
Sat, Jul 11, 2026
[Archive]
Volume 19, Issue 1 (2026)
J Med Edu Dev 2026, 19(1): 20-33 |
Back to browse issues page
Ethics code: CRS/ERC/2023/008
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Enang E O, Agiounim Imam S, Madu E O, Lawson O E, Etuk B, Adah T A. Unspoken power dynamics and the hidden curriculum in allied medical education: a qualitative study of lecturer–student relationships at the University of Calabar. J Med Edu Dev 2026; 19 (1) :20-33
URL: http://edujournal.zums.ac.ir/article-1-2623-en.html
URL: http://edujournal.zums.ac.ir/article-1-2623-en.html
Emmanuel Okon Enang *1  , Sandra Agiounim Imam2 , Ezra Onyedikachi Madu3 , Ofonime Esangubong Lawson2 , Blessing Etuk4 , Tommy Adah Adah5
, Sandra Agiounim Imam2 , Ezra Onyedikachi Madu3 , Ofonime Esangubong Lawson2 , Blessing Etuk4 , Tommy Adah Adah5
, Sandra Agiounim Imam2 , Ezra Onyedikachi Madu3 , Ofonime Esangubong Lawson2 , Blessing Etuk4 , Tommy Adah Adah5
1- Department of Physiotherapy, University of Calabar, Calabar, Cross River State, Nigeria , enangemmanuel24@gmail.com
2- Department of Nursing Science, University of Calabar, Calabar, Cross River State, Nigeria
3- Department of Nursing Sciences, State University of Medical and Applied Sciences, Enugu State, Nigeria
4- Department of Human Nutrition and Dietetics, University of Calabar, Calabar, Cross River State, Nigeria
5- Department of Radiography, University of Calabar, Calabar, Cross River State, Nigeria
2- Department of Nursing Science, University of Calabar, Calabar, Cross River State, Nigeria
3- Department of Nursing Sciences, State University of Medical and Applied Sciences, Enugu State, Nigeria
4- Department of Human Nutrition and Dietetics, University of Calabar, Calabar, Cross River State, Nigeria
5- Department of Radiography, University of Calabar, Calabar, Cross River State, Nigeria
Keywords: hidden curriculum, power dynamics, faculty–student relations, education, professional, allied health personnel, qualitative research
Full-Text [PDF 607 kb]
(180 Downloads)
| Abstract (HTML) (472 Views)
Full-Text: (212 Views)
Abstract
Background & Objective: The influence of lecturer–student relationships extends beyond formal teaching and reflects a hidden curriculum that often shapes students’ attitudes, confidence, and professional growth. In Nigerian allied medical education, these subtle power dynamics remain largely unexamined. This study explored how allied medical students at the University of Calabar experience and interpret lecturer–student power relations in their learning environment.
Materials & Methods: A phenomenological qualitative design, guided by Husserl’s framework, was employed to capture students’ subjective experiences. Forty participants were purposively selected from four departments: Physiotherapy, Nursing Science, Radiography, and Human Nutrition & Dietetics. Data were generated through ten semi-structured focus group discussions (4 participants each), lasting 45–60 minutes. All sessions were audio-recorded, transcribed verbatim, and analyzed using Colaizzi’s seven-step phenomenological method to identify the essence of shared experiences. Data saturation was monitored throughout collection, while credibility was enhanced via triangulation, reflexive journaling, peer debriefing, and member checking.
Results: Four interrelated themes emerged: lecturer misconduct, power and submission, coping mechanisms, and emotional consequences. Students described experiences of intimidation, public reprimand, and exclusion that generated fear and self-doubt. Coping responses included emotional withdrawal, peer support, and silent endurance. These experiences revealed how the hidden curriculum communicates implicit lessons about authority, conformity, and professionalism, often constraining critical engagement and emotional well-being.
Conclusion: Power asymmetry within the classroom profoundly shapes allied health students’ learning experiences and professional development. Creating supportive academic environments that foster mutual respect, mentorship, and ethical teaching practices is essential to mitigating fear-based learning and promoting healthy lecturer–student relationships.
Introduction
Medical education seeks to cultivate more than the technical mastery of anatomy, physiology, and clinical reasoning; it aspires to shape humane, reflective, and ethically grounded professionals who deliver patient-centered care [1]. Yet, beyond structured syllabi and formal assessments, a subtle and pervasive hidden curriculum exists, comprising unspoken expectations, institutional hierarchies, interpersonal power relations, and behavioral modeling that collectively influence students’ moral development, professional identity, and sense of belonging [2, 3].
Theme 1: Lecturer misconduct
Students consistently described recurring experiences of humiliation, arbitrary punishment, and intimidation from lecturers. The misconduct was not occasional; it was normalized and pervasive, shaping emotional wellbeing and academic performance.
Subtheme 1.1: Public humiliation — “They shame you just to show they have power”
Participants described emotional trauma, social exposure, and internalized self-doubt resulting from humiliation: FGD 1
P1: “I walked in confident that day, fully prepared, thinking my answers were solid. Suddenly, the lecturer stopped me, pointing at me in front of everyone, saying, ‘How did you even get here? You are a disgrace.’ My heart sank; I froze. Whispers surrounded me, and I felt
trapped. I wanted to defend myself but couldn’t. For days, I replayed that moment, questioning my intelligence, my worth, my very place in this program. The shame wasn’t just emotional; it lingered physically, making me anxious even when reviewing for unrelated classes.”
P11: “It wasn’t only the words; it was the way he looked, the pause, the deliberate tone.
Every gesture screamed authority and intent to diminish me. Even when peers tried to console me, I felt invisible, broken, and doubted whether I belonged at all.”
P21: “Sometimes the humiliation was subtle: a joke about how I spoke or my accent. Small, passing comments, but they left long shadows. I doubted every answer I gave afterward, overthinking every word, fearing ridicule.”
P31: “Before each class, I would feel my stomach churn, hands tremble. At times I considered skipping just to avoid humiliation. Yet, absence would bring its own punishment. I lived in constant anticipation of shame, trying to survive rather than learn.”
FGD 2
P2: “During clinical posting, a lecturer openly compared me to someone incompetent in front of a patient. I froze, my face burning, my mind racing with humiliation and disbelief. I wanted to explain, but fear rooted me in silence. That day, the shame followed me back to the hostel, affecting my ability to sleep and study.”
P12: “One day, my notebook was ridiculed, my handwriting described as childish, unworthy. My peers’ laughter intensified the pain.
I hid my face, suppressing tears. I wanted to leave the program; the humiliation made me question my place entirely.”
P22: “The intersection of lecturer ridicule and peer observation magnified humiliation.
I felt doubly exposed, first by authority, then by those around me.”
P32: “I began journaling every insult, every incident. Writing helped process feelings, but reading back, I still felt the emotional sting, realizing humiliation leaves deep, lingering marks on self-confidence.”
Interpretive Meaning: Public humiliation served as a psychological weapon, reinforcing hierarchical dominance and undermining self-worth. Students internalized shame, impacting emotional wellbeing and learning motivation.
Subtheme 1.2: Arbitrary dismissal — “You can be sent out for almost anything”
Students reported dismissal from lectures or clinical sessions without reason, generating helplessness and academic disruption: FGD 3
P3: “I was sent out for a trivial reason, standing behind a lecturer while helping a colleague. He shouted at me to leave.
My heart raced. I lost the entire lecture, and the next quiz covered exactly that content. I felt punished for being helpful, humiliated, and powerless.”
P13: “Even minor attire mistakes, shoes not shiny, notebook unorganized, could trigger dismissal. We would stand outside for hours, under the sun, questioning why authority had become cruelty.”
P23: “I was once sent out for greeting a lecturer ‘too casually.’ The public correction, the scolding, and forced removal taught me that survival meant compliance, not learning. Later, friends marked attendance for me because I feared reprisals.”
P33: “Dismissal without explanation became a shared narrative among students. We used collective language, ‘we get sent out’ revealing normalization of arbitrary punishment and internalized helplessness.”
Interpretive meaning: Arbitrary dismissal demonstrated institutionalized power misuse. Students learned fearful compliance, sacrificing active participation and engagement.
Subtheme 1.3: Intimidation and threats — “You either obey or you fail”
Lecturers used threats, control over grading, and psychological coercion to enforce submission:
FGD 4
P4: “A lecturer openly said, ‘If I don’t like your attitude, I can fail you even if you score 90.’ Everyone knew he meant it. After that, questions were silenced. We stopped trying to clarify or correct mistakes.”
