
Sun, Aug 2, 2026
[Archive]
Volume 15, Issue 47 (2022)
J Med Edu Dev 2022, 15(47): 1-10 |
Back to browse issues page


Ethics code: IR.SUMS.REC.1398.476
![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Hosseini Ravesh R, Rezaiee R, Mosalanejad L. Validation of the Persian version of the short self-regulated learning questionnaire for medical students: A descriptive study. J Med Edu Dev 2022; 15 (47) :1-10
URL: http://edujournal.zums.ac.ir/article-1-1634-en.html
URL: http://edujournal.zums.ac.ir/article-1-1634-en.html

1- Shiraz university of medical Sciences
2- Jahrom University of Medical Sciences ,saedparsa2012@gmail.com
2- Jahrom University of Medical Sciences ,
Keywords: self-regulated learning, Validation, Short self-regulation Questionnaire, Medical Students, Active learning
Full-Text [PDF 938 kb]
(3105 Downloads)
| Abstract (HTML) (5037 Views)
Disciplines
The use of EFA for the SSRQ and Orthogonal Rotation led to the identification of six main factors, which were consistent with the scree plot provided by the software (Figure 1). Six main factors with a total explained variance of 60.96% were identified as six values with special values greater than 1. Varimax rotation was used to identify the questions that make up each factor. After Varimax rotation, the first, second, third, fourth, fifth, and sixth factors explain 16.09%, 12.22%, 9.88%, 9.55%, 40.8%, and 4.79% of the total variance, respectively. Table 2 lists all six factors extracted along with the amount of variance explained by each factor and the amount of factor load of each item. The factor load values of all questions, except items 11 and 28, were calculated at more than 0.4, and the two excepted items were removed from the questionnaire after EFA due to a low factor load.
CFA
According to the obtained results and diagrams of the factor analysis model (Figure 2), the factor analysis model with significant coefficients T (Figure 3), as well as data (Table 3) and standardized factor load values for all questions, except Question 8, were more than 0.4. Moreover, the construct validity of all values, except item 8, was confirmed at a significance level of 0.01. At the final evaluation, results were extracted from EFA, and the questionnaire was finally approved with 27 items.
In this diagram, the factors or components and the eigenvalues are respectively shown in the horizontal (Y) and vertical (X) axes, so that the eigenvalues are reduced along with moving to the right. The six identified factors of the research questionnaire have specific values greater than 1.
Table 2. Details of the factors extracted from the research questionnaire
Validity
The findings illustrated that the AVEs of all questionnaire factors were more than 0.5; therefore, the SSRQ had a good convergence. The divergent validity of the questionnaire was evaluated using the Fornell-Larcker criterion, and the results showed that the SSRQ had an acceptable level of divergence. The concurrent validity was assessed using Fisher's self-directed learning assessment questionnaire (19). The results of the concurrent validity assessment pointed to a high correlation between the components of the SSRQ and Fisher's self-directed learning assessment questionnaire.
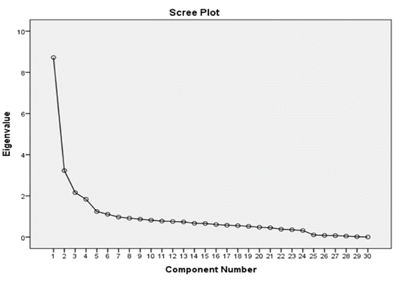
Figure 1. The scree plot for 6-factor rotation
.png)
Figure 2. Diagram of standardized path coefficients of the factor analysis model of the self-regulated learning questionnaire.
Table 3. Standardized factor load value and t-test
Reliability
Both Cronbach's alpha and combined reliability were used to assess the reliability of the SSRQ. The combined reliabilities (Delvin-Goldstein p) of all dimensions related to the components of the SSRQ, except the sixth dimension, were higher than 0.70. The total reliability of the questionnaire was calculated at 0.905 (Table 4). Therefore, the reliability of the measurement model was confirmed by removing the undesirable item (item 8) from the sixth factor (22). After the deletion of item 8, two items remained in the sixth factor. Since the factor load of the two remaining items in the sixth factor is above 0.7, it can be considered a factor of negligence.
Descriptive results of the study and the frequency of students in terms of degrees are presented in Table 1. Ph.D. students (53%) have the highest frequency, undergraduate students (46%) are in second place, and only 2% of all graduate students participated in the study. The characteristics of each of the six extracted factors, along with the amount of variance explained by each of the factors and the amount of factor load of each item, are demonstrated in Table 2. In this diagram, the factors or components and the eigenvalues are respectively shown in the horizontal (Y) and vertical (X) axes so that the eigenvalues are reduced along with moving to the right. The six identified factors of the research questionnaire have specific values greater than 1.
.png)
Figure 3. The statistical value chart of the factor analysis model of the self-regulated learning questionnaire.
Table 4. Reliability of factors in the questionnaire by Cronbach's alpha values
Discussion
The importance of self-regulation and its role in teaching and learning are highlighted in all available evidence and research. The results of the related studies suggest that the promotion of SRL skills in students increases their efficiency and effectiveness in learning environments (28,29). The SRL is one of the factors affecting a student's learning process, and students with self-regulation skills design, evaluate, and control their learning process (11), have better academic satisfaction and learning (8), and perform better in clinical settings (30). Numerous scales and questionnaires were developed regarding SRL.
This research pointed out that the levels of accuracy, commitment, and compliance were lower in the short form of the questionnaire (18). A research history illustrated that the short self-regulation scale was validated by Chen & Lin (16) on students in Taiwan using validity indicators in the analysis, while a revised shorter scale was developed by Brown, Miller, & Lewandowski (13). A valid and reliable tool is necessary for the identification of the factors affecting SRL and its promotion in the education and academic performance of learners. Therefore, six factors (goal setting, self-evaluation, perseverance, decision-making, mindfulness, and self-efficacy) were excluded from the validation process. There is some similarity that dominates the meaning of each construct in other countries. The result of this study also pointed to a difference between the extracted model and the results reported by other researchers (15, 21).
This questionnaire was normalized in many countries, including factors extracted with impulse control and goal-setting in the United States (15) with goal attainment, mindfulness, adjustment, proactiveness, and goal setting in Taiwan (16), on 1809 students from Slovakia, Lithuania, and Hungary with excluded factors self-discipline, goal-setting, learning from mistakes and impulse control in Central and Eastern Europe (17) extracted by mindfulness, self-efficacy, monitoring, change, goal, focus, and internal locus of control in South Africa (18, 19), and with four factors namely perseverance, goal setting, learning from mistakes, and decision-making in Spain (20, 21), all of which confirmed its high validity and reliability.
