
Wed, Jul 8, 2026
[Archive]
Volume 19, Issue 2 (2026)
J Med Edu Dev 2026, 19(2): 58-68 |
Back to browse issues page
Ethics code: IHEC-II/0963/25
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Aristotle S, aristotle S, Jayakumar S, Ramamoorthy B. Assessment of anatomy learning preferences and their association with academic performance among first-year medical students: a cross-sectional study. J Med Edu Dev 2026; 19 (2) :58-68
URL: http://edujournal.zums.ac.ir/article-1-2651-en.html
URL: http://edujournal.zums.ac.ir/article-1-2651-en.html
1- Department of Anatomy, Chettinad Hospital and Research Institute, Chettinad Academy of Research and Education, kelambakkam 603103, Tamil Nadu, India , sharmianat@gmail.com
2- Professor and head,Department of Anatomy, Chettinad Hospital and Research Institute, Chettinad Academy of Research and Education, kelambakkam 603103, Tamil Nadu, India.
3- Associate professor of anatomy,dept of maxillofacial surgery and diagnostic sciences, college of dentistry,majmaah university,AI majmaah,kingdom of saudiarabia 11952
4- 3Department of Anatomy,SRM Medical College Hospital and Research center, Faculty of medical and health sciences ,SRMIST,Kattankulathur.603203.Tamilnadu,India
2- Professor and head,Department of Anatomy, Chettinad Hospital and Research Institute, Chettinad Academy of Research and Education, kelambakkam 603103, Tamil Nadu, India.
3- Associate professor of anatomy,dept of maxillofacial surgery and diagnostic sciences, college of dentistry,majmaah university,AI majmaah,kingdom of saudiarabia 11952
4- 3Department of Anatomy,SRM Medical College Hospital and Research center, Faculty of medical and health sciences ,SRMIST,Kattankulathur.603203.Tamilnadu,India
Keywords: learning preferences, anatomy, education, medical, academic performance, kinesthetic learning
Full-Text [PDF 598 kb]
(155 Downloads)
| Abstract (HTML) (322 Views)
Full-Text: (150 Views)
Abstract
Background & Objective: Medical education requires understanding of complex anatomical structures and their functional correlations. Anatomy learning presents unique challenges, including spatial visualization, memory consolidation, and conceptual understanding. Despite competency-based curricula implementation, considerable variability persists in student anatomy performance. This study aimed to assess anatomy learning preferences among first-year MBBS students and examine their relationship with academic performance in anatomy.
Materials & Methods: A cross-sectional analytical study was conducted among 233 first-year MBBS students at the Department of Anatomy of a medical institute in Chennai, with a response rate of 93.2% (233/250). A validated 20-item questionnaire assessed four learning preference modalities: Visual-Spatial (VS), Auditory-Verbal (AV), Textual-Analytical (TA), and Tactile-Kinesthetic (TK). Academic performance was measured through formative theory and practical assessments. Statistical analyses included Spearman correlation, Kruskal-Wallis test, chi-square test, and independent t-tests.
Results: Among 233 participants, learning preference distribution was as follows: visual-spatial dominance in 30.9% (n = 72), tactile-kinesthetic in 28.3% (n = 66), auditory-verbal in 20.2% (n = 47), textual-analytical in 13.3% (n = 31), and multimodal preferences in 7.3% (n = 17). Tactile-kinesthetic preference showed a significant positive correlation with practical performance (=0.187 p =0.004 53.25±12.21 49.56±12.66 =0.047 =-0.208 =0.001 =-0.216 <0.001
Conclusion: Learning preferences, particularly kinesthetic preference, significantly influence practical anatomy performance. These findings support the continued importance of hands-on dissection and laboratory-based learning, while highlighting the inadequacy of text-based learning as a sole approach. Integration of traditional cadaveric dissection with emerging technologies and blended learning approaches offers a viable pathway for anatomy education.
Introduction
Medical education demands an understanding of complex structures and functional correlations across various subjects, forming the basis of clinical practice. Anatomy, often regarded as the foundation of medical education, presents unique challenges, requiring students to integrate multiple cognitive processes simultaneously, including spatial visualization, memory consolidation, and conceptual understanding [1, 2]. Beyond morphological characteristics, learners must comprehend the spatial relationships, functional correlations, and clinical relevance of anatomical structures, all of which are fundamental to achieving the desired level of clinical competence [3]. Despite the implementation of competency-based medical education curricula across India, student performance in anatomy continues to show considerable variability [4]. This variation in academic outcomes is greatly influenced by the learning preferences of students, the preferred modalities through which they optimally receive, process, and retain anatomical information [5]. A recent cross-sectional study conducted at a teaching hospital in Perambalur, India (2023) confirmed that kinesthetic and auditory learning remain prevalent among medical students [6], with demonstrations and interactive sessions being the preferred approaches for anatomy learning. The theoretical background for analyzing learning preferences in medical education is well-established through several cognitive frameworks. According to Paivio’s Dual Coding Theory, information is processed through both verbal and visual-spatial channels, a concept directly relevant to anatomy, where students must simultaneously integrate textual descriptions with visual representations [7]. Similarly, Sweller’s Cognitive Load Theory suggests that optimal learning occurs when teaching methods are tailored to an individual’s cognitive makeup [8]. This implies that matching instructional strategies to individual learning preferences can greatly improve student performance [9]. Dobson’s seminal work demonstrated that students with visual learning preferences exhibited better performance in anatomy practical examinations, suggesting a clear connection between preferred learning style and academic outcomes [10]. The introduction of newer teaching methodologies, including digital tools, 3D modeling, flipped classrooms, and problem-based learning, results in higher knowledge retention and student engagement compared to traditional methods, with blended teaching approaches associated with greater student satisfaction [11, 12]. Despite growing interest in personalized medical education, a research gap remains in understanding how students’ anatomy learning preferences relate to their academic performance. The majority of prior studies utilize tools that lack specific design for the unique requirements of anatomy, such as three-dimensional spatial reasoning [13]. Furthermore, while some research has been conducted within the Indian medical education context, studies specifically examining the association between learning preferences and academic performance within the current curriculum remain limited [6].