P14: “Indirect threats, comments like ‘I can make your life difficult here’ instilled anxiety. One classmate challenged a lecturer politely; later, assessment sheets showed false remarks. Fear dictated behavior, more than respect.”
P24: “We realized that even HODs suggested endurance over confrontation. The unwritten rule, obey or fail, created pervasive silence and submission.”
P34: “Threats extended beyond the classroom. Even when lecturers smiled or joked, we felt monitored, manipulated by fear. Our learning became secondary to survival.”
Interpretive meaning: Intimidation enforced silent obedience, suppressing critical thinking and eroding professional agency.
Theme 2: Power, fear, and submission
Overview: Students described a hierarchy-driven learning environment where fear dictated behavior, and submission became a survival strategy.
Subtheme 2.1: Hierarchy and power distance — “You don’t talk, you just nod”
FGD 5
P5: “Even knowing an answer, I kept quiet. Correcting a lecturer could result in being labelled rude, affecting grades. Silence became my shield.”
P15: “A classmate’s polite correction led to public rebuke. Since then, she never spoke in class. Authority was absolute, leaving no room for questioning.”
P25: “Walking into class felt like stepping onto a battlefield. You anticipate judgment in every gesture, tone, or response.”
P35: “The psychological impact was cumulative. Over time, we learned that survival demanded subordination over curiosity.”
Interpretive meaning: Students internalized the hierarchy, creating self-imposed silence, reinforcing structural dominance.
Subtheme 2.2: Culture of fear — “You don’t want to be noticed for the wrong reasons”
FGD 6
P6: “We moved like shadows. Being noticed could trigger punishment. Fear dictated interaction, attention, even study habits.”
P16: “Reporting misconduct was too risky. Those who tried were ostracized, branded troublemakers.”
P26: “Even routine greetings or eye contact carried potential peril. Anxiety became constant, shaping our daily academic experience.”
P36: “Fear was invisible but omnipresent. It dictated our behavior more than any rules.”
Interpretive Meaning: Fear acted as an invisible pedagogy, controlling behavior and suppressing voice.
Subtheme 2.3: Learned submission — “Survival means pretending everything is fine”
FGD 7
P7: “Pretending to be fine became a habit. Even when angry, we smiled, answered yes, nodded, concealed emotions.”
P17: “By final year, obedience felt natural. Resistance was emotionally costly.”
P27: “Classmates observed our adaptation and emulated it. Submission was socially reinforced.”
P37: “Survival required internalizing fear as professionalism.”
Interpretive meaning: Students adopted learned submission, embedding fear and obedience into their professional identity.
Theme 3: Resistance and coping mechanisms
Despite pervasive fear, humiliation, and intimidation, students actively developed strategies to survive, resist, and maintain some form of personal agency. Their resistance was complex, subtle, and multidimensional, encompassing emotional detachment, social support, silent rebellion, academic perseverance, and spiritual reliance.
Subtheme 3.1: Emotional detachment — “You stop expecting fairness, you just protect yourself”
Students described emotional shielding as a key coping mechanism, creating a psychological buffer against persistent lecturer misconduct:
P8: “I had to stop expecting fairness. Every time I raised my hand or answered confidently, it seemed like an invitation for ridicule. I trained myself to stay neutral, to nod and smile, pretending I wasn’t hurt. Inside, I felt the sting, but I had to survive.”
P18: “Detachment became a shield. I no longer took insults personally; they were part of the system. This saved my mental energy but slowly made learning mechanical, devoid of enthusiasm.”
P28: “I even started separating my grades from my emotions. If a lecturer scolded me for participation, I reminded myself it was about power, not ability. That realization helped me focus on content, not authority.”
P38: “Sometimes, detachment felt like numbness. I knew it was self-preservation, but it also made me disconnected from peers and even my own motivation.”
Interpretive meaning: Emotional detachment functioned as psychological survival, allowing students to maintain presence and engagement while insulating themselves from emotional damage.
Subtheme 3.2: Peer support and collective coping — “We heal each other”
Social support emerged as a critical coping mechanism. Students described informal networks where experiences were shared, validated, and collectively navigated:
FGD 9
P9: “After each class, we huddled together and debriefed. Sharing what happened validated our feelings. It felt like saying, ‘I am not crazy; this really happened.’”
P19: “Humor helped. We gave nicknames to lecturers, joked about ridiculous punishments, and laughed at shared misery. The laughter was both relief and quiet rebellion.”
P29: “We also shared strategies—how to respond without escalating, how to anticipate mood shifts, how to survive exams without attracting attention. This network became a safety net.”
P39: “Even simple gestures—like a nod or smile in solidarity—made us feel seen. We learned to lean on each other when authority felt overwhelming.”
Interpretive meaning: Peer support created resilient micro-communities, mitigating isolation and enabling adaptive strategies in a threatening academic environment.
Subtheme 3.3: Silent resistance — “We smile, but inside we know”
Students engaged in covert, symbolic acts of resistance, maintaining dignity and psychological autonomy
without confronting authority openly: FGD 10
P10: “I stopped showing immediate reactions. When insulted, I smiled politely. The smile masked defiance—inside, I refused to internalize the shame.”
P20: “We coded our resistance in humor, nicknames, and private discussions. Calling a lecturer a ‘dictator’ in our group chat was a way to reclaim power safely.”
P30: “Some of us focused on excelling academically, knowing that true competence would eventually speak louder than intimidation. It felt like silent protest—surviving and thriving without giving them control.”
P40: “Even when submitting assignments, we carefully followed rules but added subtle critiques in presentations. Small acts, but they felt like moral victory.”
Interpretive meaning: Silent resistance allowed students to assert psychological autonomy, retain self-respect, and maintain hope within a rigid, authoritarian environment.
Subtheme 3.4: Spiritual resilience — “Only god can see what we go through”
Faith and spirituality were central in coping with persistent fear, humiliation, and academic stress:
FGD 1
P1: “Prayer gave me calm. I told myself, ‘I may not be able to change him, but I can hold my integrity and trust God.’”
P11: “I visualized my efforts being rewarded in the long run. Believing in divine justice made enduring humiliation possible.”
P21: “Meditation and reflection became tools to process anger and maintain hope. Spirituality was the anchor in turbulent classrooms.”
P31: “Even when everything seemed unfair, faith reminded me that my knowledge and perseverance mattered beyond immediate approval.”
Interpretive meaning: Spiritual resilience provided internal moral and emotional support, allowing students to navigate systemic injustice without losing personal integrity.
Theme 4: Emotional and academic consequences
The combination of fear, humiliation, and hierarchical dominance led to multi-layered consequences, affecting mental health, emotional wellbeing, motivation, and academic engagement.
Students’ narratives reflected profound psychological burden and learning disruption, extending beyond the classroom.
Subtheme 4.1: Academic anxiety and loss of confidence — “Even prepared, I freeze”
Students reported anticipatory anxiety, self-doubt, and fear-induced performance decline:
FGD 7
P7: “I knew the answers, I studied hard, but standing in front of the class, my mind went blank. Fear made me forget everything.”
P17: “After repeated humiliation, I began doubting myself. Every wrong look from a lecturer felt like confirmation I wasn’t good enough.”
P27: “Even simple tasks like reading aloud or presenting slides triggered tremors, sweating, and nausea. Anxiety became a constant companion.”
P37: “This anxiety wasn’t limited to one class. It followed me to other courses. I questioned my intelligence, my capability, my very purpose as a student.”
Interpretive Meaning: Persistent fear undermined self-efficacy, creating a cycle of academic anxiety and reduced performance.
Subtheme 4.2: Examination experiences — “Tests became survival, not assessment”
Fear of bias, unpredictable grading, and authority-driven assessment dominated experiences:
FGD 8
P8: “Exams felt like traps. I wasn’t tested on knowledge alone; I was tested on my ability to navigate favor and fear.”
P18: “I second-guessed answers, worried if a lecturer disliked me, would they mark me unfairly? It was draining.”
P28: “Some of us scored poorly not due to lack of preparation but due to emotional paralysis. The classroom became a battlefield, and exams were ambushes.”
P38: “Even assignments were intimidating. A simple mistake could be exaggerated to shame or threaten us academically.”