Moreover, three constructs, including goal setting, decision making, and perseverance, were examined in 265 Indonesian active college students (31). The present study identified six factors for the SRL questionnaire. The questionnaire factors were named according to the theoretical and research background and by knowledgeable experts and professors in the field of education. One of the factors identified in the study was the achievement of goal setting, which includes five items and indicates the measures taken by learners to track their progress to achieve their learning goals. In the present study, the goal achievement factor is in line with the goal orientation factor in the study by Gavora et al.(32) and the achievement goal in studies by Chen and Lin in Taiwan (26) and Šebeňa et al. (17).
In our study, the second identified factor of the SRL questionnaire was the self-assessment factor, which includes seven items in the questionnaire. Self-assessment provides an opportunity for the student to plan, monitor, and reflect on progress and achieve goals. The identification of the self-assessment factor in this study is similar to valid studies by Vosloo et al. on 200 black South African contexts (19). It may also be similar to the self-discipline factor excluded in Central and Eastern Europe (17) and in accordance with the study by Potgieter and Botha as an instance in the internal locus of control and monitoring in South Africa (18, 19).
The third factor extracted in the Iranian accreditation study is the step stability factor with three items, indicating a strong readiness and high power of focus on students' SRL goals. Potgieter and Botha (18) and Garzon et al. (21) also considered the step stability factor in their SSRQs. Self-efficacy was another factor in SRL identified in this study. This factor includes six items that indicate students' belief in their ability to succeed in a given situation. The identification of this factor is in line with the study by Vosloo et al. (19).
Decision-making has been cited as another factor identified in previously validated studies. In this study, this component was identified with four items, signifying an ability to identify the best way and path to achieve student goals. In identifying the decision factor, this research is in agreement with two previous valid studies by Potgieter and Botha (18) and Garzon et al. (21). Another identified factor was mindfulness which includes two items, indicating people's mental awareness of their actions, thoughts, and goals. The identification of the mindfulness factor is in line with identifying the subjectivity factor in the studies by Chen and Lin et al. (16) and Vosloo et al. (19), as well as the mindfulness factor in the research by Potgieter and Botha (18).
The findings of the present study suggested that Iranian self-regulated students have high levels of self-efficacy and mindfulness to achieve their learning goals. By making decisive decisions in choosing the right path of progress, they take a steady step toward the achievement of success and improvement of the process of their efforts by successive self-evaluation. The importance of improving the scientific level and preparation of students, especially those of medical universities, for lifelong learning has highlighted an increasing need for training and promotion of self-regulation skills in students (10). Therefore, any training needs a measurement and evaluation tool, whether in the stage of identifying basic knowledge and skills before training or in the stage of identifying the improvement of skills and their effectiveness during and after training. Therefore, researchers can use this scale to measure learners' SRL using various validated tools. One of the available tools is the questionnaire studied in this article, and SRL skills can be measured using this short and valid Persian tool.
Implications and Limitations
This study could provide a logical combination of SRL dimensions; however, only two or three items are located in the two mindfulness and gait stability factors. Future studies are suggested to add more related items to these factors to further enhance the psychometric quality of this tool. The use of observations and interviews can help supplement the data of this tool and gain a more comprehensive view of students' SRL. Furthermore, this tool can be used to measure students' levels of self-regulation in terms of age, gender, field, and degree in future studies. Among the limitation of the present study, we can refer to the mere inclusion of students of Shiraz University of Medical Sciences. Therefore, it is suggested to include students from other universities in future investigations for a higher external validity of the results. Moreover, the level of self-regulation of students can be compared to that of students in other universities of medical sciences.
Conclusion
Owing to the method of implementation and ease of scoring, the results generally demonstrated that the proposed scale with 27 items and six factors is a short, valid, and appropriate tool for the measurement of SRL in medical students. This tool assesses students' tendency to maintain and improve SRL skills in the field of education and training. Professors can use the data of this questionnaire to take advantage of the strengths, weaknesses, and readiness for the SRL of their students. Researchers, counselors of educational centers, and educational experts can measure the level of self-regulation of learners using this reliable tool to study the differences between learners in their educational status and improve their levels of academic achievement. If the present trait is lacking, they should teach cognitive and metacognitive skills and promote SRL skills in learners. In addition, the present tool can be used with the flexibility to measure SRL in other populations and different contexts.
Ethical considerations
This study has the approval of the Ethics Committee of Shiraz University of Medical Sciences, Shiraz, Iran (code: IR.SUMS.REC.1398.476). Participants were provided with adequate information about the study aim, confidential data management, and voluntariness of withdrawal from the study.
Acknowledgments
The authors greatly appreciate all students participating in this study.
Conflicts of Interest
The authors declare that they have no conflict of interest.
Contributions
RR Designed and conducted the study, collected and analyzed the data, and drafted the manuscript: LM Participated in analysis and interpretation; read and approved the final manuscript: All authors approved the final draft. RR Participated in the analysis and interpretation; read and approved the final manuscript.
Abbreviation
The Short Self-Regulation Questionnaire (SSRQ)
Exploratory Factor Analysis (EFA)
Confirmatory Factor Analysis (CFA)
Kaiser-Mayer-Olkin (KMO)
Full-Text: (2162 Views)
Abstract
Background & Objective: Self-regulated learning (SRL) is an active and self-centered process in which learners systematically guide and evaluate their cognitive, environmental, motivational, and behavioral factors to achieve learning goals using special strategies. The present study aimed to validate the Persian version of the short SRL questionnaire as an effective tool.
Materials & Methods: The present cross-sectional study was conducted among students of Shiraz University of Medical Sciences in 2020-2021. A total of 322 students participated by stratified random sampling. The research tool was a short SRL developed by Carey & Neal (2004). The convergent and divergent validities were evaluated using the average variance extracted (AVE). The validity of the structure was assessed using exploratory and confirmatory factor analyses, as well as the Fornelli-Larcker criterion. The reliability of the questionnaire was assessed by calculating the total Cronbach's alpha coefficient. Data were analyzed statistically using SPSS software (version 22) and Smart PLS 2.
Results: The results identified six main components of goal achievement, self-assessment, consistency, self-efficacy, decision-making, and mindfulness, with a total variance of 60.96%. A Cronbach's alpha of 0.90 was calculated for the whole questionnaire, and it was approved with 27 items. The AVE and the Fornell-Larcker criterion confirmed the high level of convergence and divergence of the questionnaire. Moreover, this questionnaire has a high correlation coefficient with the matched questionnaire.
Conclusion: The internal coherence, validity, and reliability of the short SRL questionnaire were confirmed in this study, and a short and standard tool was provided for the measurement of SRL in students. This questionnaire with an extracted scope can be used in future research.
