Quarterly Journal of Nursing Management. 2021;10:60-67. [Article]
2. Lynne P L, Van Horn, ER. The state of the science on clinical evaluation in nursing education. Nursing Education Perspectives. 2019;40:4-10. [DOI]
3. Seyedamini B, Nouri M, Mahmoudifar Y, Esmaillo Y. Concepts in evaluating effective clinical education: a qualitative study of nursing students’ experiences. Health Technology Assessment in Action. 2021:5:1-7. [DOI]
4. Farzi S, Shahriari M, Farzi S. Exploring the challenges of clinical education in nursing and strategies to improve it: A qualitative study. Journal of Education and Health Promotion. 2018;7:1-8. [DOI]
5. Günaydin N, Coban SA. Experiences of nursing students during clinical education in mental health clinics: A phenomenological qualitative study. Nurse Education in Practice. 2021;54:1-7. [DOI]
6. Gamtessa LCh. Correlation between academic and clinical practice performance of nursing students at a pediatrics and child health nursing course; Mizan-tepi university, Ethiopia. Advances in Medical Education and Practice. 2021;12:155-162. [DOI]
7. Georgea TP, DeCristofaro C, Murphy PF. Self-efficacy and concerns of nursing students regarding clinical experiences. Nurse Education Today. 2020;90:1-6. [DOI]
8. Samadi N, Varei Sh, Ghiyasvandian Sh, Moshfeghi Sh. Evaluation the on feedback degree-360 on the evaluation of the clinical skills of the nursing students of Ardabil university medical of sciences. Journal of Clinical Nursing and Mid-wifery. 2019;7:250-257. [Article]
9. Shorey S, Lopez V. Self-Efficacy in a nursing context. Health promotion in health care – vital theories and research. Springer Cham. 2021;1:145-158. [DOI]
10. Brennan BA. The impact of self-efficacy based prebriefing on nursing student clinical competency and self-efficacy in simulation: An experimental study. Nurse Education Today. 2022;109:1-8. [DOI]
11. Akgül-Gündoğdu N, Selçuk-Tosun A. Examining the relationship between solution-focused thinking skills and self-efficacy levels of nursing students in Turkey. Journal of Professional Nursing. 2021;37:1180-1186. [DOI]
12. Øvrebø LJ, Dyrstad DN, Hansen BS. Assessment methods and tools to evaluate postgraduate critical care nursing students' competence in clinical placement. An integrative review. Nurse Education in Practice. 2022;58:1-14. [DOI]
13. Rørtveit K, Hansen BS, Joa I, Lode K, Severinsson E. Qualitative evaluation in nursing interventions- A review of the literature. Nursing Open. 2020;7:1285-1298. [DOI]
14. Lewallen LP, Van Horn ER. The state of the science on clinical evaluation in nursing education. Nurs Educ Perspect. 2019;40:4-10. [DOI]
15. Leighton K, Kardong-Edgren S, Gilbert GE. Are traditional and simulated clinical environments meeting nursing students’ learning needs?. Clinical Simulation in Nursing. 2021;59:85-93. [DOI]
16. Sadeghi T and Loripoor M. Usefulness of 360 degree evaluation in evaluating nursing students in Iran. Korean Journal of Medical Education. 2016;28:195–200. [DOI]
17. Georgieva D, Koleva G, Hristova I. Virtual Technologies in the Medical Professions - Creation of 360 - Degree Environments for Health Care Training. Technology, Education, Management Journal. 2021;10:1314-18. [DOI]
18. Yang TY, Huang Ch-H, An C, Weng Li-Ch. Construction and evaluation of a 360 degrees panoramic video on the physical examination of nursing students. Nurse Education in Practice. 2022;63:1-10. [DOI]
19. Baradaran H R, Kheirkhah M, Keykhosravi F. Using a 360degree feedback system for Performance Appraisal of Midwifery Students in Shahid Akbar Abadi Maternity hospital. Development Strategies in Medical Education. 2016;3:73-80. [Article]