The identification and understanding of anatomy learning preferences among medical students carries meaningful implications for educational practice. Such knowledge can enable anatomy educators to adopt tailored teaching methodologies that accommodate diverse learning needs, thereby improving both student engagement and academic outcomes [14]. Additionally, this understanding serves as a useful foundation for curriculum development and supports the creation of personalized learning pathways that maximize individual student potential [15].
The aim of this study was to assess anatomy learning preferences among first-year MBBS students and analyze their relationship with academic performance in anatomy. The specific objectives were: 1) to determine the distribution of anatomy learning preferences among first-year MBBS students; 2) to investigate relationships between specific learning preferences and performance in formative anatomy assessments; 3) to examine academic performance variations across different learning preference classifications; 4) to identify demographic factors influencing anatomy learning preferences; and 5) to validate the learning preference questionnaire through statistical analysis.
Materials & Methods
Design and setting(s)
This cross-sectional analytical study was conducted at the Department of Anatomy, Chettinad Hospital and Research Institute, Chennai, Tamil Nadu, India, during the period 1 December 2024 to 31 July 2025. Data collection occurred following completion of four formative assessments, through an online questionnaire administered via Google Forms.
Participants and sampling
Census sampling was employed, whereby all 250 first-year MBBS students enrolled during the study period were invited to participate. This approach was chosen to maximize sample size, ensure comprehensive representation of the study population, and minimize selection bias. Census sampling was feasible given the manageable cohort size and allowed us to capture the full spectrum of learning preferences within this academic cohort. However, 17 students did not meet the inclusion criterion of ≥ 75% attendance; therefore, the final analysis was conducted on 233 students (Figure 1).
Inclusion criteria were as follows: 1) first-year MBBS students enrolled during the study period (1 December 2024 to 31 July 2025); 2) aged 17–22 years at the time of enrollment; 3) completed a minimum of four anatomy formative assessments (both theory and practical components) during the study period; and 4) regular attendance of ≥ 75% in anatomy courses (lectures, dissection practicals, and tutorials) as per institutional regulations.
Students were excluded if they: 1) declined consent or withdrew during data collection; or 2) had attendance below 75% in anatomy courses (n = 17).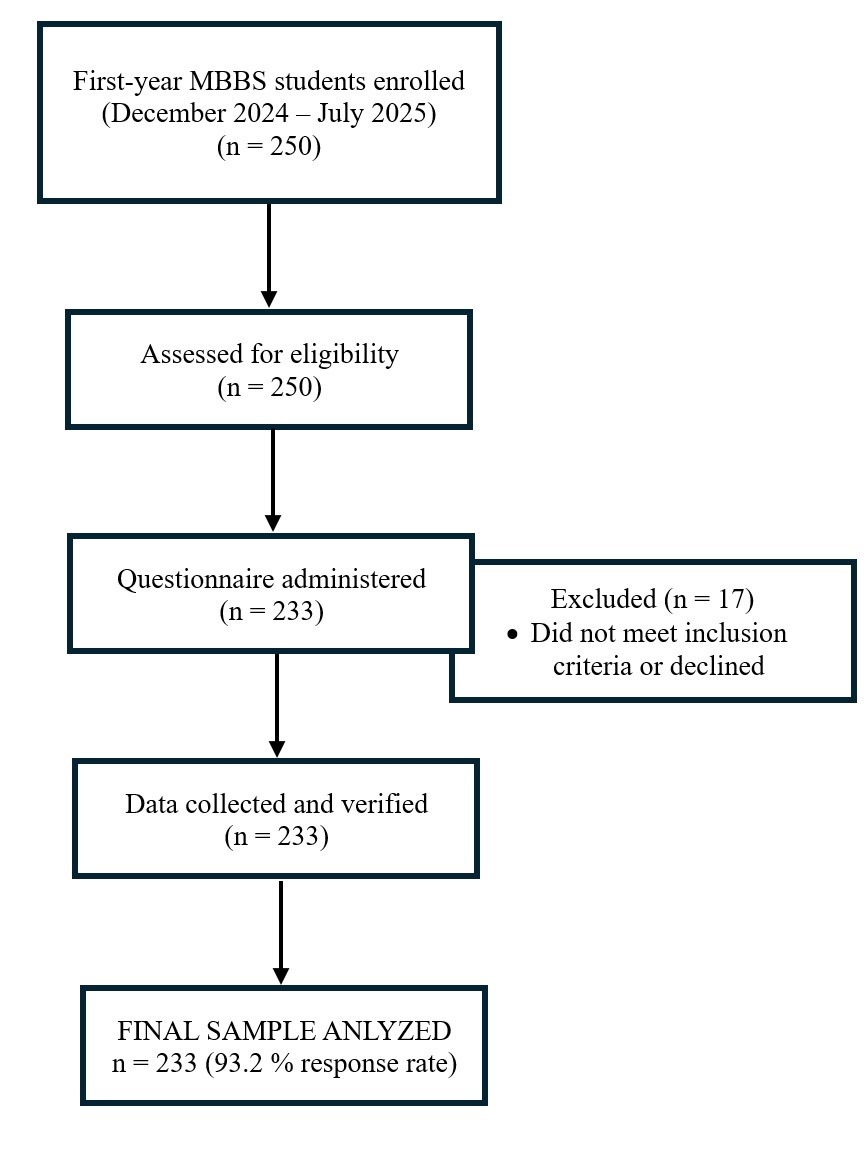
Figure 1. Flow diagram of participants through the study
Table 1. Spearman correlation matrix between learning preferences and academic performance scores
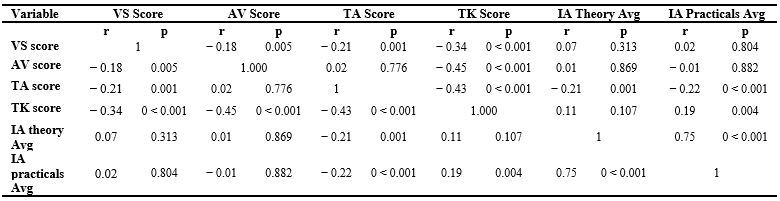
Table 2. Academic performance across dominant learning preference groups

Note: Values are presented as Mean ± SD. Kruskal-Wallis test was used to compare academic performance across dominant learning preference groups. Post hoc analysis revealed significant differences in practical performance between TA and AV groups (p = 0.045) and between TA and TK groups (p = 0.004).