Introduction
The deployment and training of experienced human resources and experts are considered one of the crucial goals of the educational system and the basis of the progress and development of any country. Universities, as a place for educating, teaching, and learning, should use the best learning programs and strategies to improve the quality of education (1). Cognitive theories and studies that try to explain learning and academic performance put an emphasis on learners' use of cognitive and metacognitive strategies when acquiring, storing, and remembering information (2). One of these strategies is the use of self-regulation skills that consider factors other than intelligence and aptitude in learning (3). In general, self-regulation can be defined as the processes by which individuals monitor, regulate, and control their cognition, motivation, and behavior (4). Self-regulatory theories have been used to explain how and why people strive to achieve various life goals, from losing weight and quitting smoking to learning to write and play music and even gaining expertise in medical sciences (5).
Educating students to optimize self-regulated learning (SRL) skills is a lifelong learning goal in response to the challenges of social change affecting teaching and learning (6). One of the appropriate teaching strategies is the development of students' self-regulation learning skills, which play a critical role in their performance and learning promotion (7). Some of these studies have demonstrated that self-regulation leads to increased academic satisfaction and better learning (8). Moreover, it increases the level of students' motivation and positively affects their academic performance (9). The importance of improving the scientific level of and preparation of students, especially students of medical universities, has highlighted the need for training and promotion of self-regulation skills in students (10). The importance of SRL in the field of education necessitates the assessment of this skill among learners (11). The importance of this issue lies in the special nature of medical sciences, as well as the characteristics of teaching and learning with a practical and skillful nature.
The application of an appropriate and standard tool can be effective in achieving research goals and applying the results of the study in educational environments (12). The question of how self-regulation can be measured has led experts to use a variety of tools. Brown and Miller et al. were among the first to develop a questionnaire to assess general self-regulation skills. This questionnaire consists of 63 items that evaluate seven factors: A) receiving information, b) evaluating information and comparing it with norms, c) triggering, d) searching for options, e) shaping the plan, f) executing the plan, and g) evaluating the effectiveness of the plan (13).13 Due to time constraints, long instruments are considered boring; therefore, efforts were made to develop shorter measuring instruments. Furthermore, the long forms of many questionnaires reduce users' accuracy and motivation to complete them. In addition, short forms increase researchers' willingness to complete the questionnaire due to their ease of use.
Carey and Neal et al. (2004) validated Brown and Miller's questionnaire with a sample of American students and extracted a shortened version of the questionnaire. The Short Self-Regulation Questionnaire (SSRQ) consists of 31 items on the Likert scale, which reduced the seven factors of the original version to a single-factor solution. Carey and Neal believe that this version reduces the burden on respondents and is a good alternative to the original version (14). The tool has been translated into various languages and validated in various countries, including the United States (15) Taiwan (16), Central and Eastern Europe (17), South Africa (18, 19), and Spain (20, 21), confirming its high validity and reliability.
The importance of the standardization of questionnaires in the cultural context of each country emphasizes the need to evaluate questionnaires before use. Moreover, the special characteristics of medical sciences, which will be considered in the teaching and learning of this group of students, make it necessary to review this questionnaire for this group of students. The use of a standardized short form will be more initiative while being feasible and usable in an application. Furthermore, a short standardized questionnaire in a specific sample and group can be used by interested researchers in future studies.
Material and Methods
Design and setting
This cross-sectional study was conducted at Shiraz University of Medical Sciences in 2020-21.
Participants and sampling
According to the number of questionnaire items and similar studies (14), 350 students were selected and participated in completing the questionnaires. Students were selected from different disciplines by a stratified random sampling method. The inclusion criteria entailed students' willingness to participate in research and passing one semester since the beginning of their studies. Out of 350 selected students participating in completing the questionnaire, those who filled out the questionnaire correctly and accurately were included in the study, and the rest were excluded from the research, resulting in 322 participants in the study.
Tools/Instruments
The main version of the Carey and Neal SSRQ (15) was used in this study. It consists of 31 items and is rated on a 5-point Likert scale (Strongly disagree=1, disagree=2, neither agree nor disagree = 3, agree=4, and strongly agree=5).
Data collection methods
The questionnaire was translated from English to Persian using the standard forward-backward method according to Guillemin et al. (1993) (22,23). To this end, the text of the SSRQ with 31 items was first translated into Persian independently by three English translation experts with sufficient experience in translating specialized texts. All three translations were reviewed by the research team, followed by preparing a single Persian version of the questionnaire. In the next step, the Persian version was back-translated by two translators fluent in Persian to English (different from the above translators), who were blind to the text of the main questionnaire. To eliminate possible errors, the texts obtained by one of the language professors of Shiraz University of Medical Sciences were compared with the original version, and a Persian version was prepared after necessary editions (16).
Data analysis
To evaluate the face and content validity of the questionnaire, professors and experts in the field of education at Shiraz University of Medical Sciences were asked in a meeting to provide the necessary feedback after a qualitative review. The questionnaire was then corrected based on their opinions. One item was removed from the questionnaire due to non-compliance with Iranian culture, and a Persian version of the questionnaire was finally prepared with 30 items. Content validity and reliability of the original version were determined as a pilot and test-re-test method and made available to 25 students. The calculated correlation coefficient of the test-re-test was obtained at 0.95 (17).
Upon the completion of these steps, the questionnaire was prepared for validation, and the initial version was distributed among the participants. Out of 350 questionnaires, 322 questionnaires were included in the study after the exclusion of 28 incomplete and distorted questionnaires. The number of samples required for the factor analysis for each item is acceptable between 3 and 10 cases (18). The concurrent validity was assessed using a self-directed questionnaire (19), consisting of 40 Likert-type items measuring three subscales: self-control, willingness to learn, and self-management, which was validated in Iran by Nadi et al. (24,25).
Data were analyzed statistically using SPSS software (version 22) and Smart.pls2. The construct validity was assessed by Exploratory Factor Analysis (EFA), Confirmatory Factor Analysis (CFA), and Pearson's correlation (to examine the relationship between research variables) at a significance level of 0.05. The hidden variables were identified and separated using the EFA (21). The appropriateness of the measurement tool (questionnaire) in terms of reliability, validity, and overall validity of the questionnaire was evaluated using CFA by Smart PLS 2 software. The EFA was performed using Kaiser-Mayer-Olkin (KMO) statistics and Bartlett's Test (18).18In the results, Bartlett's test was used to evaluate equal variances for all samples (26,27). The construct validity was evaluated using convergent and divergent validity by AVE and the Fornell-Larcker criterion, respectively. Cronbach's alpha coefficients of the whole questionnaire and the components were calculated to evaluate the reliability of the questionnaire (internal consistency of the questions). An alpha coefficient above 0.7 was considered adequate for acceptable reliability. To measure concurrent validity, the Pearson correlation test was used to assess the relationship between the two questionnaires (22).
