
Sun, Jul 26, 2026
[Archive]
Volume 15, Issue 47 (2022)
J Med Edu Dev 2022, 15(47): 36-42 |
Back to browse issues page

Ethics code: IR.TUMS.MEDICINE.REC.1400.358
![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Alizadeh M, Heidari F, Mirzazadeh A, Peighambardoust S S, Beheshtizadeh F, Angouraj Taghavi A, et al . Comparing flow experience of medical students in cognitive, behavioral, and social educational games: A quasi-experimental study. J Med Edu Dev 2022; 15 (47) :36-42
URL: http://edujournal.zums.ac.ir/article-1-1617-en.html
URL: http://edujournal.zums.ac.ir/article-1-1617-en.html
Maryam Alizadeh *1  , Fatemeh Heidari2 , Azim Mirzazadeh3 , Sana Sadat Peighambardoust4 , Fatemeh Beheshtizadeh4 , Azadeh Angouraj Taghavi4 , Alireza Saramad4 , Leila Janani5 , Gholamreza Hassanzadeh6
, Fatemeh Heidari2 , Azim Mirzazadeh3 , Sana Sadat Peighambardoust4 , Fatemeh Beheshtizadeh4 , Azadeh Angouraj Taghavi4 , Alireza Saramad4 , Leila Janani5 , Gholamreza Hassanzadeh6
, Fatemeh Heidari2 , Azim Mirzazadeh3 , Sana Sadat Peighambardoust4 , Fatemeh Beheshtizadeh4 , Azadeh Angouraj Taghavi4 , Alireza Saramad4 , Leila Janani5 , Gholamreza Hassanzadeh6
1- Education Development Center (EDC), and Medical Education Department, Tehran University of Medical Sciences, Tehran, Iran , alizade.aban@gmail.com
2- M.Sc of medical education, Virtual University of Medical Sciences, Tehran, Iran
3- 3MD, Professor at Department of Internal Medicine and Department of Medical Education, Tehran University of Medical Sciences, Tehran, Iran
4- School of medicine, Tehran University of Medical Sciences, Tehran, Iran.
5- Dep. of Biostatistics, School of Public Health, Iran University of Medical Sciences, Tehran, Iran.
6- Dep. of Neuroscience and Addiction studies, School of Advanced technologies in medicine, Tehran University of Medical Sciences, Tehran, Iran.
2- M.Sc of medical education, Virtual University of Medical Sciences, Tehran, Iran
3- 3MD, Professor at Department of Internal Medicine and Department of Medical Education, Tehran University of Medical Sciences, Tehran, Iran
4- School of medicine, Tehran University of Medical Sciences, Tehran, Iran.
5- Dep. of Biostatistics, School of Public Health, Iran University of Medical Sciences, Tehran, Iran.
6- Dep. of Neuroscience and Addiction studies, School of Advanced technologies in medicine, Tehran University of Medical Sciences, Tehran, Iran.
Full-Text [PDF 926 kb]
(1509 Downloads)
| Abstract (HTML) (3300 Views)
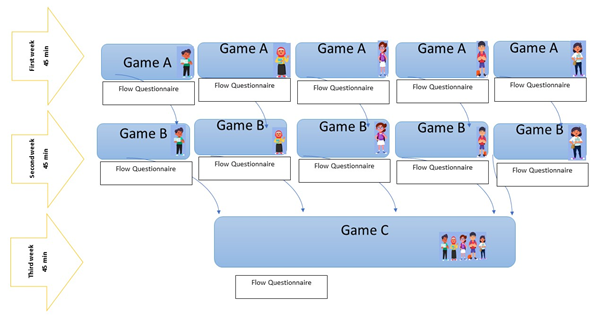
Figure 1. Intervention in a snapshot (19, 21)
Tools/Instruments
The flow experience scale developed by Pearce et al. in 2005 was used (20). The flow experience scale consists of 12 items in a 5-point Likert-type ranging from 1 (strongly disagree) to 5 (strongly agree). The scale has three subscales of enjoyment, engagement, and control. The higher the scores were, the higher the flow of experiences students would have (20). The opinions of 15 faculty members of the Tehran University of Medical Sciences were obtained to examine the content validity of the scale using the Content Validity Ratio method, both qualitatively and quantitatively in our context. They specialized in medical education (CVR=0.65). Following this, a cognitive interview with students was performed to ensure face validity (22). To ensure transparency or relevance of the instrument from the participants' viewpoint, virtual interviews with five students were held using Skype Microsoft Corp (NASDAQ: MSFT). The scale was administered to a group of 27 medical students, different from the students who participated in the main study, after a pilot educational game in an anatomy class, and the alpha coefficient was calculated (Alpha=0.76).
Data collection methods & Procedure
The three educational games were compared. We developed three Game Design Documents (GDD), a guide that is used throughout game development (23). Then, to confirm the validity of educational games, a panel of five experts in the field of medical education with experience in educational game development independently sent their suggestions on the GDDs, especially in terms of 1) Pedagogy criteria (team-based and cooperative approach for social game, problem-solving and equilibration for cognitive game, and reinforcement and punishment for behavioral game) (11), 2) Feasibility for implementation on a virtual platform, 3) Soundness and 4) Fun as the main factor that should be integrated into educational games (24). The details of the process of each game are provided in Appendix 2.