Interpretive Meaning: Academic assessment was psychologically contaminated, turning evaluation into a source of stress rather than learning feedback.
Subtheme 4.3: Emotional distress and mental exhaustion — “Every day feels heavy”
Students narrated burnout, depressive symptoms, and emotional fatigue:
FGD 9
P9: “By the end of each semester, I felt mentally drained. I lost appetite for learning, even topics I loved.”
P19: “Sleep was erratic. I replayed humiliating incidents in my head, sometimes crying alone at night.”
P29: “Friendships helped, but the emotional burden was constant. The mental energy it took to survive each class was exhausting.”
P39: “Some classmates developed physical symptoms: headaches, stomachaches. Stress wasn’t just in our minds; it manifested in our bodies.”
Interpretive meaning: Continuous mistreatment led to psychosomatic manifestations and emotional depletion, impacting overall wellbeing.
Subtheme 4.4: Academic disengagement and loss of motivation — “I learn to survive, not to excel”
Long-term consequence: reduced engagement and internalized minimalism:
FGD 10
P10: “Eventually, I stopped asking questions. Learning was secondary to surviving humiliation.”
P20: “Motivation shifted from curiosity to mere completion. Excellence felt risky; discretion felt safer.”
P30: “Even group work became stressful. I avoided leadership roles to minimize exposure.”
P40: “Some of us considered leaving the program. The environment crushed enthusiasm, leaving only mechanical effort.”
Interpretive Meaning: The oppressive environment
created academic disengagement, transforming the educational journey from active learning to survival-based compliance.
Fundamental structure
Students’ lived experiences reveal an educational ecosystem dominated by fear, humiliation, and hierarchical authority. While some survive through detachment, peer solidarity, silent resistance, and spiritual resilience, the cumulative effect erodes confidence, engagement, and mental health. Academic participation is constrained by survival imperatives, and learning becomes subordinated to self-preservation.
Validation of findings
To ensure authenticity and rigor, findings were validated through participant confirmation, where representatives from each FGD reviewed the themes and subthemes to confirm that the interpretations faithfully represented their experiences. Reflexive journaling, peer debriefing, and triangulation across the 10 FGDs ensured interpretive credibility, reducing researcher bias and confirming that the results captured the true essence of student experiences in the academic environment
Discussion
The findings indicate that students’ experiences reflect not only individual misunderstandings but also a broader structural culture of domination within academic spaces. Participants described classroom and clinical interactions frequently characterized by humiliation, dismissal, and threats. Students recounted instances of being openly insulted, yelled at, or embarrassed in front of peers for minor academic errors or for simply asking questions. One participant stated, “During a practical, the lecturer said, “You people are the worst set this department has ever produced.’ I felt so small; I could not speak again.” These recurring experiences highlight how power is exercised and reinforced through verbal aggression and public shaming.
Such patterns are consistent with the concept of the hidden curriculum [50], in which professional norms and expectations are communicated implicitly, often through unspoken power dynamics, rather than through formal instruction. Participants further emphasized the emotional weight of these encounters, reporting anxiety, emotional withdrawal, and diminished engagement in learning. Participant 3, FGD 4, reflected, “After that day, he shouted at me, I stopped answering questions even when I knew the answers. It’s safer to just keep quiet.” These avoidance responses align with findings that fear-based learning environments trigger psychological withdrawal and reduce active participation [50]. Emotional intimidation, though often framed as disciplinary, functions as a pedagogical mechanism that discourages independent thought and fosters dependency on authority, supporting the principles of Self-Determination Theory, which posit that undermining autonomy and relatedness leads to loss of intrinsic motivation and disengagement [51].
Academic assessments emerged as another domain where power was exerted and emotional control maintained. Participants reported instances of perceived bias, favoritism, and punitive grading, despite diligent preparation. One student explained, “You study so hard, yet your results are poor.
When you go to ask why, they walk you out or say you should be grateful you even passed.” These experiences suggest that assessment practices, rather than reflecting competence, were leveraged to reinforce hierarchy and obedience, consistent with previous findings on coercive educational structures [52]. When feedback is withheld or used as a tool of humiliation, assessment transforms into an instrument of oppression [53]. Repeated exposure to such treatment contributed to emotional exhaustion, with participants reporting insomnia, low self-esteem, and a sense of helplessness.
A radiography student commented, “I used to love this course, but now I just count down to graduation. Every class feels like a battle for survival.” This statement exemplifies academic burnout [50] and reflects how toxic hierarchies can suppress professional identity and ethical engagement [54]. Participants described silence as both protective and corrosive, shielding them from immediate confrontation but gradually eroding confidence, autonomy, and moral sensitivity, a process akin to moral erosion [55]. The analysis further reveals that these relational dynamics directly impacted academic performance. Students reported diminished concentration and confidence during examinations and clinical evaluations following public ridicule or perceived favoritism.
One student stated, “You go into exams already defeated because you know your script will be judged by who likes you, not what you wrote.” Attempts to seek clarification often resulted in further humiliation, exemplified by the statement, “When I approached the lecturer to ask why I failed, he laughed and said, ‘If you can’t handle failure, you don’t belong here.’” These experiences reflect emotional neglect and institutional indifference, undermining both the integrity of the assessment process and trust in the educational system [56]. Collectively, these findings suggest that the interactions observed constitute a form of structural violence within the academic environment. Structural violence arises when social institutions produce harm by restricting individuals’ potential for growth and dignity [7]. In this study, the normalization of intimidation, absence of accountability, and lack of transparent communication perpetuate harm through emotional and moral degradation rather than physical force. The convergence of participant experiences across departments indicates systemic dysfunction rather than isolated incidents, emphasizing the pervasiveness of these power dynamics [57].
The findings underscore the urgent need for transformative educational reform. Hidden curricula rooted in fear, humiliation, and silence risk producing future health professionals who replicate similar oppressive behaviors in clinical practice. Participants highlighted the necessity of learning environments grounded in empathy, dialogue, and respect. Institutional leaders should establish transparent feedback mechanisms, enforce clear misconduct policies, and implement pedagogical training emphasizing emotional intelligence and ethical accountability. Only by addressing these structural and relational factors can allied medical education in Nigeria cultivate competent, compassionate, and socially responsible professionals. This study has several limitations. Its qualitative design and focus on a single Nigerian university limit the generalizability of the findings. Data relied on student self-reports within FGDs, a method which, while invaluable for capturing shared social experiences, may have limited the disclosure of highly personal views. Furthermore, the perspectives of lecturers were not included. Despite these limitations, the study provides in-depth, contextual insights into a critical aspect of allied medical education.
Conclusion
This study concludes that lecturer–student dynamics within allied medical education at the University of Calabar are structurally shaped by hierarchical power relations that manifest as emotional domination, academic intimidation, and institutionalized silence. The findings establish that public humiliation, punitive grading, and communication breakdowns are not isolated incidents but systematic practices embedded within the hidden curriculum that reproduce fear-based learning and moral desensitization. The study, therefore, concludes that these entrenched patterns undermine the core objectives of professional education by eroding psychological safety, intrinsic motivation, and ethical development among students.
This evidence underscores an urgent need for institutional transformation, anchored on pedagogical transparency, feedback justice, and relational ethics, to restore balance, autonomy, and trust within the educational process.
In essence, the study provides empirical confirmation that unless hierarchical abuse is confronted as an academic pathology, allied medical education risks perpetuating a generation of technically competent but ethically impaired healthcare professionals.
Ethical considerations
Ethical approval was obtained from the Cross River State Ethics Review Committee (Reference No: CRS/ERC/2024/008). Participation was voluntary, and informed consent was obtained before FGDs. Confidentiality and anonymity were strictly maintained throughout data collection, transcription, and analysis. Additional safeguards included offering breaks or referrals to professional counselling to participants who showed distress.
Measures to minimize coercion included conducting off-campus FGDs, using neutral language, and emphasizing voluntary participation before, during, and after sessions.
Artificial intelligence utilization for article writing
No artificial intelligence tools were used in the design, data collection, analysis, or writing of this manuscript. The authors confirm that all interpretations, analyses, and written content are solely the result of human scholarly effort.
Acknowledgment
The authors express profound gratitude to the allied medical students from the Departments of Physiotherapy, Nursing Science, Radiography, and Nutrition & Dietetics at the University of Calabar who generously shared their lived experiences.