Results
Among the selected statistical samples, 121 (37.6%) and 201 (62.4%) subjects were male and female, respectively. Students aged 20-27 years with a mean age of 22.43 years. Three students did not specify their ages. The characteristics of the students participating in the study by degree and field of study are displayed in Table 1.
EFA
The 30 items were analyzed using the analysis method of the main elements by vertical rotation and the Varimax technique. KMO statistic (0.88) greater than 0.70 illustrated that the collected data were suitable for the factor analysis. Since the measured significance level for the Bartlett statistic is zero (< a significance level of 0.05), the structure of the data was suitable for EFA (18). The requirement of the Measure of Sampling Adequacy (MSA) value is as follows:
MSA = 1, variables can be predicted
MSA > 0.5, variables can still be predicted
MSA < 0.5, variables cannot be predicted
Table 1. Frequency distribution of students by degrees
Background & Objective: Self-regulated learning (SRL) is an active and self-centered process in which learners systematically guide and evaluate their cognitive, environmental, motivational, and behavioral factors to achieve learning goals using special strategies. The present study aimed to validate the Persian version of the short SRL questionnaire as an effective tool.
Materials & Methods: The present cross-sectional study was conducted among students of Shiraz University of Medical Sciences in 2020-2021. A total of 322 students participated by stratified random sampling. The research tool was a short SRL developed by Carey & Neal (2004). The convergent and divergent validities were evaluated using the average variance extracted (AVE). The validity of the structure was assessed using exploratory and confirmatory factor analyses, as well as the Fornelli-Larcker criterion. The reliability of the questionnaire was assessed by calculating the total Cronbach's alpha coefficient. Data were analyzed statistically using SPSS software (version 22) and Smart PLS 2.
Results: The results identified six main components of goal achievement, self-assessment, consistency, self-efficacy, decision-making, and mindfulness, with a total variance of 60.96%. A Cronbach's alpha of 0.90 was calculated for the whole questionnaire, and it was approved with 27 items. The AVE and the Fornell-Larcker criterion confirmed the high level of convergence and divergence of the questionnaire. Moreover, this questionnaire has a high correlation coefficient with the matched questionnaire.
Conclusion: The internal coherence, validity, and reliability of the short SRL questionnaire were confirmed in this study, and a short and standard tool was provided for the measurement of SRL in students. This questionnaire with an extracted scope can be used in future research.
Introduction
The deployment and training of experienced human resources and experts are considered one of the crucial goals of the educational system and the basis of the progress and development of any country. Universities, as a place for educating, teaching, and learning, should use the best learning programs and strategies to improve the quality of education (1). Cognitive theories and studies that try to explain learning and academic performance put an emphasis on learners' use of cognitive and metacognitive strategies when acquiring, storing, and remembering information (2). One of these strategies is the use of self-regulation skills that consider factors other than intelligence and aptitude in learning (3). In general, self-regulation can be defined as the processes by which individuals monitor, regulate, and control their cognition, motivation, and behavior (4). Self-regulatory theories have been used to explain how and why people strive to achieve various life goals, from losing weight and quitting smoking to learning to write and play music and even gaining expertise in medical sciences (5).
Educating students to optimize self-regulated learning (SRL) skills is a lifelong learning goal in response to the challenges of social change affecting teaching and learning (6). One of the appropriate teaching strategies is the development of students' self-regulation learning skills, which play a critical role in their performance and learning promotion (7). Some of these studies have demonstrated that self-regulation leads to increased academic satisfaction and better learning (8). Moreover, it increases the level of students' motivation and positively affects their academic performance (9). The importance of improving the scientific level of and preparation of students, especially students of medical universities, has highlighted the need for training and promotion of self-regulation skills in students (10). The importance of SRL in the field of education necessitates the assessment of this skill among learners (11). The importance of this issue lies in the special nature of medical sciences, as well as the characteristics of teaching and learning with a practical and skillful nature.
The application of an appropriate and standard tool can be effective in achieving research goals and applying the results of the study in educational environments (12). The question of how self-regulation can be measured has led experts to use a variety of tools. Brown and Miller et al. were among the first to develop a questionnaire to assess general self-regulation skills. This questionnaire consists of 63 items that evaluate seven factors: A) receiving information, b) evaluating information and comparing it with norms, c) triggering, d) searching for options, e) shaping the plan, f) executing the plan, and g) evaluating the effectiveness of the plan (13).13 Due to time constraints, long instruments are considered boring; therefore, efforts were made to develop shorter measuring instruments. Furthermore, the long forms of many questionnaires reduce users' accuracy and motivation to complete them. In addition, short forms increase researchers' willingness to complete the questionnaire due to their ease of use.
Carey and Neal et al. (2004) validated Brown and Miller's questionnaire with a sample of American students and extracted a shortened version of the questionnaire. The Short Self-Regulation Questionnaire (SSRQ) consists of 31 items on the Likert scale, which reduced the seven factors of the original version to a single-factor solution. Carey and Neal believe that this version reduces the burden on respondents and is a good alternative to the original version (14). The tool has been translated into various languages and validated in various countries, including the United States (15) Taiwan (16), Central and Eastern Europe (17), South Africa (18, 19), and Spain (20, 21), confirming its high validity and reliability.
The importance of the standardization of questionnaires in the cultural context of each country emphasizes the need to evaluate questionnaires before use. Moreover, the special characteristics of medical sciences, which will be considered in the teaching and learning of this group of students, make it necessary to review this questionnaire for this group of students. The use of a standardized short form will be more initiative while being feasible and usable in an application. Furthermore, a short standardized questionnaire in a specific sample and group can be used by interested researchers in future studies.
Material and Methods
Design and setting
This cross-sectional study was conducted at Shiraz University of Medical Sciences in 2020-21.
Participants and sampling
According to the number of questionnaire items and similar studies (14), 350 students were selected and participated in completing the questionnaires. Students were selected from different disciplines by a stratified random sampling method. The inclusion criteria entailed students' willingness to participate in research and passing one semester since the beginning of their studies. Out of 350 selected students participating in completing the questionnaire, those who filled out the questionnaire correctly and accurately were included in the study, and the rest were excluded from the research, resulting in 322 participants in the study.
Tools/Instruments
The main version of the Carey and Neal SSRQ (15) was used in this study. It consists of 31 items and is rated on a 5-point Likert scale (Strongly disagree=1, disagree=2, neither agree nor disagree = 3, agree=4, and strongly agree=5).
Data collection methods
The questionnaire was translated from English to Persian using the standard forward-backward method according to Guillemin et al. (1993) (22,23). To this end, the text of the SSRQ with 31 items was first translated into Persian independently by three English translation experts with sufficient experience in translating specialized texts. All three translations were reviewed by the research team, followed by preparing a single Persian version of the questionnaire. In the next step, the Persian version was back-translated by two translators fluent in Persian to English (different from the above translators), who were blind to the text of the main questionnaire. To eliminate possible errors, the texts obtained by one of the language professors of Shiraz University of Medical Sciences were compared with the original version, and a Persian version was prepared after necessary editions (16).