20. Carlos VC, Salvador MG, Abraham EM, Erick CME, Corby MMR. 360-Degree evaluation review applied in top-level education. EUREKA: Social and Humanities. 2020;3:27-35. [DOI]
21. Awdishu L, Zheng A, Gerd Granas A, Galasso J, Macauley K, Butera C, Hutchins S, Wallace P, Garman K, Namba J. 360-Degree feedback model to enhance interprofessional learning. MedEdPublish. 2018;7:1-13. [DOI]
22. Sahebazamani M, Farahani H, Mehrbani E, Shahbazi M. Validity and reliability of 360-degree clinical evaluation in students' clinical evaluation nursing. Journal of Islamic Azad University of Medical Sciences 2016;26:264-270. [Article]
23. Cheraghi F, Hasani F, Alavimajd H. Developing and psychometric evaluation of clinical performance self-efficacy instrument for nursing students. Iranian Institute for Health Sciences Research. 2009;9:51-60. [DOI]
24. Cheraghi F, Hasani P, Riazi H. Correlation of self-efficacy with clinical performance of nursing students. Hamedan Journal of Nursing and Midwifery Care. 2011;19:35-40. [Article]
25. Salimi HR, Pourebrahimi M, Hoseinabadi-Farahani MJ. Clinical self-efficacy, dimensions and related factors among nursing students. Iranian Journal of Psychiatric Nursing (IJPN). 2017;5:1-7. [DOI]
26. Soleimani F, Aghal M, Partash N, Aliagha Sarighamish A, Maghsoodi E. The effect of mindfulness-based education on nursing students’ clinical self-efficacy. Journal of Clinical Nursing and Midwifery. 2021:9:823-831.
27. Bahador R S, Soltani F, Madadizadeh F. The assessment of relationship between creativity and self-efficacy of clinical performance based on the nursing process in nursing students of Kerman. Journal of Clinical Nursing and Midwifery. 2016;5:12-22.
28. Pourteimour S, Jamshidi H, Parizad N. Clinical belongingness and its relationship with clinical self-efficacy among nursing students: a descriptive correlational study. Nursing and Midwifery Studies. 2021;10:47-51. [DOI]
29. Albagawi B, Mahmoud Hussein F, Alotaibi JS, Albougami AS, Amer MF, Alsharari AF, Assiri ZA, Alramadhan SE. Self-efficacy and clinical competence of fourth-year nursing students: A self-reported study. International journal of Advanced and Applied Sciences. 2019;6:65-70. [DOI]
30. Motahari M, Rahimibashar M, Ghasemnegad S. The relationship between clinical self-efficacy and academic achievement motivation in nursing students. Research in Medical Education. 2020;12:10-20. [DOI]
31. Zhang Z J. Zhang C L, Zhang X G, Liu X M, Zhung S, Wang J. Relationship between self-efficacy beliefs and achievement motivation in student nurses. Chinese Nursing Research. 2016;2:67-70. [DOI]
32. Kassem AH. Bullying behaviors and self efficacy among nursing students at clinical settings: Comparative study. Journal of Education and Practice 2015;6:25-36. [Article]
33. Cormack Cormack CL, Jensen E, Durham CO, Smith G, Dumas B. The 360-degree evaluation model: A method for assessing competency in graduate nursing students. A pilot research study. Nurse Education Today. 2018;64:132-137. [DOI]
34. Mousavi S , Sabzevari S, Safizadeh H. A comparison of common and 360-degree evaluation methods in terms of clinical skills of surgical technology students in Kerman university of medical sciences, Iran, in 2013. Strides in Development of Medical Education. 2015;12:237-248. [Article]
35. González-Gil MT, Parro-Moreno AI, Oter-Quintana C, González-Blázquez C, Martínez-Marcos M, et al. 360-Degree evaluation: Towards a comprehensive, integrated assessment of performance on clinical placement in nursing degrees: A descriptive observational study. Nurse Education Today. 2020;95:1-9. [DOI]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