Game A (Cognitive game): This game was a word board game. Students individually advanced through the board by correctly answering the questions and solving the password of the game, which in this case was “Hippocampus”. A total of 12 questions were developed with an emphasis on content from neuroanatomy textbooks. The person who was able to guess the word in due time (even if some answers were incorrect) was the winner.
Game B (Behavioral game): This game was a quick question type one. Students had a time limitation (45 min) to get scores of four packages ordered by the level of precedence; Bronze (40 Multiple Choice Questions each with 50 scores), Silver (40 short answer questions each with 100 scores), Golden (20 long answer questions each with 200 scores) and Diamond (four case scenarios required analysis and problem-solving each with 400 scores). Wrong answers had negative points and the winner was who could get 7,000 points. All questions were developed with an emphasis on content from neuroanatomy. This game was an individual endeavor (Figure 1).
Game C (Social game): The social game had three parts, including a maze, an information store, and a case. Firstly, teams (4-5 members) played a maze for 5 min to get some information and hints, in predefined milestones plus coins that would help them to solve the case in the final part. Then, a brief history of the case was presented to the team. After that, they entered the information store to wisely pay some coins and buy the required information needed to solve the case. For instance, test results, more signs or symptoms, normal/abnormal MRI, angiography results, guidance, and basic science knowledge. Finally, they had to analyze and synthesize all information together and solve the case. All three parts required a team-based discussion, shared decision-making, and cooperation to advance game C.
Based on Gall and Gall and Borg the interaction of background, growth, and selection is time-dependent and was not considered a threatening factor in the present study. However, test effect and attrition can be viewed as threats to internal validity (25). In the current study for all three types of games, we used the same questionnaire, to control the effect of test-wiseness threat, we defined a one-week washout time between each game and also emphasized that students should fill out the questionnaire about their specific experience based on each game. Attrition means the drop of students due to absence or avoidance of participation in the study, to avoid the attrition effect we considered a 15% attrition rate, and reached 45 participants for the final sample size. A major threat to the external validity of this study was the interference of multiple experimental procedures. In the sense that the effectiveness or non-execution of one game type may be affected by the execution or non-execution of another game type, to control this effect we had a one-week washout time and students were asked to fill out the questionnaire immediately after playing each game. A detailed description of the intervention process was provided to increase external validity based on Gall's recommendation (25).
Data analysis
Statistical analysis was carried out in SPSS (version 25; IBM SPSS Statistics). This design was complete and normal because the number of observations in all levels was equal (one sample repeated all interventions), Data were presented using the mean (SD). the repeated-measures ANOVA was used for the comparisons of the three games. In this case, the assumption of sphericity was assessed by Mauchly’s test, and then, to correct any deviation from the assumption, the Greenhouse–Geisser correction was applied. A P-value less than 0.05 was considered statistically significant.
Results
Thirty-nine medical students took part in three educational games and completed the questionnaires. Respondents’ age mean was 20.58 (SD=1.82), 20(51.3%) were male and 19(48.70%) were female. The grade point average was 17.83 (SD=1.15). All participants represented eight learning teams for the social game. Seven teams had five members and one team had four members (Table 1).
Table 1: Demographics of Second-Year Medical Students, Tehran University of Medical Sciences
No evidence showed that the flow experience of medical students differs when they play cognitive, behavioral, or social educational games. The mean of flow was 42.59(SD=4.20) for cognitive, 43.15(SD=4.63) for behavioral, and 43.74(SD=5.99) for the social game (F=0.87, P=0.40). The repeated measure test showed that the mean of students’ scores on subdomains of flow experience (enjoyment, engagement, and control) did not differ significantly in the three games. The mean was 15.87(SD=1.99) in the enjoyment subscale for the cognitive game, 16.54(SD=1.93) for the behavioral game, and 16.61(SD=2.55) for the social game (F=2.34, P=0.10). In the engagement subscale, the mean was 11.90(SD=1.55) for the cognitive game, 11.47(SD=1.52) for the behavioral game, and 12.08(SD=1.38) for the social game (F=0.78, P=0.46) and in control subscale the mean was 14.82 (SD=2.14) for cognitive, 14.87 (SD=2.45) for behavioral, and 15.05 (SD=2.96) for the social game (F=0.14, P=0.82) (Table 2).