Data analysis
To evaluate the face and content validity of the questionnaire, professors and experts in the field of education at Shiraz University of Medical Sciences were asked in a meeting to provide the necessary feedback after a qualitative review. The questionnaire was then corrected based on their opinions. One item was removed from the questionnaire due to non-compliance with Iranian culture, and a Persian version of the questionnaire was finally prepared with 30 items. Content validity and reliability of the original version were determined as a pilot and test-re-test method and made available to 25 students. The calculated correlation coefficient of the test-re-test was obtained at 0.95 (17).
Upon the completion of these steps, the questionnaire was prepared for validation, and the initial version was distributed among the participants. Out of 350 questionnaires, 322 questionnaires were included in the study after the exclusion of 28 incomplete and distorted questionnaires. The number of samples required for the factor analysis for each item is acceptable between 3 and 10 cases (18). The concurrent validity was assessed using a self-directed questionnaire (19), consisting of 40 Likert-type items measuring three subscales: self-control, willingness to learn, and self-management, which was validated in Iran by Nadi et al. (24,25).
Data were analyzed statistically using SPSS software (version 22) and Smart.pls2. The construct validity was assessed by Exploratory Factor Analysis (EFA), Confirmatory Factor Analysis (CFA), and Pearson's correlation (to examine the relationship between research variables) at a significance level of 0.05. The hidden variables were identified and separated using the EFA (21). The appropriateness of the measurement tool (questionnaire) in terms of reliability, validity, and overall validity of the questionnaire was evaluated using CFA by Smart PLS 2 software. The EFA was performed using Kaiser-Mayer-Olkin (KMO) statistics and Bartlett's Test (18).18In the results, Bartlett's test was used to evaluate equal variances for all samples (26,27). The construct validity was evaluated using convergent and divergent validity by AVE and the Fornell-Larcker criterion, respectively. Cronbach's alpha coefficients of the whole questionnaire and the components were calculated to evaluate the reliability of the questionnaire (internal consistency of the questions). An alpha coefficient above 0.7 was considered adequate for acceptable reliability. To measure concurrent validity, the Pearson correlation test was used to assess the relationship between the two questionnaires (22).
Results
Among the selected statistical samples, 121 (37.6%) and 201 (62.4%) subjects were male and female, respectively. Students aged 20-27 years with a mean age of 22.43 years. Three students did not specify their ages. The characteristics of the students participating in the study by degree and field of study are displayed in Table 1.
EFA
The 30 items were analyzed using the analysis method of the main elements by vertical rotation and the Varimax technique. KMO statistic (0.88) greater than 0.70 illustrated that the collected data were suitable for the factor analysis. Since the measured significance level for the Bartlett statistic is zero (< a significance level of 0.05), the structure of the data was suitable for EFA (18). The requirement of the Measure of Sampling Adequacy (MSA) value is as follows:
MSA = 1, variables can be predicted
MSA > 0.5, variables can still be predicted
MSA < 0.5, variables cannot be predicted
Table 1. Frequency distribution of students by degrees
| Grade | |||||
| Undergraduate | Graduate | Ph.D. | Total | ||
| Medical | Frequency | 0 | 1 | 104 | 105 |
| Percent | 0% | 1% | 99% | 100% | |
| Nursing and Midwifery | Frequency | 49 | 1 | 0 | 50 |
| Percent | 98% | 2% | 0% | 100% | |
| Dentistry | Frequency | 0 | 0 | 26 | 26 |
| Percent | 0 | 0 | 100% | 100% | |
| Pharmacy | Frequency | 0 | 0 | 38 | 38 |
| Percent | 0 | 0 | 100% | 100% | |
| Rehabilitation | Frequency | 19 | 0 | 0 | 19 |
| Percent | 100% | 0 | 0 | 100% | |
| Nutrition | Frequency | 21 | 0 | 0 | 21 |
| Percent | 100% | 0 | 0 | 100% | |
| Health | Frequency | 22 | 0 | 0 | 22 |
| Percent | 100% | 0 | 0 | 100% | |
| Paramedical | Frequency | 24 | 0 | 0 | 24 |
| Percent | 100% | 0 | 0 | 100% | |
| Modern Science and Technology |
Frequency | 0 | 0 | 5 | 5 |
| Percent | 0 | 0 | 100% | 100% | |
| Management | Frequency | 12 | 0 | 0 | 12 |
| Percent | 100% | 0 | 0 | 100% | |
| Total | Frequency | 147 | 2 | 173 | 322 |
| Percent | 46% | 1% | 53% | 100% |
The use of EFA for the SSRQ and Orthogonal Rotation led to the identification of six main factors, which were consistent with the scree plot provided by the software (Figure 1). Six main factors with a total explained variance of 60.96% were identified as six values with special values greater than 1. Varimax rotation was used to identify the questions that make up each factor. After Varimax rotation, the first, second, third, fourth, fifth, and sixth factors explain 16.09%, 12.22%, 9.88%, 9.55%, 40.8%, and 4.79% of the total variance, respectively. Table 2 lists all six factors extracted along with the amount of variance explained by each factor and the amount of factor load of each item. The factor load values of all questions, except items 11 and 28, were calculated at more than 0.4, and the two excepted items were removed from the questionnaire after EFA due to a low factor load.
CFA
According to the obtained results and diagrams of the factor analysis model (Figure 2), the factor analysis model with significant coefficients T (Figure 3), as well as data (Table 3) and standardized factor load values for all questions, except Question 8, were more than 0.4. Moreover, the construct validity of all values, except item 8, was confirmed at a significance level of 0.01. At the final evaluation, results were extracted from EFA, and the questionnaire was finally approved with 27 items.
In this diagram, the factors or components and the eigenvalues are respectively shown in the horizontal (Y) and vertical (X) axes, so that the eigenvalues are reduced along with moving to the right. The six identified factors of the research questionnaire have specific values greater than 1.