Abbreviations: VS, visual-spatial; AV, auditory-verbal; TA, textual-analytical; TK, tactile-kinesthetic; IA, integrated assessment; Avg, average; n, number of participants; SD, standard deviation; p, probability value.
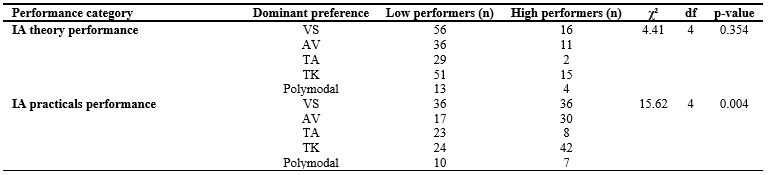
Table 3. Chi-square analysis of the association between dominant learning preference and academic performance categories
Independent samples t-tests revealed that practical-oriented learners (AV + TK dominant) achieved significantly higher practical assessment scores compared to theory-oriented learners (VS + TA dominant; p = 0.043; Table 4). Visual-dominant learners did not differ significantly from non-visual-dominant learners in either theory or practical performance (Table 5). Kinesthetic-dominant learners demonstrated significantly higher practical scores compared to non-kinesthetic-dominant learners (53.25 ± 12.21 vs. 49.56 ± 12.66; p = 0.047; Cohen’s d = 0.29), indicating a small but statistically significant effect (Table 6). The most common daily anatomy study duration reported was 1–2 hours. Students expressed a strong preference for practical demonstrations and faculty mentoring as primary learning support strategies. Memory retention was identified as the most frequently cited learning challenge, reported by 55.8% of participants.
Table 4. Comparison of academic performance between theory-oriented and practical-oriented learners

Note: Values are presented as Mean ± SD. Independent samples t-test was used for group comparisons. Polymodal learners (n = 17) were excluded from this analysis (total analyzed n = 216). Practical-oriented learners scored significantly higher in practical performance (p = 0.043); no significant difference was observed in theory performance (p = 0.558).
Abbreviations: VS, visual-spatial; AV, auditory-verbal; TA, textual-analytical; TK, tactile-kinesthetic; IA, integrated assessment; n, number of participants; SD, standard deviation; t, t-statistic; p, probability value; d, Cohen’s d effect size.
Table 5. Comparison of academic performance between visual-dominant and non-visual-dominant learners

Note: Values are presented as Mean ± SD. Independent samples t-test was used for group comparisons. Polymodal learners (n = 17) were excluded from this analysis (total analyzed N=216). No significant differences were observed in either theory (p=0.126) or practical performance (p = 0.706) between visual-dominant and non-visual-dominant learners.
Abbreviations: n, number of participants; SD, standard deviation; t, t-statistic; p, probability value; d, Cohen’s d effect size.
Table 6. Comparison of academic performance between kinesthetic-dominant and non-kinesthetic-dominant learners

The present study found that 31% of students exhibited visual-spatial dominance, 28% demonstrated tactile-kinesthetic preference, 20% showed auditory-verbal preference, 13% preferred textual-analytical learning, and 7% demonstrated multimodal preferences. These findings align with existing literature. Satapathy and Singh reported that 70% of MBBS students demonstrated unimodal learning preferences, with kinesthetic modality being the most prevalent at 34% [21]. Rawat et al. similarly identified kinesthetic learning as the dominant preference among medical undergraduates, reinforcing the notion that anatomy education is inherently oriented toward hands-on approaches [22]. The predominance of kinesthetic and visual preferences reflects the spatially demanding and practically oriented nature of anatomy as a discipline [23]. Aboregela et al. reported that 90.5% of medical students preferred kinesthetic learning, followed by 54% auditory, 34.9% visual, and 17.5% read/write modalities [24], suggesting cross-cultural consistency in learning preference distribution among medical students globally.
The most significant finding of this study was the positive correlation between tactile-kinesthetic preference and practical examination performance (=0.187 =0.004 53.25±12.21 49.56±12.66 =0.047 =0.29
The basis for superior kinesthetic outcomes in anatomy has been studied extensively. Chatha et al. concluded that physical examination of human tissues provides tactile and spatial understanding that digital tools cannot fully replicate, and that cadaveric dissection remains foundational for developing three-dimensional anatomical comprehension and clinical reasoning skills [27]. Elbeshbeishy et al. further confirmed that hands-on dissection facilitates professional identity formation fundamental to medical education [28].
A noteworthy finding was the negative correlation between textual-analytical preference and both theory (=-0.208 =0.001 =-0.216 p <0.001
However, the cross-sectional design of this study prevents establishing causality. Two interpretations are plausible: first, text-based learning may be insufficient for mastering anatomy’s spatial demands, as suggested by Martinez et al. [29]; second, students struggling with anatomy may compensate by increasing reading, making textual preference a consequence rather than a cause of poor performance. Regardless of causal direction, students with strong textual preferences warrant educational attention, either to diversify their learning approaches or to address underlying spatial reasoning difficulties. Medical educators should identify these students early and provide explicit instruction in visual-spatial and kinesthetic strategies. Longitudinal research measuring baseline preferences before anatomy instruction is needed to clarify this relationship. Contrary to initial expectations, this study found no significant performance advantage for students with multimodal learning preferences compared to those with unimodal preferences (theory:=0.627 =0.634
The study revealed that 61% of students used digital resources frequently, with 49% preferring online videos as their primary digital learning tool. Nevertheless, 51% still preferred offline resources, indicating that traditional methods retain significant value and that optimal anatomy education should embrace a blended approach combining the strengths of both traditional and modern pedagogies. Recent systematic reviews support this conclusion. Nebot-Cegarra et al. conducted a comparative analysis of face-to-face and e-learning methodologies in medical anatomy education and found that blended learning approaches produced superior academic results compared to either method alone [36]. While virtual reality and augmented reality are increasingly recognized as valuable supplements to traditional dissection, Chatha et al. emphasized that these technologies should complement rather than replace cadaveric dissection, as the tactile experience remains irreplaceable for comprehensive anatomical understanding [27].