Appreciation is also extended to faculty mentors who provided valuable feedback during data validation and to the Department of Physiotherapy for institutional and logistical support throughout the research process.
Conflict of interest statement
The authors declare no conflict of interest.
Author contributions
The author contributions are as follows: EOE was responsible for conceptualization, methodology, qualitative study design, data collection, formal analysis, interpretation of findings, writing the original draft, reviewing and editing, and project administration. SAI contributed to methodology, data collection, qualitative coding support, and review and editing. EOM handled data collection, supervision, validation of themes, and review and editing.
EOL performed data analysis, thematic interpretation, and review and editing. BE assisted with data collection, transcription, and critical revision of the manuscript for intellectual content. TAA provided methodological oversight and data curation.
Funding
This research received no external funding. All expenses were personally covered by the authors.
Data availability statement
The data supporting the findings of this study are not publicly available due to confidentiality agreements with participants, but may be accessed from the corresponding author upon reasonable request and with appropriate ethical clearance.
Background & Objective: The influence of lecturer–student relationships extends beyond formal teaching and reflects a hidden curriculum that often shapes students’ attitudes, confidence, and professional growth. In Nigerian allied medical education, these subtle power dynamics remain largely unexamined. This study explored how allied medical students at the University of Calabar experience and interpret lecturer–student power relations in their learning environment.
Materials & Methods: A phenomenological qualitative design, guided by Husserl’s framework, was employed to capture students’ subjective experiences. Forty participants were purposively selected from four departments: Physiotherapy, Nursing Science, Radiography, and Human Nutrition & Dietetics. Data were generated through ten semi-structured focus group discussions (4 participants each), lasting 45–60 minutes. All sessions were audio-recorded, transcribed verbatim, and analyzed using Colaizzi’s seven-step phenomenological method to identify the essence of shared experiences. Data saturation was monitored throughout collection, while credibility was enhanced via triangulation, reflexive journaling, peer debriefing, and member checking.
Results: Four interrelated themes emerged: lecturer misconduct, power and submission, coping mechanisms, and emotional consequences. Students described experiences of intimidation, public reprimand, and exclusion that generated fear and self-doubt. Coping responses included emotional withdrawal, peer support, and silent endurance. These experiences revealed how the hidden curriculum communicates implicit lessons about authority, conformity, and professionalism, often constraining critical engagement and emotional well-being.
Conclusion: Power asymmetry within the classroom profoundly shapes allied health students’ learning experiences and professional development. Creating supportive academic environments that foster mutual respect, mentorship, and ethical teaching practices is essential to mitigating fear-based learning and promoting healthy lecturer–student relationships.
Introduction
While the formal curriculum teaches what physicians ought to do, the hidden curriculum often teaches what they actually become [4]. Globally, evidence shows that these unarticulated lessons powerfully shape attitudes toward authority, empathy, and patient care, sometimes undermining the explicit values of compassion and professionalism embedded in medical education [1, 3, 4]. In Nigeria, the hidden curriculum operates within a context marked by steep hierarchies, limited institutional accountability, and sociocultural norms that privilege deference to authority.
These conditions magnify the impact of faculty–student power dynamics, making them a central yet underexplored determinant of professional socialization. Studies across Nigerian medical schools consistently reveal that mistreatment and intimidation are systemic rather than exceptional.
Owoaje et al. [8] found that nearly 59% of students at the University of Ibadan reported experiencing verbal abuse or public humiliation, while 63% of respondents at the University of Lagos reported experiencing neglect or dismissive treatment from lecturers [9].
At the University of Nigeria, Nsukka, 49% of students reported witnessing peers being publicly punished or reprimanded without justification [10]. A recent meta-review synthesizing data from six medical schools reported an overall prevalence of mistreatment ranging from 46% to 91% [3, 6, 11].
The implications extend far beyond classroom discomfort. Empirical studies associate exposure to mistreatment with heightened anxiety, depression, burnout, and moral distress [12–14].
For example, Ayinde et al. [12] observed that Nigerian students repeatedly subjected to public shaming displayed diminished motivation, withdrawal from academic engagement, and impaired self-confidence. Sustained exposure to hierarchical humiliation can
corrode empathy and distort emerging professional identities [13, 14]. Academically, mistreated students exhibit lower participation in clinical discussions, avoidance of supervisors, and reduced academic performance [15]. These psychosocial and behavioral sequelae underscore that the hidden curriculum is not merely an educational phenomenon but also a public health concern. When internalized, these negative patterns risk perpetuating cycles of disrespect in clinical practice, eroding trust between future doctors and patients, and potentially compromising patient safety [19,20]. Bandura’s social learning theory explains that students emulate behaviors modeled by authority figures, thereby normalizing hierarchical or abusive conduct [16]. Foucault’s concept of disciplinary power reveals how medical institutions subtly regulate behavior through surveillance and authority, while Bourdieu’s notion of habitus demonstrates how repeated exposure to domination shapes enduring professional dispositions [17, 18, 19].
This study draws primarily on Foucault’s theory to interpret hierarchical practices and on Bourdieu’s framework to understand how students internalize these dynamics. Consequently, critical questions remain unanswered: How do Nigerian medical students make sense of institutionalized authority? What coping mechanisms allow them to survive emotionally taxing learning environments? And how do these experiences shape their emerging professional identities? Therefore, this study explores how the hidden curriculum manifests through lecturer–student power relations and experiences of mistreatment among medical students at the University of Calabar.
By employing a phenomenological design, the research seeks to uncover the depth and complexity of students’ lived experiences, emotional interpretations, and coping mechanisms, dimensions that quantitative data alone cannot reveal.
Materials & Methods
Design and setting(s)
This study adopted a phenomenological qualitative design to explore the lived experiences of medical students regarding hidden curricula and lecturer–student power dynamics at the University of Calabar (UNICAL) [20,21]. The central research question guiding this design was: How do medical students at UNICAL experience and interpret hidden curricula and lecturer–student power relations in their training environment? Phenomenology was chosen because it captures the essence of participants’ lived experiences, emphasizing subjective perceptions, emotions, and meanings that shape academic engagement and professional identity. A Husserlian framework guided the inquiry, emphasizing descriptive experiences and the process of bracketing researcher preconceptions to ensure participants’ voices remained central [24,25]. This approach was preferred over Heideggerian phenomenology, which emphasizes interpretation, as the study sought to describe experiences of power dynamics without researcher-imposed meaning.
The study was conducted within the Faculty of Allied Medical Sciences, University of Calabar, which comprises the Departments of Nursing Science, Physiotherapy, Radiography, and Human Nutrition & Dietetics. This faculty represents diverse health-related programs with hierarchical teaching structures, frequent lecturer–student interactions, and combined theoretical and clinical exposures [26,27].
The setting mirrors the broader sociocultural context of Nigerian medical schools, where power hierarchies, professional expectations, and resource constraints shape both the formal and hidden curricula [28,29]. Previous studies in similar contexts show that over 60% of medical students report verbal abuse or humiliation from lecturers, underscoring the national relevance of this issue [30–32].
Data collection was conducted over a three-month period, from 10 March 2024 to 28 May 2024, encompassing all phases of participant recruitment, scheduling, and completion of the Focus Group Discussions (FGDs).”
Participants and sampling
A total of 40 students were purposively selected, comprising 10 participants from each department, consistent with phenomenological principles emphasizing information richness over numerical breadth [34, 35]. Inclusion criteria were: (1) current enrollment in 300-level or above, (2) completion of at least one clinical posting, and (3) willingness to share experiences freely. Students on academic suspension or those below 300 level were excluded.
Participants were recruited through departmental notice boards and class WhatsApp groups, allowing voluntary, private contact with the researcher.
To reduce coercion, recruitment, and FGDs were conducted off-campus, and no lecturer participated in the recruitment process. This ensured participants’ autonomy and confidentiality in expressing sensitive opinions about lecturers. Sample adequacy was determined through data saturation, the point at which no new themes or insights emerged [36, 37].
Monitoring occurred concurrently with data collection and preliminary analysis, typically reached between the 8th and 10th FGDs [38, 39].
The researcher’s insider position was acknowledged as both a strength and a potential source of bias. Reflexivity strategies included reflective journaling after each FGD to document assumptions, emotional responses, and interpretive decisions, and weekly peer debriefing with qualitative experts to challenge subjectivity [40, 41]. An audit trail documented all methodological decisions, ensuring transparency and dependability.