Table 2. Details of the factors extracted from the research questionnaire
| Variables | Questionnaire questions | Symbol | Amount of
factor load
|
Percentage of variance |
| Factor 1 | When I decide to make a change, I'm sure I will. | Q6 | 0.91 | 15.89 |
| As soon as I encounter a problem or challenge, I start to find all possible solutions. | Q10 | 0.920 | ||
| I'm used to doing something 'one way', even when it does not work. | Q12 | 0.92 | ||
| When I try to change something, I can usually find different 'solutions'. | Q22 | 0.93 | ||
| I learn from my mistakes. | Q29 | 0.93 | ||
| Factor 2 | I usually check my progress towards my goals. | Q2 | 0.71 | 12.77 |
| I am easily distracted from my plans. | Q3 | 0.65 | ||
| I have the ability to achieve the goals I have set for myself. | Q4 | 0.69 | ||
| I have personal standards and criteria that I try to implement well. | Q9 | 0.49 | ||
| I give up quickly. | Q21 | 0.62 | ||
| When I have a goal, I can usually plan to achieve it. | Q26 | 0.68 | ||
| I have trouble planning to achieve my goals. | Q30 | 0.57 | ||
| Factor 3 | I have a strong will. | Q15 | 0.87 | 11.60 |
| When I realize the effect and consequences of my actions, it is too late. | Q17 | 0.92 | ||
| I can resist the air of my breath. | Q18 | 0.92 | ||
| Factor 4 | I have trouble deciding my affairs. | Q1 | 0.51 | 9.36 |
| I often do not pay attention to what I do. | Q7 | 0.64 | ||
| When I decide to do something, I have trouble following and completing them. | Q16 | 0.66 | ||
| I usually postpone my decisions. | Q20 | 0.51 | ||
| I know how I want to be human. | Q24 | 0.45 | ||
| I usually think before I do anything. | Q25 | 0.62 | ||
| Factor 5 | If I decide to change something, I will do my best to do it. | Q5 | 0.40 | 8.63 |
| It is very difficult for me to set a goal for myself. | Q13 | 0.61 | ||
| When I have to make a decision to change something, I have to make different decisions. | Q14 | 0.66 | ||
| I set goals for myself and follow my progress towards the goals. | Q23 | 0.66 | ||
| Factor 6 | When I try to change something in myself, I pay close attention to how I do it. | Q8 | 0.55 | 7.86 |
| I do not seem to learn from my mistakes. | Q19 | 0.57 | ||
| I can follow a program that responds well. | Q27 | 0.42 |
Validity
The findings illustrated that the AVEs of all questionnaire factors were more than 0.5; therefore, the SSRQ had a good convergence. The divergent validity of the questionnaire was evaluated using the Fornell-Larcker criterion, and the results showed that the SSRQ had an acceptable level of divergence. The concurrent validity was assessed using Fisher's self-directed learning assessment questionnaire (19). The results of the concurrent validity assessment pointed to a high correlation between the components of the SSRQ and Fisher's self-directed learning assessment questionnaire.
Figure 1. The scree plot for 6-factor rotation
Figure 2. Diagram of standardized path coefficients of the factor analysis model of the self-regulated learning questionnaire.
Table 3. Standardized factor load value and t-test
| Variables | Symbol | Amount of factor load | t value | Result |
| Factor 1 | Q6 | 0.96 | 66.11 | Optimal |
| Q10 | 0.97 | 92.04 | Optimal | |
| Q12 | 0.96 | 44.93 | Optimal | |
| Q22 | 0.98 | 99.49 | Optimal | |
| Q29 | 0.99 | 446.74 | Optimal | |
| Factor 2 | Q2 | 0.71 | 11.04 | Optimal |
| Q3 | 0.66 | 8.76 | Optimal | |
| Q4 | 0.72 | 10.32 | Optimal | |
| Q9 | 0.61 | 6.69 | Optimal | |
| Q21 | 0.71 | 12.23 | Optimal | |
| Q26 | 0.67 | 8.88 | Optimal | |
| Q30 | 0.63 | 8.76 | Optimal | |
| Factor 3 | Q15 | 0.96 | 91.22 | Optimal |
| Q17 | 0.98 | 241.43 | Optimal | |
| Q18 | 0.99 | 272.49 | Optimal | |
| Factor 4 | Q1 | 0.57 | 5.77 | Optimal |
| Q7 | 0.58 | 4.89 | Optimal | |
| Q16 | 0.72 | 10.31 | Optimal | |
| Q20 | 0.71 | 9.90 | Optimal | |
| Q24 | 0.67 | 8.504 | Optimal | |
| Q25 | 0.58 | 12.64 | Optimal | |
| Factor 5 | Q5 | 0.62 | 6.07 | Optimal |
| Q13 | 0.70 | 7.70 | Optimal | |
| Q14 | 0.73 | 6.48 | Optimal | |
| Q23 | 0.71 | 9.98 | Optimal | |
| Factor 6 | Q8 | 0.31 | 1.22 | Adverse |
| Q19 | 0.71 | 8.29 | Optimal | |
| Q27 | 0.82 | 4.63 | Optimal |
Reliability
Both Cronbach's alpha and combined reliability were used to assess the reliability of the SSRQ. The combined reliabilities (Delvin-Goldstein p) of all dimensions related to the components of the SSRQ, except the sixth dimension, were higher than 0.70. The total reliability of the questionnaire was calculated at 0.905 (Table 4). Therefore, the reliability of the measurement model was confirmed by removing the undesirable item (item 8) from the sixth factor (22). After the deletion of item 8, two items remained in the sixth factor. Since the factor load of the two remaining items in the sixth factor is above 0.7, it can be considered a factor of negligence.
Descriptive results of the study and the frequency of students in terms of degrees are presented in Table 1. Ph.D. students (53%) have the highest frequency, undergraduate students (46%) are in second place, and only 2% of all graduate students participated in the study. The characteristics of each of the six extracted factors, along with the amount of variance explained by each of the factors and the amount of factor load of each item, are demonstrated in Table 2. In this diagram, the factors or components and the eigenvalues are respectively shown in the horizontal (Y) and vertical (X) axes so that the eigenvalues are reduced along with moving to the right. The six identified factors of the research questionnaire have specific values greater than 1.
Figure 3. The statistical value chart of the factor analysis model of the self-regulated learning questionnaire.
Table 4. Reliability of factors in the questionnaire by Cronbach's alpha values
| Factors | Composite reliability | Cronbach's alpha |
| Factor 1 | 0.98 | 0.98 |
| Factor 2 | 0.85 | 0.80 |
| Factor 3 | 0.98 | 0.98 |
| Factor 4 | 0.82 | 0.75 |
| Factor 5 | 0.78 | 0.64 |
| Factor 6 | 0.46 | 0.02 |
| Total reliability | 0.90 | |
Discussion
The importance of self-regulation and its role in teaching and learning are highlighted in all available evidence and research. The results of the related studies suggest that the promotion of SRL skills in students increases their efficiency and effectiveness in learning environments (28,29). The SRL is one of the factors affecting a student's learning process, and students with self-regulation skills design, evaluate, and control their learning process (11), have better academic satisfaction and learning (8), and perform better in clinical settings (30). Numerous scales and questionnaires were developed regarding SRL.