Discussion
This study using a quasi-experimental model, explored the difference in the flow experience and its subscales (engagement, enjoyment, and control) of medical students when playing cognitive, behavioral, or social educational games. We hypothesized that flow experience and its subscales would differ in three types of educational games based on a pedagogical perspective. Although the effect of the educational pedagogy of a game on flow experience had been anticipated, we found none. Many variables contribute to flow experience; however, fun, level of difficulty, and challenges are among the most important ones. Jongwoo Kim (2015) states that fun is the key element to inducing the flow and emotional fun is the most effective compared to the other types (cognitive and social). Most likely, Fun overcomes the theoretical foundation of a game to induce the flow (26). Furthermore, our games were adapted to perform in a virtual platform due to social distancing restrictions, consequently, results may have been different if the interventions occurred face to face. However, an alternative explanation is using only one group to measure the effects of the interventions on flow experience. Results may have been different if three different groups were allocated to each game. Based on the results of this study, we observed that the different dimensions of flow (i.e., engagement, control, and enjoyment) are not statistically significant in the three types of games. It seems that all three types of games have brought a high level of engagement, a sense of control over learning, and a high level of enjoyment for students. Barzilia and Blau showed that if the student has a state of flow experience during the learning activity, there is a high probability that learning the content will also happen (27). There is a systematic review investigating flow experiences in educational games. Five studies included and reported positive results regarding the impact of immersion in the learning activities. This study did not report which subscales of flow in educational games resulted in a positive effect, or which characteristics were the result of this positive effect (28). The most important question in the current study is that if the fundamental pedagogy of a game does not lead to change in the flow state, what good is it? And what happens if the game developers do not use any pedagogy of learning? In the game literature, the flow is the potential element for learning, motivation, and immersion in the learning activity. Moreover, it must be valuable that we consider the other aspects of using the pedagogy of learning for game development. From what we learned from this study, the behavioral and cognitive games required recognizing and remembering knowledge; however, in the social game, students were supposed to construct knowledge, cooperate, use hints, gather information, and integrate team knowledge to advance through the game. The learning vibe of the social game was cooperative. Additionally, students were able to fill their gaps of knowledge in a team-based context like the other team-based learning activities (29). In other words, students learn new knowledge, while taking part in a social game. All games were fun, exciting, and enjoyable, as Paulo R. Shiroma states that playing games enhance enjoyment (30). Medical students were more active during the social game. Studies have shown that students engaging in a social context of learning (i.e., educational games) enhances their competence to practice as team members (31).
Considering that the current research deals with the design of non-digital educational games, future studies could be conducted on digital games. There is a need to compare the effectiveness, time requirement, impact on learning, and acceptance of these games by students and teachers. In the current study, the game was played on a virtual platform due to covid-19 restrictions. It is proposed to make comparisons with respect to playing games in face-to-face sessions. Other effects of game types on motivation and learning are suggested for further research.
The major strengths of the current study are grounding in educational theories and applying three pedagogies of learning for developing educational games. This study has some limitations. Firstly, there was no control group and one group took part in all three games; therefore, to reduce this limitation, a one-week washout was considered to reduce the effects of interactions between three interventions (three games) as a treatment of internal validity. Secondly, the study was performed in a virtual learning platform (BigBlueButton), and this may affect the flow experience of medical students. Thirdly, the games were used as an additional learning activity to the main teaching course. As Akl et al. recommended in their review, medical educators should be careful whether the game is helping to reach educational objectives (24). Finally, the other aspects of the intervention on the learning outcomes (e.g., actual learning and higher-order thinking abilities) were not measured.
Conclusion
Based on the findings of the present research, the flow experience did not differ in the three educational games. Moreover, we observed that the different dimensions of flow (engagement, control, and enjoyment) were not statistically significant in the three types of games. It seems that all three types of games have brought a high level of engagement, a sense of control over learning, and a high level of enjoyment for students. Considering medical students have to pass various comprehensive exams they are generally focused on learning biomedical science, which was important in designing our behavioral and cognitive games. With the primary focus on the development of competencies for the practice of medicine in medical education, not just knowledge, medical teachers seek ways to develop those competencies of medical students that will enhance their team skills. Becoming a member of a healthcare team requires a host of skills, including the ability to engage in shared decision-making. The social game experience could be seen as a “learning ground” for enabling these skills.
Ethical Considerations
The Ethical Review Board of the Tehran University of Medical Sciences Medical School approved the study (IR.TUMS.MEDICINE.REC.1400.358). Prior to the study, all participants received information about the study from their representatives and signed an informed consent form. They were assured of confidentiality and anonymity when the findings were used for discussions or publications in any form. The students were free to withdraw from the study at any time. Data were used for educational research purposes only.
Acknowledgments
We thank all medical students who participated in our study and all faculty members who reviewed the GGDs. We also appreciate Mis Ameneh Ebrahimi for her helpful contribution to the statistical analyses of the data.
Conflict of Interest
All authors report no Conflict of interest.
Funding
Tehran University of medical Sciences, School of Medicine.
Full-Text: (1480 Views)
Abstract
Background & Objective: This study contributed to the current body of literature on educational games by comparing medical students’ flow experience in three types of educational games developed based on three learning theories: behavioral, cognitive, and social.
Materials & Methods: A quasi-experimental repeated measure design was employed. A total of 39 second-year medical students played three neuroanatomy educational games developed based on cognitive, behavioral, and social learning theories. At the end of each game, students completed a standard flow experience scale developed by Pearce et al. (2005) with Content Validity Ratio=0.65 and Alpha=0.76 in our context. The repeated-measures ANOVA was used for the comparisons of three games.
Results: No evidence was found to indicate that the flow experience of medical students differs when they play cognitive, behavioral, or social educational games (P=0.40). The repeated measure test showed that the mean of students’ scores on subdomains of flow experience (Enjoyment (P=0.10), engagement (P=0.46), and control (P=0.82) did not differ significantly in three different games.
Conclusion: Based on the results of this study, it was observed that the different dimensions of flow (i.e., engagement, control, and enjoyment) are not statistically significant in the three types of games. It seems that all three types of games have brought a high level of engagement, a sense of control over learning, and a high level of enjoyment for students. However, considering the lessons learned from this intervention, the social game could be seen as a “learning ground” for enabling a host of skills, including the ability to engage in shared decision-making in teams.