Tools/Instruments
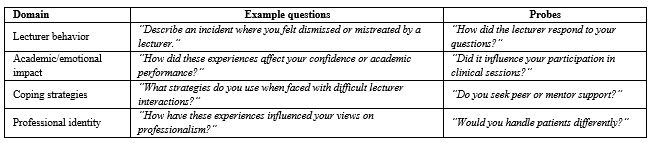
Data were collected using a semi-structured FGD guide developed from literature on hidden curricula, professional socialization, and power dynamics [42, 43]. The guide was informed by Hafferty’s Hidden Curriculum Theory and Bourdieu’s Theory of Power and Habitus, providing theoretical grounding for exploring hierarchical interactions in medical education. The instrument was reviewed by three qualitative research experts for content validity and pilot-tested with two students outside the study sample, leading to refinement of emotionally charged questions to encourage openness (Table 1).
Table 1. Domains and example questions from the semi-structured focus group discussion guideThese conditions magnify the impact of faculty–student power dynamics, making them a central yet underexplored determinant of professional socialization. Studies across Nigerian medical schools consistently reveal that mistreatment and intimidation are systemic rather than exceptional.
Owoaje et al. [8] found that nearly 59% of students at the University of Ibadan reported experiencing verbal abuse or public humiliation, while 63% of respondents at the University of Lagos reported experiencing neglect or dismissive treatment from lecturers [9].
At the University of Nigeria, Nsukka, 49% of students reported witnessing peers being publicly punished or reprimanded without justification [10]. A recent meta-review synthesizing data from six medical schools reported an overall prevalence of mistreatment ranging from 46% to 91% [3, 6, 11].
The implications extend far beyond classroom discomfort. Empirical studies associate exposure to mistreatment with heightened anxiety, depression, burnout, and moral distress [12–14].
For example, Ayinde et al. [12] observed that Nigerian students repeatedly subjected to public shaming displayed diminished motivation, withdrawal from academic engagement, and impaired self-confidence. Sustained exposure to hierarchical humiliation can
corrode empathy and distort emerging professional identities [13, 14]. Academically, mistreated students exhibit lower participation in clinical discussions, avoidance of supervisors, and reduced academic performance [15]. These psychosocial and behavioral sequelae underscore that the hidden curriculum is not merely an educational phenomenon but also a public health concern. When internalized, these negative patterns risk perpetuating cycles of disrespect in clinical practice, eroding trust between future doctors and patients, and potentially compromising patient safety [19,20]. Bandura’s social learning theory explains that students emulate behaviors modeled by authority figures, thereby normalizing hierarchical or abusive conduct [16]. Foucault’s concept of disciplinary power reveals how medical institutions subtly regulate behavior through surveillance and authority, while Bourdieu’s notion of habitus demonstrates how repeated exposure to domination shapes enduring professional dispositions [17, 18, 19].
This study draws primarily on Foucault’s theory to interpret hierarchical practices and on Bourdieu’s framework to understand how students internalize these dynamics. Consequently, critical questions remain unanswered: How do Nigerian medical students make sense of institutionalized authority? What coping mechanisms allow them to survive emotionally taxing learning environments? And how do these experiences shape their emerging professional identities? Therefore, this study explores how the hidden curriculum manifests through lecturer–student power relations and experiences of mistreatment among medical students at the University of Calabar.
By employing a phenomenological design, the research seeks to uncover the depth and complexity of students’ lived experiences, emotional interpretations, and coping mechanisms, dimensions that quantitative data alone cannot reveal.
Materials & Methods
Design and setting(s)
This study adopted a phenomenological qualitative design to explore the lived experiences of medical students regarding hidden curricula and lecturer–student power dynamics at the University of Calabar (UNICAL) [20,21]. The central research question guiding this design was: How do medical students at UNICAL experience and interpret hidden curricula and lecturer–student power relations in their training environment? Phenomenology was chosen because it captures the essence of participants’ lived experiences, emphasizing subjective perceptions, emotions, and meanings that shape academic engagement and professional identity. A Husserlian framework guided the inquiry, emphasizing descriptive experiences and the process of bracketing researcher preconceptions to ensure participants’ voices remained central [24,25]. This approach was preferred over Heideggerian phenomenology, which emphasizes interpretation, as the study sought to describe experiences of power dynamics without researcher-imposed meaning.
The study was conducted within the Faculty of Allied Medical Sciences, University of Calabar, which comprises the Departments of Nursing Science, Physiotherapy, Radiography, and Human Nutrition & Dietetics. This faculty represents diverse health-related programs with hierarchical teaching structures, frequent lecturer–student interactions, and combined theoretical and clinical exposures [26,27].
The setting mirrors the broader sociocultural context of Nigerian medical schools, where power hierarchies, professional expectations, and resource constraints shape both the formal and hidden curricula [28,29]. Previous studies in similar contexts show that over 60% of medical students report verbal abuse or humiliation from lecturers, underscoring the national relevance of this issue [30–32].
Data collection was conducted over a three-month period, from 10 March 2024 to 28 May 2024, encompassing all phases of participant recruitment, scheduling, and completion of the Focus Group Discussions (FGDs).”
Participants and sampling
A total of 40 students were purposively selected, comprising 10 participants from each department, consistent with phenomenological principles emphasizing information richness over numerical breadth [34, 35]. Inclusion criteria were: (1) current enrollment in 300-level or above, (2) completion of at least one clinical posting, and (3) willingness to share experiences freely. Students on academic suspension or those below 300 level were excluded.
Participants were recruited through departmental notice boards and class WhatsApp groups, allowing voluntary, private contact with the researcher.
To reduce coercion, recruitment, and FGDs were conducted off-campus, and no lecturer participated in the recruitment process. This ensured participants’ autonomy and confidentiality in expressing sensitive opinions about lecturers. Sample adequacy was determined through data saturation, the point at which no new themes or insights emerged [36, 37].
Monitoring occurred concurrently with data collection and preliminary analysis, typically reached between the 8th and 10th FGDs [38, 39].
The researcher’s insider position was acknowledged as both a strength and a potential source of bias. Reflexivity strategies included reflective journaling after each FGD to document assumptions, emotional responses, and interpretive decisions, and weekly peer debriefing with qualitative experts to challenge subjectivity [40, 41]. An audit trail documented all methodological decisions, ensuring transparency and dependability.
Tools/Instruments
Data were collected using a semi-structured FGD guide developed from literature on hidden curricula, professional socialization, and power dynamics [42, 43]. The guide was informed by Hafferty’s Hidden Curriculum Theory and Bourdieu’s Theory of Power and Habitus, providing theoretical grounding for exploring hierarchical interactions in medical education. The instrument was reviewed by three qualitative research experts for content validity and pilot-tested with two students outside the study sample, leading to refinement of emotionally charged questions to encourage openness (Table 1).
Note: The FGD guide was developed based on literature on hidden curricula and power dynamics, and was pilot-tested prior to use.
Data collection methods
Data collection methods
Data were obtained through FGDs lasting 45–60 minutes, facilitated by the principal investigator to ensure consistency. All FGDs were conducted in private, neutral settings outside faculty buildings to enhance participant comfort. Discussions were audio-recorded with consent and transcribed verbatim.
Field notes captured non-verbal cues, emotional tones, and contextual observations, which were integrated with transcripts during analysis to deepen interpretation. The facilitator maintained reflexive awareness by documenting emotional reactions and potential influence on questioning style. A referral protocol was developed for participants who experienced emotional distress, ensuring access to the university counselling unit. Participants were reminded of their right to withdraw at any point without penalty [44, 45]. Confidentiality was maintained through anonymization of data, and transcripts were stored in encrypted, password-protected files. To ensure phenomenological rigor and minimize researcher bias, bracketing was systematically implemented. Before each FGD, the researcher kept a reflective journal to identify personal assumptions, expectations, and prior experiences related to lecturer–student dynamics.
This process helped to suspend preconceptions and facilitate discussions that centered on participants’ authentic voices. During FGDs, reflexive memos were recorded to document immediate reactions, emotional responses, and contextual nuances that could influence interpretation. Post-FGD, the research team conducted peer debriefing sessions, collectively reviewing transcripts and field notes to cross-check emerging interpretations and challenge potential bias. This iterative process ensured that themes and subthemes accurately reflected participants’ lived experiences and not the researcher’s subjective views.