This research pointed out that the levels of accuracy, commitment, and compliance were lower in the short form of the questionnaire (18). A research history illustrated that the short self-regulation scale was validated by Chen & Lin (16) on students in Taiwan using validity indicators in the analysis, while a revised shorter scale was developed by Brown, Miller, & Lewandowski (13). A valid and reliable tool is necessary for the identification of the factors affecting SRL and its promotion in the education and academic performance of learners. Therefore, six factors (goal setting, self-evaluation, perseverance, decision-making, mindfulness, and self-efficacy) were excluded from the validation process. There is some similarity that dominates the meaning of each construct in other countries. The result of this study also pointed to a difference between the extracted model and the results reported by other researchers (15, 21).
This questionnaire was normalized in many countries, including factors extracted with impulse control and goal-setting in the United States (15) with goal attainment, mindfulness, adjustment, proactiveness, and goal setting in Taiwan (16), on 1809 students from Slovakia, Lithuania, and Hungary with excluded factors self-discipline, goal-setting, learning from mistakes and impulse control in Central and Eastern Europe (17) extracted by mindfulness, self-efficacy, monitoring, change, goal, focus, and internal locus of control in South Africa (18, 19), and with four factors namely perseverance, goal setting, learning from mistakes, and decision-making in Spain (20, 21), all of which confirmed its high validity and reliability.
Moreover, three constructs, including goal setting, decision making, and perseverance, were examined in 265 Indonesian active college students (31). The present study identified six factors for the SRL questionnaire. The questionnaire factors were named according to the theoretical and research background and by knowledgeable experts and professors in the field of education. One of the factors identified in the study was the achievement of goal setting, which includes five items and indicates the measures taken by learners to track their progress to achieve their learning goals. In the present study, the goal achievement factor is in line with the goal orientation factor in the study by Gavora et al.(32) and the achievement goal in studies by Chen and Lin in Taiwan (26) and Šebeňa et al. (17).
In our study, the second identified factor of the SRL questionnaire was the self-assessment factor, which includes seven items in the questionnaire. Self-assessment provides an opportunity for the student to plan, monitor, and reflect on progress and achieve goals. The identification of the self-assessment factor in this study is similar to valid studies by Vosloo et al. on 200 black South African contexts (19). It may also be similar to the self-discipline factor excluded in Central and Eastern Europe (17) and in accordance with the study by Potgieter and Botha as an instance in the internal locus of control and monitoring in South Africa (18, 19).
The third factor extracted in the Iranian accreditation study is the step stability factor with three items, indicating a strong readiness and high power of focus on students' SRL goals. Potgieter and Botha (18) and Garzon et al. (21) also considered the step stability factor in their SSRQs. Self-efficacy was another factor in SRL identified in this study. This factor includes six items that indicate students' belief in their ability to succeed in a given situation. The identification of this factor is in line with the study by Vosloo et al. (19).
Decision-making has been cited as another factor identified in previously validated studies. In this study, this component was identified with four items, signifying an ability to identify the best way and path to achieve student goals. In identifying the decision factor, this research is in agreement with two previous valid studies by Potgieter and Botha (18) and Garzon et al. (21). Another identified factor was mindfulness which includes two items, indicating people's mental awareness of their actions, thoughts, and goals. The identification of the mindfulness factor is in line with identifying the subjectivity factor in the studies by Chen and Lin et al. (16) and Vosloo et al. (19), as well as the mindfulness factor in the research by Potgieter and Botha (18).
The findings of the present study suggested that Iranian self-regulated students have high levels of self-efficacy and mindfulness to achieve their learning goals. By making decisive decisions in choosing the right path of progress, they take a steady step toward the achievement of success and improvement of the process of their efforts by successive self-evaluation. The importance of improving the scientific level and preparation of students, especially those of medical universities, for lifelong learning has highlighted an increasing need for training and promotion of self-regulation skills in students (10). Therefore, any training needs a measurement and evaluation tool, whether in the stage of identifying basic knowledge and skills before training or in the stage of identifying the improvement of skills and their effectiveness during and after training. Therefore, researchers can use this scale to measure learners' SRL using various validated tools. One of the available tools is the questionnaire studied in this article, and SRL skills can be measured using this short and valid Persian tool.
Implications and Limitations
This study could provide a logical combination of SRL dimensions; however, only two or three items are located in the two mindfulness and gait stability factors. Future studies are suggested to add more related items to these factors to further enhance the psychometric quality of this tool. The use of observations and interviews can help supplement the data of this tool and gain a more comprehensive view of students' SRL. Furthermore, this tool can be used to measure students' levels of self-regulation in terms of age, gender, field, and degree in future studies. Among the limitation of the present study, we can refer to the mere inclusion of students of Shiraz University of Medical Sciences. Therefore, it is suggested to include students from other universities in future investigations for a higher external validity of the results. Moreover, the level of self-regulation of students can be compared to that of students in other universities of medical sciences.
Conclusion
Owing to the method of implementation and ease of scoring, the results generally demonstrated that the proposed scale with 27 items and six factors is a short, valid, and appropriate tool for the measurement of SRL in medical students. This tool assesses students' tendency to maintain and improve SRL skills in the field of education and training. Professors can use the data of this questionnaire to take advantage of the strengths, weaknesses, and readiness for the SRL of their students. Researchers, counselors of educational centers, and educational experts can measure the level of self-regulation of learners using this reliable tool to study the differences between learners in their educational status and improve their levels of academic achievement. If the present trait is lacking, they should teach cognitive and metacognitive skills and promote SRL skills in learners. In addition, the present tool can be used with the flexibility to measure SRL in other populations and different contexts.
Ethical considerations
This study has the approval of the Ethics Committee of Shiraz University of Medical Sciences, Shiraz, Iran (code: IR.SUMS.REC.1398.476). Participants were provided with adequate information about the study aim, confidential data management, and voluntariness of withdrawal from the study.
Acknowledgments
The authors greatly appreciate all students participating in this study.
Conflicts of Interest
The authors declare that they have no conflict of interest.
Contributions
RR Designed and conducted the study, collected and analyzed the data, and drafted the manuscript: LM Participated in analysis and interpretation; read and approved the final manuscript: All authors approved the final draft. RR Participated in the analysis and interpretation; read and approved the final manuscript.