Background & Objective: This study contributed to the current body of literature on educational games by comparing medical students’ flow experience in three types of educational games developed based on three learning theories: behavioral, cognitive, and social.
Materials & Methods: A quasi-experimental repeated measure design was employed. A total of 39 second-year medical students played three neuroanatomy educational games developed based on cognitive, behavioral, and social learning theories. At the end of each game, students completed a standard flow experience scale developed by Pearce et al. (2005) with Content Validity Ratio=0.65 and Alpha=0.76 in our context. The repeated-measures ANOVA was used for the comparisons of three games.
Results: No evidence was found to indicate that the flow experience of medical students differs when they play cognitive, behavioral, or social educational games (P=0.40). The repeated measure test showed that the mean of students’ scores on subdomains of flow experience (Enjoyment (P=0.10), engagement (P=0.46), and control (P=0.82) did not differ significantly in three different games.
Conclusion: Based on the results of this study, it was observed that the different dimensions of flow (i.e., engagement, control, and enjoyment) are not statistically significant in the three types of games. It seems that all three types of games have brought a high level of engagement, a sense of control over learning, and a high level of enjoyment for students. However, considering the lessons learned from this intervention, the social game could be seen as a “learning ground” for enabling a host of skills, including the ability to engage in shared decision-making in teams.
Introduction
Numerous positive outcomes have been linked to well-designed, robust educational games such as motivation, satisfaction, engagement, joy, captivation, immersion, creativity, and problem-solving (1-6). Currently, the relationship between flow experience and the mentioned outcomes is under investigation in educational games in higher education, mostly outside the field of medical education (7-9). Flow experience according to Csikszentmihalyi’s theory (1996) is a state of full immersion with enjoyment in a learning activity or complete absorption in what a person (i.e., a student) do. To put it in other words, flow experience means deep involvement in the current moment. From the perspective of Beylefeld, the theory of flow experience is a well-known framework for studying game-based learning activities (3).
The selection of a pedagogical perspective is among the concerns about designing educational games. Game developers are, generally, focused on practical and mechanical aspects of the games; however, theoretical foundation aspects are neglected. Based on what we know from the related literature, if learning theories are utilized, the educational effect of games can be magnified. Moreover, from a review of the related literature, it is apparent that different pedagogical theories can underlie educational games: behavioral, cognitive, and social (10). Nowadays, these learning theories are widely used in medical education (11). Cognitive learning theories portray learning as a mental process, concerning information processing and perception. Social theories of learning explain learning as a team-based activity. Behavioral learning theories explore the way a stimulus can shape behavior, focusing on reinforcement and punishment (11).
Although several studies have investigated medical students’ attitudes, knowledge, skills, satisfaction, experience, and acceptance of educational games (12-16), only a limited number of studies investigated the flow experience of medical students in a game-based learning environment (3, 17, 18). However, these studies did not compare flow experience in three types of educational games based on a pedagogical perspective (7). Therefore, our research question arises: Is flow experience and its subscales (engagement, enjoyment, and control) different when medical students play cognitive, behavioral, or social educational games?
Materials & Methods
Design and setting(s)
The study took place at the Tehran University of Medical Sciences, Tehran, Iran, during 2020-2021. Based on the research question and considering the feasibility of the study in our setting, we adapted a quasi-experimental repeated measure design.
Participants and sampling
Repeated measures enable assessment of within-person change over time/over experiments (19). A group of randomly selected (based on a random number table) second-year medical students played three educational games developed based on cognitive, behavioral, and social learning theories. At the end of each game, students completed the flow experience scale (20). Due to the mandates of social distancing of Covid-19, a virtual platform “BigBlueBotton” with breakout rooms was used to run the games. Sessions were facilitated by four trained and experienced senior medical students. The content was neuroanatomy and there was one-week washout period. The order of the games was determined by lottery (cognitive, behavioral, and social). A snapshot of the design of this intervention is provided in Figure 1.
Sampling method and sample size
The required sample size was calculated as 38 to have 90% power for detecting a medium effect size=0.25. Considering a 15% attrition rate, we reached 45 participants, out of 110 for the final sample size. The G-power software was used for sample size calculation and medical students were recruited by random table numbers.
Inclusion and exclusion criteria
All second-year medical students who passed the nervous system block (one of the blocks of the basic sciences course) were included in the present study. As flow experience was the main variable in our study, exclusion criteria were any condition that could have an impact on this state based on the self-report form (Appendix 1). Furthermore, those who were not able to participate in all three games were excluded. the self-report form was completed by all participants 24 h before implementing the games. There was no case for exclusion.
Numerous positive outcomes have been linked to well-designed, robust educational games such as motivation, satisfaction, engagement, joy, captivation, immersion, creativity, and problem-solving (1-6). Currently, the relationship between flow experience and the mentioned outcomes is under investigation in educational games in higher education, mostly outside the field of medical education (7-9). Flow experience according to Csikszentmihalyi’s theory (1996) is a state of full immersion with enjoyment in a learning activity or complete absorption in what a person (i.e., a student) do. To put it in other words, flow experience means deep involvement in the current moment. From the perspective of Beylefeld, the theory of flow experience is a well-known framework for studying game-based learning activities (3).