Data analysis
Data analysis followed Colaizzi’s seven-step phenomenological method [46, 47]: (1) Reading all FGD transcripts repeatedly to gain a comprehensive understanding of participants’ experiences. (2) Extracting significant statements related to lecturer misconduct, hidden curricula, and power dynamics. (3) Formulating meanings from these significant statements while staying close to the participants’ wording. (4) Clustering these meanings into emerging themes and subthemes reflects shared experiences across FGDs. (5) Developing exhaustive descriptions of each phenomenon, integrating both verbal statements and non-verbal field notes. (6) Identifying the essential structure of students’ lived experiences regarding hidden curricula and power relations. (7) Validating findings through member checking with selected participants to confirm authenticity and accuracy. (8) Coding and data management were performed using NVivo 12 software. A second qualitative researcher independently coded 20% of transcripts to enhance inter-coder reliability. Coding discrepancies were resolved through discussion and consensus. Thematic saturation was confirmed when no new themes emerged across the final FGDs.
Rigor
Trustworthiness was established following Lincoln and Guba’s criteria [48, 49]:
Credibility: achieved through member checking, triangulation of FGDs, field notes, and journals, and peer debriefing.
Dependability: ensured through a detailed audit trail documenting all methodological decisions.
Confirmability: maintained through reflective journaling and data source triangulation.
Transferability: enhanced by providing thick descriptions of context, participant diversity, and departmental structure.
Member checking involved sharing synthesized theme summaries with five participants to confirm accuracy and representativeness.
Results
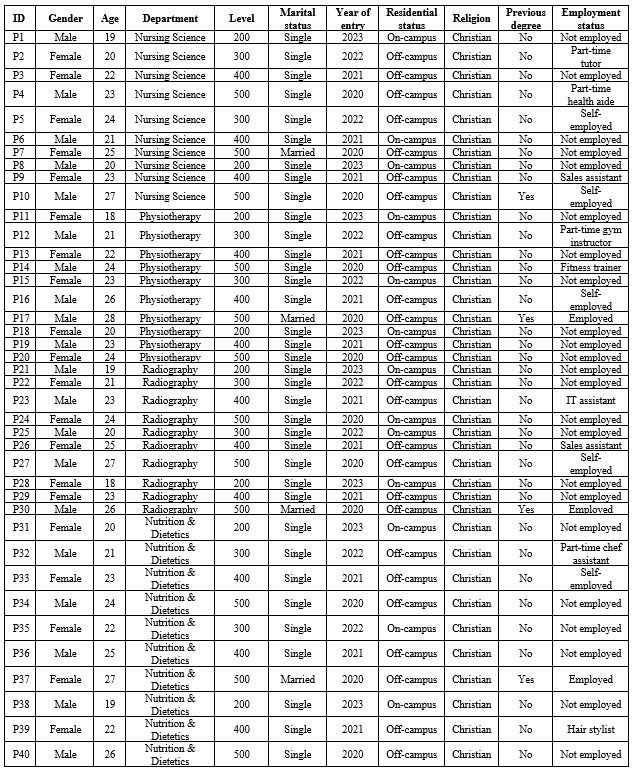
The study involved forty participants (P1–P40) drawn from diverse academic programs within the allied health sciences. Participants ranged in age from late adolescence to young adulthood, with both males and females represented across all study levels from 200 to 500. Although the majority were single, a few were married.
Their educational journeys also differed, as indicated by varied years of entry and progression patterns. Participants resided on or off campus, and all self-identified as Christians. Several held part-time jobs, ranging from tutoring and fitness training to sales and small-scale entrepreneurship, whereas others were full-time students with no employment responsibilities. A few individuals also reported having previous degrees (Table 2). The study employed 10 FGDs, each with 4 participants. Sessions lasted 60–75 minutes and were audio-recorded. Analysis followed Colaizzi’s seven-step method:
Table 2. Sociodemographic characteristics of participants (n = 40)Field notes captured non-verbal cues, emotional tones, and contextual observations, which were integrated with transcripts during analysis to deepen interpretation. The facilitator maintained reflexive awareness by documenting emotional reactions and potential influence on questioning style. A referral protocol was developed for participants who experienced emotional distress, ensuring access to the university counselling unit. Participants were reminded of their right to withdraw at any point without penalty [44, 45]. Confidentiality was maintained through anonymization of data, and transcripts were stored in encrypted, password-protected files. To ensure phenomenological rigor and minimize researcher bias, bracketing was systematically implemented. Before each FGD, the researcher kept a reflective journal to identify personal assumptions, expectations, and prior experiences related to lecturer–student dynamics.
This process helped to suspend preconceptions and facilitate discussions that centered on participants’ authentic voices. During FGDs, reflexive memos were recorded to document immediate reactions, emotional responses, and contextual nuances that could influence interpretation. Post-FGD, the research team conducted peer debriefing sessions, collectively reviewing transcripts and field notes to cross-check emerging interpretations and challenge potential bias. This iterative process ensured that themes and subthemes accurately reflected participants’ lived experiences and not the researcher’s subjective views.
Data analysis
Data analysis followed Colaizzi’s seven-step phenomenological method [46, 47]: (1) Reading all FGD transcripts repeatedly to gain a comprehensive understanding of participants’ experiences. (2) Extracting significant statements related to lecturer misconduct, hidden curricula, and power dynamics. (3) Formulating meanings from these significant statements while staying close to the participants’ wording. (4) Clustering these meanings into emerging themes and subthemes reflects shared experiences across FGDs. (5) Developing exhaustive descriptions of each phenomenon, integrating both verbal statements and non-verbal field notes. (6) Identifying the essential structure of students’ lived experiences regarding hidden curricula and power relations. (7) Validating findings through member checking with selected participants to confirm authenticity and accuracy. (8) Coding and data management were performed using NVivo 12 software. A second qualitative researcher independently coded 20% of transcripts to enhance inter-coder reliability. Coding discrepancies were resolved through discussion and consensus. Thematic saturation was confirmed when no new themes emerged across the final FGDs.
Rigor
Trustworthiness was established following Lincoln and Guba’s criteria [48, 49]:
Credibility: achieved through member checking, triangulation of FGDs, field notes, and journals, and peer debriefing.
Dependability: ensured through a detailed audit trail documenting all methodological decisions.
Confirmability: maintained through reflective journaling and data source triangulation.
Transferability: enhanced by providing thick descriptions of context, participant diversity, and departmental structure.
Member checking involved sharing synthesized theme summaries with five participants to confirm accuracy and representativeness.
Results
The study involved forty participants (P1–P40) drawn from diverse academic programs within the allied health sciences. Participants ranged in age from late adolescence to young adulthood, with both males and females represented across all study levels from 200 to 500. Although the majority were single, a few were married.
Their educational journeys also differed, as indicated by varied years of entry and progression patterns. Participants resided on or off campus, and all self-identified as Christians. Several held part-time jobs, ranging from tutoring and fitness training to sales and small-scale entrepreneurship, whereas others were full-time students with no employment responsibilities. A few individuals also reported having previous degrees (Table 2). The study employed 10 FGDs, each with 4 participants. Sessions lasted 60–75 minutes and were audio-recorded. Analysis followed Colaizzi’s seven-step method:
Note: Participants were purposively sampled from four allied medical science departments.
Abbreviation: ID, identifier.
Abbreviation: ID, identifier.
Theme 1: Lecturer misconduct
Students consistently described recurring experiences of humiliation, arbitrary punishment, and intimidation from lecturers. The misconduct was not occasional; it was normalized and pervasive, shaping emotional wellbeing and academic performance.
Subtheme 1.1: Public humiliation — “They shame you just to show they have power”
Participants described emotional trauma, social exposure, and internalized self-doubt resulting from humiliation: FGD 1
P1: “I walked in confident that day, fully prepared, thinking my answers were solid. Suddenly, the lecturer stopped me, pointing at me in front of everyone, saying, ‘How did you even get here? You are a disgrace.’ My heart sank; I froze. Whispers surrounded me, and I felt
trapped. I wanted to defend myself but couldn’t. For days, I replayed that moment, questioning my intelligence, my worth, my very place in this program. The shame wasn’t just emotional; it lingered physically, making me anxious even when reviewing for unrelated classes.”
P11: “It wasn’t only the words; it was the way he looked, the pause, the deliberate tone.
Every gesture screamed authority and intent to diminish me. Even when peers tried to console me, I felt invisible, broken, and doubted whether I belonged at all.”