Abbreviation
The Short Self-Regulation Questionnaire (SSRQ)
Exploratory Factor Analysis (EFA)
Confirmatory Factor Analysis (CFA)
Kaiser-Mayer-Olkin (KMO)
Article Type : Orginal Research |
Received: 2022/06/19 | Accepted: 2022/12/4 | Published: 2022/12/19
Received: 2022/06/19 | Accepted: 2022/12/4 | Published: 2022/12/19
References
1. Zimmerman BJ, Pons MM. Development of a structured interview for assessing student use of self-regulated learning strategies. American Educational Research Journal. 1986;23(4):614-28. [DOI]
2. Zare M, Zeinalipour H, Naserijahromi R. Study of the relationship between self-regulated learners strategies with academic achievement. Research in Medical Education. 2018;9(4):48-56. [DOI]
3. Jaramillo A, Salinas-Cerda JP, Fuentes P. Self-Regulated Learning and Academic Performance in Chilean University Students in Virtual Mode During the Pandemic: Effect of the 4Planning App. Frontiers in Psychology. 2022;13. [DOI]
4. Zimmerman BJ. Attaining self-regulation: A social cognitive perspective. Handbook of self-regulation: Elsevier; 2000. p. 13-39. [DOI]
5. Artino J, Anthony R, Brydges R, Gruppen LD. Self‐regulated learning in healthcare profession education: theoretical perspectives and research methods. Researching Medical Education. 2015:155-66. [DOI]
6. de la Fuente J ZL, Martínez-Vicente JM, Cardelle-Elawar M, Sander P, Justicia F, Pichardo MC, García-Belén AB. Regulatory teaching and self-regulated learning in college students: confirmatory validation study of the IATLP scales. Electronic Journal of Research in Educational Psychology. 2012:10(2):839-66. [DOI]
7. Chen CM, Chen LC, Yang SM. An English vocabulary learning app with self-regulated learning mechanism to improve learning performance and motivation. Computer Assisted Language Learning. 2019 Mar 4;32(3):237-60. [DOI]
8. Van Alten DC, Phielix C, Janssen J, Kester L. Self-regulated learning support in flipped learning videos enhances learning outcomes. Computers & Education. 2020;158:104000. [DOI]
9. Cazan A-M. Teaching Self Regulated Learning Strategies for Psychology Students. Procedia - Social and Behavioral Sciences. 2013;78:743-7. [DOI]
10. Lucieer SM, Jonker L, Visscher C, Rikers RM, Themmen AP. Self-regulated learning and academic performance in medical education. Medical Teacher. 2016;38(6):585-93. [DOI]
11. Jansen RS, Van Leeuwen A, Janssen J, Jak S, Kester L. Self-regulated learning partially mediates the effect of self-regulated learning interventions on achievement in higher education: A meta-analysis. Educational Research Review. 2019;28:100292. [DOI]
12. Borjalilu S, Mojtahedzadeh R, Mohammadi A. Exploring the validity, reliability and factor analysis of self-regulation scale for medical students. Medical Education and Development.25-35:(2)8;2013. [Article]
13. Brown, J., Miller, WR., & Lawendowski, LA. The self-regulation questionnaire. In L. VandeCreek, & TL. Jackson (Eds.), Innovations in Clinical Practice: A Source Book, Vol. 17 Professional Resource Press; 1999.
14. Carey KB, Neal DJ, Collins SE. A psychometric analysis of the self-regulation questionnaire. Addictive Behaviors. 2004;29(2):253-60. [DOI]
15. Neal DJ, Carey KB. A follow-up psychometric analysis of the self-regulation questionnaire. Psychology of Addictive Behaviors. 2005;19(4):414. [DOI]
16. Chen YH, Lin YJ. Validation of the Short Self-Regulation Questionnaire for Taiwanese College Students (TSSRQ). Frontiers in Psychology. 2018;9:259. [DOI]
17. Šebeňa R, Orosová O, Helmer S, Petkeviciene J, Salonna F, Lukacs A, et al. Psychometric evaluation of the Short Self-Regulation Questionnaire across three European countries. Studia Psychologica. 2018;60(1):5-15. [DOI]
18. Potgieter JC, Botha KF. Psychometric properties of the short self-regulation questionnaire (SSRQ) in a South African context. Journal of Psychology in Africa. 2009;19(3):321-8. [DOI]
19. Vosloo M, Potgieter J, Temane M, Ellis S, Khumalo T. Validation of the Short Self-Regulation Questionnaire in a group of Black teachers: The SABPA study. SA Journal of Industrial Psychology. 2013;39(1):1-10. [DOI]
20. Pichardo C, Justicia F, de la Fuente J, Martínez-Vicente JM, Berbén AB. Factor structure of the self-regulation questionnaire (SRQ) at Spanish Universities. The Spanish Journal of Psychology. 2014;17. [DOI]
21. Garzon Umerenkova A, de la Fuente Arias J, Martinez-Vicente JM, Zapata Sevillano L, Pichardo MC, Garcia-Berben AB. Validation of the Spanish Short Self-Regulation Questionnaire (SSSRQ) through Rasch Analysis. Frontiers in Psychology. 2017;8:276. [DOI]
22. Anthoine E, Moret L, Regnault A, Sébille V, Hardouin J-B. Sample size used to validate a scale: a review of publications on newly-developed patient reported outcomes measures. Health and Quality of Life Outcomes. 2014;12(1):1-10. [DOI]
23. Guillemin F, Bombardier C, Beaton D. Cross-cultural adaptation of health-related quality of life measures: literature review and proposed guidelines. Journal of Clinical Epidemiology. 1993 Dec 1;46(12):1417-32. [DOI]
24. Fooladvand M, Nadi MA. Validation of revisited self-directed learning readiness scale for nursing education among Iranian nursing and midwifery students. Journal of Education and hHealth Promotion. 2019;8. [DOI]
25. Fisher M, King J, Tague G. Development of a self-directed learning readiness scale for nursing education. Nurse Education Today. 2001;21(7):516-25. [DOI]
26. Nunnally JC. Psychometric theory 3E: Tata McGraw-hill Education; 1994.
27. Munro BH. Statistical methods for health care research: Lippincott Wwilliams & Wilkins; 2005.
28. Shen WQ, Chen HL, Hu Y. The validity and reliability of the self-directed learning instrument (SDLI) in mainland Chinese nursing students. BMC Medical Education. 2014 Dec;14(1):1-7. [DOI]
29. Nückles M, Roelle J, Glogger-Frey I, Waldeyer J, Renkl A. The self-regulation-view in writing-to-learn: Using journal writing to optimize cognitive load in self-regulated learning. Educational Psychology Review. 2020:1-38. [DOI]
30. Leggett H, Sandars J, Roberts T. Twelve tips on how to provide self-regulated learning (SRL) enhanced feedback on clinical performance. Medical Teacher. 2019 Feb;41(2):147-151. [DOI]
31. Tresnadiani D, Taufik A, editors. The Development and Validation of Short Self-Regulation Scale (SSR) on Indonesian College Students. Proceedings of the 5th International Seminar of Public Health and Education; 2020. [DOI]
32. Gavora P, Jakešová J, Kalenda J. The Czech Validation of the Self-Regulation Questionnaire. Procedia - Social and Behavioral Sciences. 2015; 171:222-30. [DOI]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