The selection of a pedagogical perspective is among the concerns about designing educational games. Game developers are, generally, focused on practical and mechanical aspects of the games; however, theoretical foundation aspects are neglected. Based on what we know from the related literature, if learning theories are utilized, the educational effect of games can be magnified. Moreover, from a review of the related literature, it is apparent that different pedagogical theories can underlie educational games: behavioral, cognitive, and social (10). Nowadays, these learning theories are widely used in medical education (11). Cognitive learning theories portray learning as a mental process, concerning information processing and perception. Social theories of learning explain learning as a team-based activity. Behavioral learning theories explore the way a stimulus can shape behavior, focusing on reinforcement and punishment (11).
Although several studies have investigated medical students’ attitudes, knowledge, skills, satisfaction, experience, and acceptance of educational games (12-16), only a limited number of studies investigated the flow experience of medical students in a game-based learning environment (3, 17, 18). However, these studies did not compare flow experience in three types of educational games based on a pedagogical perspective (7). Therefore, our research question arises: Is flow experience and its subscales (engagement, enjoyment, and control) different when medical students play cognitive, behavioral, or social educational games?
Materials & Methods
Design and setting(s)
The study took place at the Tehran University of Medical Sciences, Tehran, Iran, during 2020-2021. Based on the research question and considering the feasibility of the study in our setting, we adapted a quasi-experimental repeated measure design.
Participants and sampling
Repeated measures enable assessment of within-person change over time/over experiments (19). A group of randomly selected (based on a random number table) second-year medical students played three educational games developed based on cognitive, behavioral, and social learning theories. At the end of each game, students completed the flow experience scale (20). Due to the mandates of social distancing of Covid-19, a virtual platform “BigBlueBotton” with breakout rooms was used to run the games. Sessions were facilitated by four trained and experienced senior medical students. The content was neuroanatomy and there was one-week washout period. The order of the games was determined by lottery (cognitive, behavioral, and social). A snapshot of the design of this intervention is provided in Figure 1.
Sampling method and sample size
The required sample size was calculated as 38 to have 90% power for detecting a medium effect size=0.25. Considering a 15% attrition rate, we reached 45 participants, out of 110 for the final sample size. The G-power software was used for sample size calculation and medical students were recruited by random table numbers.
Inclusion and exclusion criteria
All second-year medical students who passed the nervous system block (one of the blocks of the basic sciences course) were included in the present study. As flow experience was the main variable in our study, exclusion criteria were any condition that could have an impact on this state based on the self-report form (Appendix 1). Furthermore, those who were not able to participate in all three games were excluded. the self-report form was completed by all participants 24 h before implementing the games. There was no case for exclusion.
Figure 1. Intervention in a snapshot (19, 21)
Tools/Instruments
The flow experience scale developed by Pearce et al. in 2005 was used (20). The flow experience scale consists of 12 items in a 5-point Likert-type ranging from 1 (strongly disagree) to 5 (strongly agree). The scale has three subscales of enjoyment, engagement, and control. The higher the scores were, the higher the flow of experiences students would have (20). The opinions of 15 faculty members of the Tehran University of Medical Sciences were obtained to examine the content validity of the scale using the Content Validity Ratio method, both qualitatively and quantitatively in our context. They specialized in medical education (CVR=0.65). Following this, a cognitive interview with students was performed to ensure face validity (22). To ensure transparency or relevance of the instrument from the participants' viewpoint, virtual interviews with five students were held using Skype Microsoft Corp (NASDAQ: MSFT). The scale was administered to a group of 27 medical students, different from the students who participated in the main study, after a pilot educational game in an anatomy class, and the alpha coefficient was calculated (Alpha=0.76).
Data collection methods & Procedure
The three educational games were compared. We developed three Game Design Documents (GDD), a guide that is used throughout game development (23). Then, to confirm the validity of educational games, a panel of five experts in the field of medical education with experience in educational game development independently sent their suggestions on the GDDs, especially in terms of 1) Pedagogy criteria (team-based and cooperative approach for social game, problem-solving and equilibration for cognitive game, and reinforcement and punishment for behavioral game) (11), 2) Feasibility for implementation on a virtual platform, 3) Soundness and 4) Fun as the main factor that should be integrated into educational games (24). The details of the process of each game are provided in Appendix 2.
Game A (Cognitive game): This game was a word board game. Students individually advanced through the board by correctly answering the questions and solving the password of the game, which in this case was “Hippocampus”. A total of 12 questions were developed with an emphasis on content from neuroanatomy textbooks. The person who was able to guess the word in due time (even if some answers were incorrect) was the winner.
Game B (Behavioral game): This game was a quick question type one. Students had a time limitation (45 min) to get scores of four packages ordered by the level of precedence; Bronze (40 Multiple Choice Questions each with 50 scores), Silver (40 short answer questions each with 100 scores), Golden (20 long answer questions each with 200 scores) and Diamond (four case scenarios required analysis and problem-solving each with 400 scores). Wrong answers had negative points and the winner was who could get 7,000 points. All questions were developed with an emphasis on content from neuroanatomy. This game was an individual endeavor (Figure 1).