The cross-sectional design provides only a snapshot of learning preferences and performance at a single point in time, limiting the ability to assess how these relationships evolve as students progress through medical training. Longitudinal studies tracking students across multiple years would provide more robust evidence regarding the stability of learning preferences and their long-term influence on academic and clinical performance.
Academic performance was restricted to formative internal assessments and may not reflect performance in summative examinations, clinical settings, or long-term knowledge retention. Furthermore, practical assessments emphasizing specimen identification may have inherently favored kinesthetic and visual learners, potentially introducing assessment bias. The study was conducted at a single institution, and some preference groups had limited sample sizes (TA dominant:=31 =17
Conclusion
This study provides evidence that learning preferences, particularly kinesthetic preference, are significantly associated with practical anatomy performance among first-year medical students. The findings support the continued importance of hands-on dissection and laboratory-based learning, while highlighting that exclusive reliance on text-based learning is associated with lower anatomy achievement. The absence of a significant association between learning preferences and theory performance suggests that multiple cognitive abilities contribute to success in anatomy, and that instructional design should address this multidimensional nature of anatomical knowledge. As medical education continues to evolve, integration of traditional cadaveric dissection with emerging technologies, blended learning approaches, and learner-centered pedagogies may be associated with improved anatomy education outcomes. Recognizing and accommodating diverse learning preferences while maintaining rigorous academic standards may enhance both immediate learning and long-term retention. However, the cross-sectional nature of this study prevents establishing causal relationships, and controlled intervention trials are needed to determine which specific pedagogical approaches optimize outcomes for students with different learning preference profiles.
Future research should employ longitudinal and experimental designs to clarify whether adapting instruction to individual learning preferences improves anatomy performance, or whether encouraging flexibility across multiple learning modalities proves more effective. Longitudinal studies tracking how learning preferences evolve from preclinical to clinical training would establish the long-term relevance of learning preference assessment, and evaluating the scalability of different instructional approaches, including traditional dissection, virtual reality, three-dimensional printed models, and augmented reality, across diverse institutional contexts would inform evidence-based resource allocation decisions. Ultimately, evidence-based anatomy education should aim to produce physicians better prepared for the anatomical demands of clinical practice.
Ethical considerations
The study was approved by the Institutional Ethics Committee of Chettinad Hospital and Research Institute (approval number: IHEC-II/0963/25). Participant confidentiality was maintained throughout the study, and all data were anonymized during analysis.
Artificial intelligence utilization for article writing
Artificial intelligence tools were used for language editing and grammar checking to improve manuscript clarity and readability. All content, data analysis, interpretations, and conclusions are the original work of the authors. No AI tools were used for data generation, analysis, or interpretation.
Acknowledgment
The authors would like to express their sincere gratitude to the first-year MBBS students of Chettinad Hospital and Research Institute, Chettinad Academy of Research and Education, Kelambakkam, Tamil Nadu, India, for their voluntary participation and cooperation in this study. The authors also acknowledge the faculty members of the Department of Anatomy and the Medical Education Unit who contributed to the content and face validity of the Learning Preference Assessment Instrument. Special thanks are extended to the institutional administration for granting permission to access academic performance records and for their support throughout the data collection process. No external funding was received for this study.
Conflict of interest statement
The authors declare no conflict of interest.
Author contributions
Conceptualization, methodology, project administration, resources, data curation, and supervision were performed by SA. Formal analysis and software management were conducted by SJ. The original draft was written by BR. Writing review and editing were contributed by SA, SJ, and BR. All authors provided final approval of the version to be published and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
This research received no external funding.
Data availability statement
The datasets used and analyzed during the current study are available from the corresponding author.
Background & Objective: Medical education requires understanding of complex anatomical structures and their functional correlations. Anatomy learning presents unique challenges, including spatial visualization, memory consolidation, and conceptual understanding. Despite competency-based curricula implementation, considerable variability persists in student anatomy performance. This study aimed to assess anatomy learning preferences among first-year MBBS students and examine their relationship with academic performance in anatomy.
Materials & Methods: A cross-sectional analytical study was conducted among 233 first-year MBBS students at the Department of Anatomy of a medical institute in Chennai, with a response rate of 93.2% (233/250). A validated 20-item questionnaire assessed four learning preference modalities: Visual-Spatial (VS), Auditory-Verbal (AV), Textual-Analytical (TA), and Tactile-Kinesthetic (TK). Academic performance was measured through formative theory and practical assessments. Statistical analyses included Spearman correlation, Kruskal-Wallis test, chi-square test, and independent t-tests.
Results: Among 233 participants, learning preference distribution was as follows: visual-spatial dominance in 30.9% (n = 72), tactile-kinesthetic in 28.3% (n = 66), auditory-verbal in 20.2% (n = 47), textual-analytical in 13.3% (n = 31), and multimodal preferences in 7.3% (n = 17). Tactile-kinesthetic preference showed a significant positive correlation with practical performance (
Conclusion: Learning preferences, particularly kinesthetic preference, significantly influence practical anatomy performance. These findings support the continued importance of hands-on dissection and laboratory-based learning, while highlighting the inadequacy of text-based learning as a sole approach. Integration of traditional cadaveric dissection with emerging technologies and blended learning approaches offers a viable pathway for anatomy education.