P21: “Sometimes the humiliation was subtle: a joke about how I spoke or my accent. Small, passing comments, but they left long shadows. I doubted every answer I gave afterward, overthinking every word, fearing ridicule.”
P31: “Before each class, I would feel my stomach churn, hands tremble. At times I considered skipping just to avoid humiliation. Yet, absence would bring its own punishment. I lived in constant anticipation of shame, trying to survive rather than learn.”
FGD 2
P2: “During clinical posting, a lecturer openly compared me to someone incompetent in front of a patient. I froze, my face burning, my mind racing with humiliation and disbelief. I wanted to explain, but fear rooted me in silence. That day, the shame followed me back to the hostel, affecting my ability to sleep and study.”
P12: “One day, my notebook was ridiculed, my handwriting described as childish, unworthy. My peers’ laughter intensified the pain.
I hid my face, suppressing tears. I wanted to leave the program; the humiliation made me question my place entirely.”
P22: “The intersection of lecturer ridicule and peer observation magnified humiliation.
I felt doubly exposed, first by authority, then by those around me.”
P32: “I began journaling every insult, every incident. Writing helped process feelings, but reading back, I still felt the emotional sting, realizing humiliation leaves deep, lingering marks on self-confidence.”
Interpretive Meaning: Public humiliation served as a psychological weapon, reinforcing hierarchical dominance and undermining self-worth. Students internalized shame, impacting emotional wellbeing and learning motivation.
Subtheme 1.2: Arbitrary dismissal — “You can be sent out for almost anything”
Students reported dismissal from lectures or clinical sessions without reason, generating helplessness and academic disruption: FGD 3
P3: “I was sent out for a trivial reason, standing behind a lecturer while helping a colleague. He shouted at me to leave.
My heart raced. I lost the entire lecture, and the next quiz covered exactly that content. I felt punished for being helpful, humiliated, and powerless.”
P13: “Even minor attire mistakes, shoes not shiny, notebook unorganized, could trigger dismissal. We would stand outside for hours, under the sun, questioning why authority had become cruelty.”
P23: “I was once sent out for greeting a lecturer ‘too casually.’ The public correction, the scolding, and forced removal taught me that survival meant compliance, not learning. Later, friends marked attendance for me because I feared reprisals.”
P33: “Dismissal without explanation became a shared narrative among students. We used collective language, ‘we get sent out’ revealing normalization of arbitrary punishment and internalized helplessness.”
Interpretive meaning: Arbitrary dismissal demonstrated institutionalized power misuse. Students learned fearful compliance, sacrificing active participation and engagement.
Subtheme 1.3: Intimidation and threats — “You either obey or you fail”
Lecturers used threats, control over grading, and psychological coercion to enforce submission:
FGD 4
P4: “A lecturer openly said, ‘If I don’t like your attitude, I can fail you even if you score 90.’ Everyone knew he meant it. After that, questions were silenced. We stopped trying to clarify or correct mistakes.”
P14: “Indirect threats, comments like ‘I can make your life difficult here’ instilled anxiety. One classmate challenged a lecturer politely; later, assessment sheets showed false remarks. Fear dictated behavior, more than respect.”
P24: “We realized that even HODs suggested endurance over confrontation. The unwritten rule, obey or fail, created pervasive silence and submission.”
P34: “Threats extended beyond the classroom. Even when lecturers smiled or joked, we felt monitored, manipulated by fear. Our learning became secondary to survival.”
Interpretive meaning: Intimidation enforced silent obedience, suppressing critical thinking and eroding professional agency.
Theme 2: Power, fear, and submission
Overview: Students described a hierarchy-driven learning environment where fear dictated behavior, and submission became a survival strategy.
Subtheme 2.1: Hierarchy and power distance — “You don’t talk, you just nod”
FGD 5
P5: “Even knowing an answer, I kept quiet. Correcting a lecturer could result in being labelled rude, affecting grades. Silence became my shield.”
P15: “A classmate’s polite correction led to public rebuke. Since then, she never spoke in class. Authority was absolute, leaving no room for questioning.”
P25: “Walking into class felt like stepping onto a battlefield. You anticipate judgment in every gesture, tone, or response.”
P35: “The psychological impact was cumulative. Over time, we learned that survival demanded subordination over curiosity.”
Interpretive meaning: Students internalized the hierarchy, creating self-imposed silence, reinforcing structural dominance.
Subtheme 2.2: Culture of fear — “You don’t want to be noticed for the wrong reasons”
FGD 6
P6: “We moved like shadows. Being noticed could trigger punishment. Fear dictated interaction, attention, even study habits.”
P16: “Reporting misconduct was too risky. Those who tried were ostracized, branded troublemakers.”
P26: “Even routine greetings or eye contact carried potential peril. Anxiety became constant, shaping our daily academic experience.”
P36: “Fear was invisible but omnipresent. It dictated our behavior more than any rules.”
Interpretive Meaning: Fear acted as an invisible pedagogy, controlling behavior and suppressing voice.
Subtheme 2.3: Learned submission — “Survival means pretending everything is fine”
FGD 7
P7: “Pretending to be fine became a habit. Even when angry, we smiled, answered yes, nodded, concealed emotions.”
P17: “By final year, obedience felt natural. Resistance was emotionally costly.”
P27: “Classmates observed our adaptation and emulated it. Submission was socially reinforced.”
P37: “Survival required internalizing fear as professionalism.”
Interpretive meaning: Students adopted learned submission, embedding fear and obedience into their professional identity.
Theme 3: Resistance and coping mechanisms
Despite pervasive fear, humiliation, and intimidation, students actively developed strategies to survive, resist, and maintain some form of personal agency. Their resistance was complex, subtle, and multidimensional, encompassing emotional detachment, social support, silent rebellion, academic perseverance, and spiritual reliance.
Subtheme 3.1: Emotional detachment — “You stop expecting fairness, you just protect yourself”
Students described emotional shielding as a key coping mechanism, creating a psychological buffer against persistent lecturer misconduct:
P8: “I had to stop expecting fairness. Every time I raised my hand or answered confidently, it seemed like an invitation for ridicule. I trained myself to stay neutral, to nod and smile, pretending I wasn’t hurt. Inside, I felt the sting, but I had to survive.”
P18: “Detachment became a shield. I no longer took insults personally; they were part of the system. This saved my mental energy but slowly made learning mechanical, devoid of enthusiasm.”
P28: “I even started separating my grades from my emotions. If a lecturer scolded me for participation, I reminded myself it was about power, not ability. That realization helped me focus on content, not authority.”
P38: “Sometimes, detachment felt like numbness. I knew it was self-preservation, but it also made me disconnected from peers and even my own motivation.”
Interpretive meaning: Emotional detachment functioned as psychological survival, allowing students to maintain presence and engagement while insulating themselves from emotional damage.
Subtheme 3.2: Peer support and collective coping — “We heal each other”
Social support emerged as a critical coping mechanism. Students described informal networks where experiences were shared, validated, and collectively navigated:
FGD 9
P9: “After each class, we huddled together and debriefed. Sharing what happened validated our feelings. It felt like saying, ‘I am not crazy; this really happened.’”
P19: “Humor helped. We gave nicknames to lecturers, joked about ridiculous punishments, and laughed at shared misery. The laughter was both relief and quiet rebellion.”
P29: “We also shared strategies—how to respond without escalating, how to anticipate mood shifts, how to survive exams without attracting attention. This network became a safety net.”
P39: “Even simple gestures—like a nod or smile in solidarity—made us feel seen. We learned to lean on each other when authority felt overwhelming.”
Interpretive meaning: Peer support created resilient micro-communities, mitigating isolation and enabling adaptive strategies in a threatening academic environment.
Subtheme 3.3: Silent resistance — “We smile, but inside we know”
Students engaged in covert, symbolic acts of resistance, maintaining dignity and psychological autonomy
without confronting authority openly: FGD 10
P10: “I stopped showing immediate reactions. When insulted, I smiled politely. The smile masked defiance—inside, I refused to internalize the shame.”
P20: “We coded our resistance in humor, nicknames, and private discussions. Calling a lecturer a ‘dictator’ in our group chat was a way to reclaim power safely.”
P30: “Some of us focused on excelling academically, knowing that true competence would eventually speak louder than intimidation. It felt like silent protest—surviving and thriving without giving them control.”