Game C (Social game): The social game had three parts, including a maze, an information store, and a case. Firstly, teams (4-5 members) played a maze for 5 min to get some information and hints, in predefined milestones plus coins that would help them to solve the case in the final part. Then, a brief history of the case was presented to the team. After that, they entered the information store to wisely pay some coins and buy the required information needed to solve the case. For instance, test results, more signs or symptoms, normal/abnormal MRI, angiography results, guidance, and basic science knowledge. Finally, they had to analyze and synthesize all information together and solve the case. All three parts required a team-based discussion, shared decision-making, and cooperation to advance game C.
Based on Gall and Gall and Borg the interaction of background, growth, and selection is time-dependent and was not considered a threatening factor in the present study. However, test effect and attrition can be viewed as threats to internal validity (25). In the current study for all three types of games, we used the same questionnaire, to control the effect of test-wiseness threat, we defined a one-week washout time between each game and also emphasized that students should fill out the questionnaire about their specific experience based on each game. Attrition means the drop of students due to absence or avoidance of participation in the study, to avoid the attrition effect we considered a 15% attrition rate, and reached 45 participants for the final sample size. A major threat to the external validity of this study was the interference of multiple experimental procedures. In the sense that the effectiveness or non-execution of one game type may be affected by the execution or non-execution of another game type, to control this effect we had a one-week washout time and students were asked to fill out the questionnaire immediately after playing each game. A detailed description of the intervention process was provided to increase external validity based on Gall's recommendation (25).
Data analysis
Statistical analysis was carried out in SPSS (version 25; IBM SPSS Statistics). This design was complete and normal because the number of observations in all levels was equal (one sample repeated all interventions), Data were presented using the mean (SD). the repeated-measures ANOVA was used for the comparisons of the three games. In this case, the assumption of sphericity was assessed by Mauchly’s test, and then, to correct any deviation from the assumption, the Greenhouse–Geisser correction was applied. A P-value less than 0.05 was considered statistically significant.
Results
Thirty-nine medical students took part in three educational games and completed the questionnaires. Respondents’ age mean was 20.58 (SD=1.82), 20(51.3%) were male and 19(48.70%) were female. The grade point average was 17.83 (SD=1.15). All participants represented eight learning teams for the social game. Seven teams had five members and one team had four members (Table 1).
Table 1: Demographics of Second-Year Medical Students, Tehran University of Medical Sciences
| Gender | Age | GPA | |
| female | male | Mean (SD) | Mean (SD) |
| Frequency (%) | Frequency (%) | ||
| 19 (48.7) | 20 (51.3) | 20.58 (1.82) | 17.83 (1.15) |
No evidence showed that the flow experience of medical students differs when they play cognitive, behavioral, or social educational games. The mean of flow was 42.59(SD=4.20) for cognitive, 43.15(SD=4.63) for behavioral, and 43.74(SD=5.99) for the social game (F=0.87, P=0.40). The repeated measure test showed that the mean of students’ scores on subdomains of flow experience (enjoyment, engagement, and control) did not differ significantly in the three games. The mean was 15.87(SD=1.99) in the enjoyment subscale for the cognitive game, 16.54(SD=1.93) for the behavioral game, and 16.61(SD=2.55) for the social game (F=2.34, P=0.10). In the engagement subscale, the mean was 11.90(SD=1.55) for the cognitive game, 11.47(SD=1.52) for the behavioral game, and 12.08(SD=1.38) for the social game (F=0.78, P=0.46) and in control subscale the mean was 14.82 (SD=2.14) for cognitive, 14.87 (SD=2.45) for behavioral, and 15.05 (SD=2.96) for the social game (F=0.14, P=0.82) (Table 2).
Table 2. Flow experience and its subscales of second year medical students in Cognitive, Behavioral and Social educational games
| Enjoyment | Engagement | Control | Flow | |
| Cognitive | 15.87(1.99) | 11.90(1.55) | 14.82(2.14) | 42.59(4.20) |
| Behavioral | 16.54(1.93) | 11.74(1.52) | 14.87(2.45) | 43.15(4.63) |
| Social | 16.61(2.55) | 12.08(1.38) | 15.05(2.96) | 43.74(5.99) |
| Mauchly's Test of Sphericity (Mauchly's W, P-value) | 0.88 , 0.10 | 0.86 , 0.06 | 0.75 , 0.005 | 0.78 , 0.01 |
| Tests of Within-Subjects Effects (F, P-value*) | 2.34 , 0.10 | 0.78 , 0.46 | 0.14 , 0.82 | 0.87 , 0.40 |
*P-value was reported based on Mauchly's Test, if p-value of Mauchly's W was less than 0.05, Greenhouse-Geisser was assumed
Discussion
This study using a quasi-experimental model, explored the difference in the flow experience and its subscales (engagement, enjoyment, and control) of medical students when playing cognitive, behavioral, or social educational games. We hypothesized that flow experience and its subscales would differ in three types of educational games based on a pedagogical perspective. Although the effect of the educational pedagogy of a game on flow experience had been anticipated, we found none. Many variables contribute to flow experience; however, fun, level of difficulty, and challenges are among the most important ones. Jongwoo Kim (2015) states that fun is the key element to inducing the flow and emotional fun is the most effective compared to the other types (cognitive and social). Most likely, Fun overcomes the theoretical foundation of a game to induce the flow (26). Furthermore, our games were adapted to perform in a virtual platform due to social distancing restrictions, consequently, results may have been different if the interventions occurred face to face. However, an alternative explanation is using only one group to measure the effects of the interventions on flow experience. Results may have been different if three different groups were allocated to each game. Based on the results of this study, we observed that the different dimensions of flow (i.e., engagement, control, and enjoyment) are not statistically significant in the three types of games. It seems that all three types of games have brought a high level of engagement, a sense of control over learning, and a high level of enjoyment for students. Barzilia and Blau showed that if the student has a state of flow experience during the learning activity, there is a high probability that learning the content will also happen (27). There is a systematic review investigating flow experiences in educational