Introduction
Medical education demands an understanding of complex structures and functional correlations across various subjects, forming the basis of clinical practice. Anatomy, often regarded as the foundation of medical education, presents unique challenges, requiring students to integrate multiple cognitive processes simultaneously, including spatial visualization, memory consolidation, and conceptual understanding [1, 2]. Beyond morphological characteristics, learners must comprehend the spatial relationships, functional correlations, and clinical relevance of anatomical structures, all of which are fundamental to achieving the desired level of clinical competence [3]. Despite the implementation of competency-based medical education curricula across India, student performance in anatomy continues to show considerable variability [4]. This variation in academic outcomes is greatly influenced by the learning preferences of students, the preferred modalities through which they optimally receive, process, and retain anatomical information [5]. A recent cross-sectional study conducted at a teaching hospital in Perambalur, India (2023) confirmed that kinesthetic and auditory learning remain prevalent among medical students [6], with demonstrations and interactive sessions being the preferred approaches for anatomy learning. The theoretical background for analyzing learning preferences in medical education is well-established through several cognitive frameworks. According to Paivio’s Dual Coding Theory, information is processed through both verbal and visual-spatial channels, a concept directly relevant to anatomy, where students must simultaneously integrate textual descriptions with visual representations [7]. Similarly, Sweller’s Cognitive Load Theory suggests that optimal learning occurs when teaching methods are tailored to an individual’s cognitive makeup [8]. This implies that matching instructional strategies to individual learning preferences can greatly improve student performance [9]. Dobson’s seminal work demonstrated that students with visual learning preferences exhibited better performance in anatomy practical examinations, suggesting a clear connection between preferred learning style and academic outcomes [10]. The introduction of newer teaching methodologies, including digital tools, 3D modeling, flipped classrooms, and problem-based learning, results in higher knowledge retention and student engagement compared to traditional methods, with blended teaching approaches associated with greater student satisfaction [11, 12]. Despite growing interest in personalized medical education, a research gap remains in understanding how students’ anatomy learning preferences relate to their academic performance. The majority of prior studies utilize tools that lack specific design for the unique requirements of anatomy, such as three-dimensional spatial reasoning [13]. Furthermore, while some research has been conducted within the Indian medical education context, studies specifically examining the association between learning preferences and academic performance within the current curriculum remain limited [6].
The identification and understanding of anatomy learning preferences among medical students carries meaningful implications for educational practice. Such knowledge can enable anatomy educators to adopt tailored teaching methodologies that accommodate diverse learning needs, thereby improving both student engagement and academic outcomes [14]. Additionally, this understanding serves as a useful foundation for curriculum development and supports the creation of personalized learning pathways that maximize individual student potential [15].
The aim of this study was to assess anatomy learning preferences among first-year MBBS students and analyze their relationship with academic performance in anatomy. The specific objectives were: 1) to determine the distribution of anatomy learning preferences among first-year MBBS students; 2) to investigate relationships between specific learning preferences and performance in formative anatomy assessments; 3) to examine academic performance variations across different learning preference classifications; 4) to identify demographic factors influencing anatomy learning preferences; and 5) to validate the learning preference questionnaire through statistical analysis.
Materials & Methods
Design and setting(s)
This cross-sectional analytical study was conducted at the Department of Anatomy, Chettinad Hospital and Research Institute, Chennai, Tamil Nadu, India, during the period 1 December 2024 to 31 July 2025. Data collection occurred following completion of four formative assessments, through an online questionnaire administered via Google Forms.
Participants and sampling
Census sampling was employed, whereby all 250 first-year MBBS students enrolled during the study period were invited to participate. This approach was chosen to maximize sample size, ensure comprehensive representation of the study population, and minimize selection bias. Census sampling was feasible given the manageable cohort size and allowed us to capture the full spectrum of learning preferences within this academic cohort. However, 17 students did not meet the inclusion criterion of ≥ 75% attendance; therefore, the final analysis was conducted on 233 students (Figure 1).
Inclusion criteria were as follows: 1) first-year MBBS students enrolled during the study period (1 December 2024 to 31 July 2025); 2) aged 17–22 years at the time of enrollment; 3) completed a minimum of four anatomy formative assessments (both theory and practical components) during the study period; and 4) regular attendance of ≥ 75% in anatomy courses (lectures, dissection practicals, and tutorials) as per institutional regulations.
Students were excluded if they: 1) declined consent or withdrew during data collection; or 2) had attendance below 75% in anatomy courses (n = 17).
Figure 1. Flow diagram of participants through the study
Tools/Instruments
A 20-item questionnaire was developed to assess anatomy learning preferences across four modalities (Appendix 1). The instrument was constructed de novo specifically for this study; item development was informed by established theoretical frameworks, including Fleming and Mills’ VARK model [5], Felder-Soloman’s Index of Learning Styles [16], Kolb’s Experiential Learning Theory [17], and Honey and Mumford’s Learning Styles framework [18]. While these theoretical foundations guided item construction, the LPAI was not adapted from any single existing tool. All items were newly written to reflect anatomy-specific learning scenarios, for example, “I learn anatomical structures best when I can physically dissect and handle specimens” (tactile-kinesthetic preference) and “I prefer studying from anatomical atlases and color-coded diagrams” (visual-spatial preference). Face and content validity were established through expert review of item relevance, clarity, and comprehensiveness, following recommendations for obtaining content-related validity evidence via expert judgment [19, 20]. The panel comprised two anatomy faculty members, a Professor with 15 years of experience in anatomy education and an Associate Professor with 11 years of experience, along with two faculty members from the Medical Education Unit with expertise in medical education technologies. Internal consistency was evaluated using Cronbach’s alpha, which yielded a value of 0.71. The instrument assessed four learning preference modalities: Visual-Spatial Preference (VS), reflecting preference for diagrams, anatomical atlases, 3D models, and color-coded materials; Auditory-Verbal Preference (AV), reflecting preference for lectures, discussions, and verbal interaction; Textual-Analytical Preference (TA), reflecting preference for reading, note-taking, and written materials; and Tactile-Kinesthetic Preference (TK), reflecting preference for hands-on activities, dissection, and physical manipulation of specimens. Each response option was weighted equally, and total scores were calculated for each modality on a scale of 0–20. Preferences were classified as Dominant (highest score ≥ 15 with a ≥ 3-point difference from other modalities), Balanced (no modality exceeds others by ≥ 3 points), or Multimodal (two or more modalities within 2 points of each other).
Data collection methods
Data collection took place in August 2025 via an online questionnaire administered through Google Forms, following completion of four formative assessments. The Principal Investigator distributed the questionnaire link through the institutional learning management system, providing students a two-week window for completion with reminder emails sent at seven-day intervals. Confidentiality was maintained through unique identification codes linking responses to academic performance data, with password-protected storage accessible only to the Principal Investigator. Academic performance data, comprising internal assessment theory and practical scores — were obtained from official institutional records maintained by the Department of Anatomy, with appropriate administrative permissions.
Data analysis
All analyses were performed using IBM SPSS Statistics (version 29.0; IBM Corp., Armonk, NY, USA), with statistical significance set at p < 0.05 (two-tailed). Descriptive statistics, including means, standard deviations, frequencies, and percentages, were computed as appropriate.
Normality was assessed using the Kolmogorov-Smirnov and Shapiro-Wilk tests. Since learning preference scores (VS, AV, TA, TK) were not normally distributed, Spearman’s rank-order correlation coefficients were used to examine bivariate relationships between learning preference modality scores and academic performance measures. Participants were classified into dominant learning preference groups (VS, AV, TA, TK, and multimodal) based on their highest modality score. The Kruskal-Wallis H test was used to compare internal assessment theory and practical performance across these groups, with Bonferroni-corrected Dunn’s post hoc pairwise comparisons applied where significant differences were found. Pearson’s chi-square test of independence assessed associations between dominant learning preference categories and dichotomized academic performance (high ≥ 50% versus low < 50%) for both theory and practical components, as 50% represented the institutional passing threshold. As academic performance was normally distributed within unimodal subgroups (n = 216), independent samples t-tests were conducted to compare performance between theory-oriented (VS + TA dominant) versus practical-oriented (AV + TK dominant) learners, visual-dominant versus non-visual-dominant learners, and kinesthetic-dominant versus non-kinesthetic-dominant learners. Polymodal learners were excluded from these comparisons. Levene’s test was used to verify homogeneity of variance, and Cohen’s d was calculated to estimate effect sizes.
Results
Among the 233 participants, the most prevalent dominant learning preference was Visual-Spatial (VS; n = 72, 30.9%), followed by Tactile-Kinesthetic (TK; n = 66, 28.3%), Auditory-Verbal (AV; n = 47, 20.2%), Textual-Analytical (TA; n = 31, 13.3%), and Multimodal (n = 17, 7.3%). The predominance of visual and kinesthetic preferences is consistent with the hands-on, visually rich nature of anatomy education. Spearman’s rank-order correlation analysis revealed that Tactile-Kinesthetic preference was significantly and positively associated with practical assessment performance (r = 0.187, p = 0.004). Textual-Analytical preference demonstrated significant negative correlations with both theory performance (r = −0.208, p = 0.001) and practical performance (r = −0.216, p < 0.001). No other modality scores yielded statistically significant correlations with academic performance measures. Full correlation coefficients are presented in Table 1.
A 20-item questionnaire was developed to assess anatomy learning preferences across four modalities (Appendix 1). The instrument was constructed de novo specifically for this study; item development was informed by established theoretical frameworks, including Fleming and Mills’ VARK model [5], Felder-Soloman’s Index of Learning Styles [16], Kolb’s Experiential Learning Theory [17], and Honey and Mumford’s Learning Styles framework [18]. While these theoretical foundations guided item construction, the LPAI was not adapted from any single existing tool. All items were newly written to reflect anatomy-specific learning scenarios, for example, “I learn anatomical structures best when I can physically dissect and handle specimens” (tactile-kinesthetic preference) and “I prefer studying from anatomical atlases and color-coded diagrams” (visual-spatial preference). Face and content validity were established through expert review of item relevance, clarity, and comprehensiveness, following recommendations for obtaining content-related validity evidence via expert judgment [19, 20]. The panel comprised two anatomy faculty members, a Professor with 15 years of experience in anatomy education and an Associate Professor with 11 years of experience, along with two faculty members from the Medical Education Unit with expertise in medical education technologies. Internal consistency was evaluated using Cronbach’s alpha, which yielded a value of 0.71. The instrument assessed four learning preference modalities: Visual-Spatial Preference (VS), reflecting preference for diagrams, anatomical atlases, 3D models, and color-coded materials; Auditory-Verbal Preference (AV), reflecting preference for lectures, discussions, and verbal interaction; Textual-Analytical Preference (TA), reflecting preference for reading, note-taking, and written materials; and Tactile-Kinesthetic Preference (TK), reflecting preference for hands-on activities, dissection, and physical manipulation of specimens. Each response option was weighted equally, and total scores were calculated for each modality on a scale of 0–20. Preferences were classified as Dominant (highest score ≥ 15 with a ≥ 3-point difference from other modalities), Balanced (no modality exceeds others by ≥ 3 points), or Multimodal (two or more modalities within 2 points of each other).
Data collection methods
Data collection took place in August 2025 via an online questionnaire administered through Google Forms, following completion of four formative assessments. The Principal Investigator distributed the questionnaire link through the institutional learning management system, providing students a two-week window for completion with reminder emails sent at seven-day intervals. Confidentiality was maintained through unique identification codes linking responses to academic performance data, with password-protected storage accessible only to the Principal Investigator. Academic performance data, comprising internal assessment theory and practical scores — were obtained from official institutional records maintained by the Department of Anatomy, with appropriate administrative permissions.
Data analysis
All analyses were performed using IBM SPSS Statistics (version 29.0; IBM Corp., Armonk, NY, USA), with statistical significance set at p < 0.05 (two-tailed). Descriptive statistics, including means, standard deviations, frequencies, and percentages, were computed as appropriate.
Normality was assessed using the Kolmogorov-Smirnov and Shapiro-Wilk tests. Since learning preference scores (VS, AV, TA, TK) were not normally distributed, Spearman’s rank-order correlation coefficients were used to examine bivariate relationships between learning preference modality scores and academic performance measures. Participants were classified into dominant learning preference groups (VS, AV, TA, TK, and multimodal) based on their highest modality score. The Kruskal-Wallis H test was used to compare internal assessment theory and practical performance across these groups, with Bonferroni-corrected Dunn’s post hoc pairwise comparisons applied where significant differences were found. Pearson’s chi-square test of independence assessed associations between dominant learning preference categories and dichotomized academic performance (high ≥ 50% versus low < 50%) for both theory and practical components, as 50% represented the institutional passing threshold. As academic performance was normally distributed within unimodal subgroups (n = 216), independent samples t-tests were conducted to compare performance between theory-oriented (VS + TA dominant) versus practical-oriented (AV + TK dominant) learners, visual-dominant versus non-visual-dominant learners, and kinesthetic-dominant versus non-kinesthetic-dominant learners. Polymodal learners were excluded from these comparisons. Levene’s test was used to verify homogeneity of variance, and Cohen’s d was calculated to estimate effect sizes.