games. Five studies included and reported positive results regarding the impact of immersion in the learning activities. This study did not report which subscales of flow in educational games resulted in a positive effect, or which characteristics were the result of this positive effect (28). The most important question in the current study is that if the fundamental pedagogy of a game does not lead to change in the flow state, what good is it? And what happens if the game developers do not use any pedagogy of learning? In the game literature, the flow is the potential element for learning, motivation, and immersion in the learning activity. Moreover, it must be valuable that we consider the other aspects of using the pedagogy of learning for game development. From what we learned from this study, the behavioral and cognitive games required recognizing and remembering knowledge; however, in the social game, students were supposed to construct knowledge, cooperate, use hints, gather information, and integrate team knowledge to advance through the game. The learning vibe of the social game was cooperative. Additionally, students were able to fill their gaps of knowledge in a team-based context like the other team-based learning activities (29). In other words, students learn new knowledge, while taking part in a social game. All games were fun, exciting, and enjoyable, as Paulo R. Shiroma states that playing games enhance enjoyment (30). Medical students were more active during the social game. Studies have shown that students engaging in a social context of learning (i.e., educational games) enhances their competence to practice as team members (31).
Considering that the current research deals with the design of non-digital educational games, future studies could be conducted on digital games. There is a need to compare the effectiveness, time requirement, impact on learning, and acceptance of these games by students and teachers. In the current study, the game was played on a virtual platform due to covid-19 restrictions. It is proposed to make comparisons with respect to playing games in face-to-face sessions. Other effects of game types on motivation and learning are suggested for further research.
The major strengths of the current study are grounding in educational theories and applying three pedagogies of learning for developing educational games. This study has some limitations. Firstly, there was no control group and one group took part in all three games; therefore, to reduce this limitation, a one-week washout was considered to reduce the effects of interactions between three interventions (three games) as a treatment of internal validity. Secondly, the study was performed in a virtual learning platform (BigBlueButton), and this may affect the flow experience of medical students. Thirdly, the games were used as an additional learning activity to the main teaching course. As Akl et al. recommended in their review, medical educators should be careful whether the game is helping to reach educational objectives (24). Finally, the other aspects of the intervention on the learning outcomes (e.g., actual learning and higher-order thinking abilities) were not measured.
Conclusion
Based on the findings of the present research, the flow experience did not differ in the three educational games. Moreover, we observed that the different dimensions of flow (engagement, control, and enjoyment) were not statistically significant in the three types of games. It seems that all three types of games have brought a high level of engagement, a sense of control over learning, and a high level of enjoyment for students. Considering medical students have to pass various comprehensive exams they are generally focused on learning biomedical science, which was important in designing our behavioral and cognitive games. With the primary focus on the development of competencies for the practice of medicine in medical education, not just knowledge, medical teachers seek ways to develop those competencies of medical students that will enhance their team skills. Becoming a member of a healthcare team requires a host of skills, including the ability to engage in shared decision-making. The social game experience could be seen as a “learning ground” for enabling these skills.
Ethical Considerations
The Ethical Review Board of the Tehran University of Medical Sciences Medical School approved the study (IR.TUMS.MEDICINE.REC.1400.358). Prior to the study, all participants received information about the study from their representatives and signed an informed consent form. They were assured of confidentiality and anonymity when the findings were used for discussions or publications in any form. The students were free to withdraw from the study at any time. Data were used for educational research purposes only.
Acknowledgments
We thank all medical students who participated in our study and all faculty members who reviewed the GGDs. We also appreciate Mis Ameneh Ebrahimi for her helpful contribution to the statistical analyses of the data.
Conflict of Interest
All authors report no Conflict of interest.
Funding
Tehran University of medical Sciences, School of Medicine.
Article Type : Orginal Research |
Received: 2022/05/26 | Accepted: 2022/11/25 | Published: 2022/12/19
Received: 2022/05/26 | Accepted: 2022/11/25 | Published: 2022/12/19
References
1. Abdulmajed H, Park YS, Tekian A. Assessment of educational games for health professions: A systematic review of trends and outcomes. Medical Teacher. 2015;37(sup1):S27-S32. [DOI]
2. Aksoy E. Comparing the effects on learning outcomes of tablet-based and virtual reality–based serious gaming modules for basic life support training: randomized trial. JMIR serious games. 2019;7(2):e13442. [DOI]
3. Beylefeld AA, Struwig MC. A gaming approach to learning medical microbiology: students’ experiences of flow. Medical Teacher. 2007;29(9-10):933-40. [DOI]
4. Cheng M-T, Annetta L. Students’ learning outcomes and learning experiences through playing a Serious Educational Game. Journal of Biological Education. 2012;46(4):203-13. [DOI]
5. Ober CP. Examination outcomes following use of card games for learning radiographic image quality in veterinary medicine. Journal of Veterinary Medical Education. 2018;45(1):140-4. [DOI]
6. Teng YY, Chou WC, Cheng MT. Learning immunology in a game: Learning outcomes, the use of player characters, immersion experiences and visual attention distributions. Journal of Computer Assisted Learning. 2020. [DOI]
7. Perttula A, Kiili K, Lindstedt A, Tuomi P. Flow experience in game based learning–a systematic literature review. International Journal of Serious Games. 2017;4(1):57-72. [DOI]
8. Erhel S, Jamet E. Improving instructions in educational computer games: Exploring the relations between goal specificity, flow experience and learning outcomes. Computers in Human Behavior. 2019;91:106-14. [DOI]
9. Peifer C, Tan J. The psychophysiology of flow experience. Advances in flow research: Springer; 2021. p. 191-230.
10. Gorbanev I, Agudelo-Londoño S, González RA, Cortes A, Pomares A, Delgadillo V, et al. A systematic review of serious games in medical education: quality of evidence and pedagogical strategy. Medical Education Online. 2018;23(1):1438718. [DOI]
11. Taylor DCM, Hamdy H. Adult learning theories: Implications for learning and teaching in medical education: AMEE Guide No. 83. Medical Teacher. 2013;35(11):e1561-e72. [DOI]
12. Tsopra R, Courtine M, Sedki K, Eap D, Cabal M, Cohen S, et al. AntibioGame®: A serious game for teaching medical students about antibiotic use. International Journal of Medical Informatics. 2020;136:104074. [DOI]
13. Palee P, Wongta N, Khwanngern K, Jitmun W, Choosri N. Serious Game for Teaching Undergraduate Medical Students in Cleft lip and Palate Treatment Protocol. International Journal of Medical Informatics. 2020;141:104166. [DOI]
14. Agudelo-Londoño S, Gorbanev I, Delgadillo V, Muñoz Ó, Cortes A, González RA, et al. Development and Evaluation of a Serious Game for Teaching ICD-10 Diagnosis Coding to Medical Students. Games for health journal. 2019;8(5):349-56. [DOI]
15. Felszeghy S, Pasonen-Seppänen S, Koskela A, Nieminen P, Härkönen K, Paldanius KMA, et al. Using online game-based platforms to improve student performance and engagement in histology teaching. BMC Med Educ. 2019;19(1):273. [DOI]
16. Hill RV, Nassrallah Z. A Game-Based Approach to Teaching and Learning Anatomy of the Liver and Portal Venous System. MedEdPORTAL. 2018;14:10696. [DOI]
17. Larche CJ, Dixon MJ. The relationship between the skill-challenge balance, game expertise, flow and the urge to keep playing complex mobile games. Journal of behavioral addictions. 2020;9(3):606-16. [DOI]
18. Yeh YC, Chen SY, Rega EM, Lin CS. Mindful Learning Experience Facilitates Mastery Experience Through Heightened Flow and Self-Efficacy in Game-Based Creativity Learning. Frontiers in psychology. 2019;10:1593. [DOI]
19. Maciejewski ML. Quasi-experimental design. Biostatistics & Epidemiology. 2020;4(1):38-47. [DOI]
20. Pearce JM, Ainley M, Howard S. The ebb and flow of online learning. Computers in Human Behavior. 2005;21(5):745-71. [DOI]
21. Artino Jr AR, La Rochelle JS, Dezee KJ, Gehlbach H. Developing questionnaires for educational research: AMEE Guide No. 87. Medical Teacher. 2014;36(6):463-74. [DOI]
22. Colby R, Colby RS. Game design documentation: Four perspectives from independent game studios. Communication Design Quarterly Review. 2019 Nov 15;7(3):5-15. [DOI]
23. Akl EA, Pretorius RW, Sackett K, Erdley WS, Bhoopathi PS, Alfarah Z, et al. The effect of educational games on medical students’ learning outcomes: A systematic review: BEME Guide No 14. Medical Teacher. 2010;32(1):16-27. [DOI]
24. Gall MD, Gall JP, Borg WR. Educational Research: an Introduction. Pearson Education; 2003.
25. Kim J, Jung J, Kim S. The relationship of game elements, fun and flow. Indian Journal of Science and Technology. 2015;8(8):405-11. [DOI]
26. Barzilai S, Blau I. Scaffolding game-based learning: Impact on learning achievements, perceived learning, and game experiences. Computers & Education. 2014;70:65-79. [DOI]
27. Admiraal W, Huizenga J, Akkerman S, Ten Dam G. The concept of flow in collaborative game-based learning. Computers in Human Behavior. 2011;27(3):1185-94. [DOI]
28. Parmelee D, Michaelsen LK, Cook S, Hudes PD. Team-based learning: a practical guide: AMEE guide no. 65. Medical Teacher. 2012;34(5):e275-e87. [DOI]
29. Shiroma PR, Massa AA, Alarcon RD. Using game format to teach psychopharmacology to medical students. Medical Teacher. 2011;33(2):156-60. [DOI]
30. Parmelee D, Roman B, Overman I, Alizadeh M. The lecture-free curriculum: Setting the stage for life-long learning: AMEE Guide No. 135. Medical Teacher. 2020;42(9):962-9. [DOI]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