Results
Among the 233 participants, the most prevalent dominant learning preference was Visual-Spatial (VS; n = 72, 30.9%), followed by Tactile-Kinesthetic (TK; n = 66, 28.3%), Auditory-Verbal (AV; n = 47, 20.2%), Textual-Analytical (TA; n = 31, 13.3%), and Multimodal (n = 17, 7.3%). The predominance of visual and kinesthetic preferences is consistent with the hands-on, visually rich nature of anatomy education. Spearman’s rank-order correlation analysis revealed that Tactile-Kinesthetic preference was significantly and positively associated with practical assessment performance (r = 0.187, p = 0.004). Textual-Analytical preference demonstrated significant negative correlations with both theory performance (r = −0.208, p = 0.001) and practical performance (r = −0.216, p < 0.001). No other modality scores yielded statistically significant correlations with academic performance measures. Full correlation coefficients are presented in Table 1.
Table 1. Spearman correlation matrix between learning preferences and academic performance scores
Note: Spearman correlation coefficients are reported with p-values in parentheses.
Abbreviations: VS, visual-spatial; AV, auditory-verbal; TA, textual-analytical; TK, tactile-kinesthetic; IA, integrated assessment; Avg, average; p, probability value.
Abbreviations: VS, visual-spatial; AV, auditory-verbal; TA, textual-analytical; TK, tactile-kinesthetic; IA, integrated assessment; Avg, average; p, probability value.
Kruskal-Wallis H test revealed a statistically significant difference in practical assessment scores across dominant learning preference groups (p = 0.010), while theory scores did not differ significantly across groups. Post hoc pairwise comparisons with Bonferroni correction identified the specific group differences contributing to this finding (Table 2). Chi-square analysis indicated a significant association between dominant learning preference category and dichotomized practical performance (high vs. low; p = 0.004), whereas no significant association was observed for theory performance categories (p = 0.354; Table 3).
Table 2. Academic performance across dominant learning preference groups
Note: Values are presented as Mean ± SD. Kruskal-Wallis test was used to compare academic performance across dominant learning preference groups. Post hoc analysis revealed significant differences in practical performance between TA and AV groups (p = 0.045) and between TA and TK groups (p = 0.004).
Abbreviations: VS, visual-spatial; AV, auditory-verbal; TA, textual-analytical; TK, tactile-kinesthetic; IA, integrated assessment; Avg, average; n, number of participants; SD, standard deviation; p, probability value.
Table 3. Chi-square analysis of the association between dominant learning preference and academic performance categories
Note: Chi-square test of independence was used to examine the association between dominant learning preference and performance categories. Performance was categorized as Low (<50%) or High (≥50%) based on assessment scores.
Abbreviations: VS, visual-spatial; AV, auditory-verbal; TA, textual-analytical; TK, tactile-kinesthetic; IA, integrated assessment; n, number of participants; χ², Chi-square test; df, degrees of freedom; p, probability value.
Abbreviations: VS, visual-spatial; AV, auditory-verbal; TA, textual-analytical; TK, tactile-kinesthetic; IA, integrated assessment; n, number of participants; χ², Chi-square test; df, degrees of freedom; p, probability value.
Table 4. Comparison of academic performance between theory-oriented and practical-oriented learners
Note: Values are presented as Mean ± SD. Independent samples t-test was used for group comparisons. Polymodal learners (n = 17) were excluded from this analysis (total analyzed n = 216). Practical-oriented learners scored significantly higher in practical performance (p = 0.043); no significant difference was observed in theory performance (p = 0.558).
Abbreviations: VS, visual-spatial; AV, auditory-verbal; TA, textual-analytical; TK, tactile-kinesthetic; IA, integrated assessment; n, number of participants; SD, standard deviation; t, t-statistic; p, probability value; d, Cohen’s d effect size.
Table 5. Comparison of academic performance between visual-dominant and non-visual-dominant learners
Note: Values are presented as Mean ± SD. Independent samples t-test was used for group comparisons. Polymodal learners (n = 17) were excluded from this analysis (total analyzed N=216). No significant differences were observed in either theory (p=0.126) or practical performance (p = 0.706) between visual-dominant and non-visual-dominant learners.
Abbreviations: n, number of participants; SD, standard deviation; t, t-statistic; p, probability value; d, Cohen’s d effect size.
Table 6. Comparison of academic performance between kinesthetic-dominant and non-kinesthetic-dominant learners
Note: Values are presented as Mean ± SD. Independent samples t-test was used for group comparisons. Polymodal learners (n = 17) were excluded from this analysis (total analyzed n = 216). Kinesthetic-dominant learners scored significantly higher in practical performance (p = 0.047); no significant difference was observed in theory performance (p = 0.518).
Abbreviations: n, number of participants; SD, standard deviation; t, t-statistic; p, probability value; d, Cohen’s d effect size.
DiscussionAbbreviations: n, number of participants; SD, standard deviation; t, t-statistic; p, probability value; d, Cohen’s d effect size.
The present study found that 31% of students exhibited visual-spatial dominance, 28% demonstrated tactile-kinesthetic preference, 20% showed auditory-verbal preference, 13% preferred textual-analytical learning, and 7% demonstrated multimodal preferences. These findings align with existing literature. Satapathy and Singh reported that 70% of MBBS students demonstrated unimodal learning preferences, with kinesthetic modality being the most prevalent at 34% [21]. Rawat et al. similarly identified kinesthetic learning as the dominant preference among medical undergraduates, reinforcing the notion that anatomy education is inherently oriented toward hands-on approaches [22]. The predominance of kinesthetic and visual preferences reflects the spatially demanding and practically oriented nature of anatomy as a discipline [23]. Aboregela et al. reported that 90.5% of medical students preferred kinesthetic learning, followed by 54% auditory, 34.9% visual, and 17.5% read/write modalities [24], suggesting cross-cultural consistency in learning preference distribution among medical students globally.
The most significant finding of this study was the positive correlation between tactile-kinesthetic preference and practical examination performance (
The basis for superior kinesthetic outcomes in anatomy has been studied extensively. Chatha et al. concluded that physical examination of human tissues provides tactile and spatial understanding that digital tools cannot fully replicate, and that cadaveric dissection remains foundational for developing three-dimensional anatomical comprehension and clinical reasoning skills [27]. Elbeshbeishy et al. further confirmed that hands-on dissection facilitates professional identity formation fundamental to medical education [28].
A noteworthy finding was the negative correlation between textual-analytical preference and both theory (
However, the cross-sectional design of this study prevents establishing causality. Two interpretations are plausible: first, text-based learning may be insufficient for mastering anatomy’s spatial demands, as suggested by Martinez et al. [29]; second, students struggling with anatomy may compensate by increasing reading, making textual preference a consequence rather than a cause of poor performance. Regardless of causal direction, students with strong textual preferences warrant educational attention, either to diversify their learning approaches or to address underlying spatial reasoning difficulties. Medical educators should identify these students early and provide explicit instruction in visual-spatial and kinesthetic strategies. Longitudinal research measuring baseline preferences before anatomy instruction is needed to clarify this relationship. Contrary to initial expectations, this study found no significant performance advantage for students with multimodal learning preferences compared to those with unimodal preferences (theory:
The study revealed that 61% of students used digital resources frequently, with 49% preferring online videos as their primary digital learning tool. Nevertheless, 51% still preferred offline resources, indicating that traditional methods retain significant value and that optimal anatomy education should embrace a blended approach combining the strengths of both traditional and modern pedagogies. Recent systematic reviews support this conclusion. Nebot-Cegarra et al. conducted a comparative analysis of face-to-face and e-learning methodologies in medical anatomy education and found that blended learning approaches produced superior academic results compared to either method alone [36]. While virtual reality and augmented reality are increasingly recognized as valuable supplements to traditional dissection, Chatha et al. emphasized that these technologies should complement rather than replace cadaveric dissection, as the tactile experience remains irreplaceable for comprehensive anatomical understanding [27].
The cross-sectional design provides only a snapshot of learning preferences and performance at a single point in time, limiting the ability to assess how these relationships evolve as students progress through medical training. Longitudinal studies tracking students across multiple years would provide more robust evidence regarding the stability of learning preferences and their long-term influence on academic and clinical performance.
Academic performance was restricted to formative internal assessments and may not reflect performance in summative examinations, clinical settings, or long-term knowledge retention. Furthermore, practical assessments emphasizing specimen identification may have inherently favored kinesthetic and visual learners, potentially introducing assessment bias. The study was conducted at a single institution, and some preference groups had limited sample sizes (TA dominant:
Conclusion
This study provides evidence that learning preferences, particularly kinesthetic preference, are significantly associated with practical anatomy performance among first-year medical students. The findings support the continued importance of hands-on dissection and laboratory-based learning, while highlighting that exclusive reliance on text-based learning is associated with lower anatomy achievement. The absence of a significant association between learning preferences and theory performance suggests that multiple cognitive abilities contribute to success in anatomy, and that instructional design should address this multidimensional nature of anatomical knowledge. As medical education continues to evolve, integration of traditional cadaveric dissection with emerging technologies, blended learning approaches, and learner-centered pedagogies may be associated with improved anatomy education outcomes. Recognizing and accommodating diverse learning preferences while maintaining rigorous academic standards may enhance both immediate learning and long-term retention. However, the cross-sectional nature of this study prevents establishing causal relationships, and controlled intervention trials are needed to determine which specific pedagogical approaches optimize outcomes for students with different learning preference profiles.
Future research should employ longitudinal and experimental designs to clarify whether adapting instruction to individual learning preferences improves anatomy performance, or whether encouraging flexibility across multiple learning modalities proves more effective. Longitudinal studies tracking how learning preferences evolve from preclinical to clinical training would establish the long-term relevance of learning preference assessment, and evaluating the scalability of different instructional approaches, including traditional dissection, virtual reality, three-dimensional printed models, and augmented reality, across diverse institutional contexts would inform evidence-based resource allocation decisions. Ultimately, evidence-based anatomy education should aim to produce physicians better prepared for the anatomical demands of clinical practice.
Ethical considerations
The study was approved by the Institutional Ethics Committee of Chettinad Hospital and Research Institute (approval number: IHEC-II/0963/25). Participant confidentiality was maintained throughout the study, and all data were anonymized during analysis.
Artificial intelligence utilization for article writing
Artificial intelligence tools were used for language editing and grammar checking to improve manuscript clarity and readability. All content, data analysis, interpretations, and conclusions are the original work of the authors. No AI tools were used for data generation, analysis, or interpretation.
Acknowledgment
The authors would like to express their sincere gratitude to the first-year MBBS students of Chettinad Hospital and Research Institute, Chettinad Academy of Research and Education, Kelambakkam, Tamil Nadu, India, for their voluntary participation and cooperation in this study. The authors also acknowledge the faculty members of the Department of Anatomy and the Medical Education Unit who contributed to the content and face validity of the Learning Preference Assessment Instrument. Special thanks are extended to the institutional administration for granting permission to access academic performance records and for their support throughout the data collection process. No external funding was received for this study.
Conflict of interest statement
The authors declare no conflict of interest.
Author contributions
Conceptualization, methodology, project administration, resources, data curation, and supervision were performed by SA. Formal analysis and software management were conducted by SJ. The original draft was written by BR. Writing review and editing were contributed by SA, SJ, and BR. All authors provided final approval of the version to be published and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
This research received no external funding.
Data availability statement
The datasets used and analyzed during the current study are available from the corresponding author.
Article Type : Orginal Research |
Subject:
Medical Education
Received: 2025/11/26 | Accepted: 2026/02/22 | Published: 2026/04/1
Received: 2025/11/26 | Accepted: 2026/02/22 | Published: 2026/04/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