P40: “Even when submitting assignments, we carefully followed rules but added subtle critiques in presentations. Small acts, but they felt like moral victory.”
Interpretive meaning: Silent resistance allowed students to assert psychological autonomy, retain self-respect, and maintain hope within a rigid, authoritarian environment.
Subtheme 3.4: Spiritual resilience — “Only god can see what we go through”
Faith and spirituality were central in coping with persistent fear, humiliation, and academic stress:
FGD 1
P1: “Prayer gave me calm. I told myself, ‘I may not be able to change him, but I can hold my integrity and trust God.’”
P11: “I visualized my efforts being rewarded in the long run. Believing in divine justice made enduring humiliation possible.”
P21: “Meditation and reflection became tools to process anger and maintain hope. Spirituality was the anchor in turbulent classrooms.”
P31: “Even when everything seemed unfair, faith reminded me that my knowledge and perseverance mattered beyond immediate approval.”
Interpretive meaning: Spiritual resilience provided internal moral and emotional support, allowing students to navigate systemic injustice without losing personal integrity.
Theme 4: Emotional and academic consequences
The combination of fear, humiliation, and hierarchical dominance led to multi-layered consequences, affecting mental health, emotional wellbeing, motivation, and academic engagement.
Students’ narratives reflected profound psychological burden and learning disruption, extending beyond the classroom.
Subtheme 4.1: Academic anxiety and loss of confidence — “Even prepared, I freeze”
Students reported anticipatory anxiety, self-doubt, and fear-induced performance decline:
FGD 7
P7: “I knew the answers, I studied hard, but standing in front of the class, my mind went blank. Fear made me forget everything.”
P17: “After repeated humiliation, I began doubting myself. Every wrong look from a lecturer felt like confirmation I wasn’t good enough.”
P27: “Even simple tasks like reading aloud or presenting slides triggered tremors, sweating, and nausea. Anxiety became a constant companion.”
P37: “This anxiety wasn’t limited to one class. It followed me to other courses. I questioned my intelligence, my capability, my very purpose as a student.”
Interpretive Meaning: Persistent fear undermined self-efficacy, creating a cycle of academic anxiety and reduced performance.
Subtheme 4.2: Examination experiences — “Tests became survival, not assessment”
Fear of bias, unpredictable grading, and authority-driven assessment dominated experiences:
FGD 8
P8: “Exams felt like traps. I wasn’t tested on knowledge alone; I was tested on my ability to navigate favor and fear.”
P18: “I second-guessed answers, worried if a lecturer disliked me, would they mark me unfairly? It was draining.”
P28: “Some of us scored poorly not due to lack of preparation but due to emotional paralysis. The classroom became a battlefield, and exams were ambushes.”
P38: “Even assignments were intimidating. A simple mistake could be exaggerated to shame or threaten us academically.”
Interpretive Meaning: Academic assessment was psychologically contaminated, turning evaluation into a source of stress rather than learning feedback.
Subtheme 4.3: Emotional distress and mental exhaustion — “Every day feels heavy”
Students narrated burnout, depressive symptoms, and emotional fatigue:
FGD 9
P9: “By the end of each semester, I felt mentally drained. I lost appetite for learning, even topics I loved.”
P19: “Sleep was erratic. I replayed humiliating incidents in my head, sometimes crying alone at night.”
P29: “Friendships helped, but the emotional burden was constant. The mental energy it took to survive each class was exhausting.”
P39: “Some classmates developed physical symptoms: headaches, stomachaches. Stress wasn’t just in our minds; it manifested in our bodies.”
Interpretive meaning: Continuous mistreatment led to psychosomatic manifestations and emotional depletion, impacting overall wellbeing.
Subtheme 4.4: Academic disengagement and loss of motivation — “I learn to survive, not to excel”
Long-term consequence: reduced engagement and internalized minimalism:
FGD 10
P10: “Eventually, I stopped asking questions. Learning was secondary to surviving humiliation.”
P20: “Motivation shifted from curiosity to mere completion. Excellence felt risky; discretion felt safer.”
P30: “Even group work became stressful. I avoided leadership roles to minimize exposure.”
P40: “Some of us considered leaving the program. The environment crushed enthusiasm, leaving only mechanical effort.”
Interpretive Meaning: The oppressive environment
created academic disengagement, transforming the educational journey from active learning to survival-based compliance.
Fundamental structure
Students’ lived experiences reveal an educational ecosystem dominated by fear, humiliation, and hierarchical authority. While some survive through detachment, peer solidarity, silent resistance, and spiritual resilience, the cumulative effect erodes confidence, engagement, and mental health. Academic participation is constrained by survival imperatives, and learning becomes subordinated to self-preservation.
Validation of findings
To ensure authenticity and rigor, findings were validated through participant confirmation, where representatives from each FGD reviewed the themes and subthemes to confirm that the interpretations faithfully represented their experiences. Reflexive journaling, peer debriefing, and triangulation across the 10 FGDs ensured interpretive credibility, reducing researcher bias and confirming that the results captured the true essence of student experiences in the academic environment
Discussion
The findings indicate that students’ experiences reflect not only individual misunderstandings but also a broader structural culture of domination within academic spaces. Participants described classroom and clinical interactions frequently characterized by humiliation, dismissal, and threats. Students recounted instances of being openly insulted, yelled at, or embarrassed in front of peers for minor academic errors or for simply asking questions. One participant stated, “During a practical, the lecturer said, “You people are the worst set this department has ever produced.’ I felt so small; I could not speak again.” These recurring experiences highlight how power is exercised and reinforced through verbal aggression and public shaming.
Such patterns are consistent with the concept of the hidden curriculum [50], in which professional norms and expectations are communicated implicitly, often through unspoken power dynamics, rather than through formal instruction. Participants further emphasized the emotional weight of these encounters, reporting anxiety, emotional withdrawal, and diminished engagement in learning. Participant 3, FGD 4, reflected, “After that day, he shouted at me, I stopped answering questions even when I knew the answers. It’s safer to just keep quiet.” These avoidance responses align with findings that fear-based learning environments trigger psychological withdrawal and reduce active participation [50]. Emotional intimidation, though often framed as disciplinary, functions as a pedagogical mechanism that discourages independent thought and fosters dependency on authority, supporting the principles of Self-Determination Theory, which posit that undermining autonomy and relatedness leads to loss of intrinsic motivation and disengagement [51].
Academic assessments emerged as another domain where power was exerted and emotional control maintained. Participants reported instances of perceived bias, favoritism, and punitive grading, despite diligent preparation. One student explained, “You study so hard, yet your results are poor.
When you go to ask why, they walk you out or say you should be grateful you even passed.” These experiences suggest that assessment practices, rather than reflecting competence, were leveraged to reinforce hierarchy and obedience, consistent with previous findings on coercive educational structures [52]. When feedback is withheld or used as a tool of humiliation, assessment transforms into an instrument of oppression [53]. Repeated exposure to such treatment contributed to emotional exhaustion, with participants reporting insomnia, low self-esteem, and a sense of helplessness.
A radiography student commented, “I used to love this course, but now I just count down to graduation. Every class feels like a battle for survival.” This statement exemplifies academic burnout [50] and reflects how toxic hierarchies can suppress professional identity and ethical engagement [54]. Participants described silence as both protective and corrosive, shielding them from immediate confrontation but gradually eroding confidence, autonomy, and moral sensitivity, a process akin to moral erosion [55]. The analysis further reveals that these relational dynamics directly impacted academic performance. Students reported diminished concentration and confidence during examinations and clinical evaluations following public ridicule or perceived favoritism.
One student stated, “You go into exams already defeated because you know your script will be judged by who likes you, not what you wrote.” Attempts to seek clarification often resulted in further humiliation, exemplified by the statement, “When I approached the lecturer to ask why I failed, he laughed and said, ‘If you can’t handle failure, you don’t belong here.’” These experiences reflect emotional neglect and institutional indifference, undermining both the integrity of the assessment process and trust in the educational system [56]. Collectively, these findings suggest that the interactions observed constitute a form of structural violence within the academic environment. Structural violence arises when social institutions produce harm by restricting individuals’ potential for growth and dignity [7]. In this study, the normalization of intimidation, absence of accountability, and lack of transparent communication perpetuate harm through emotional and moral degradation rather than physical force. The convergence of participant experiences across departments indicates systemic dysfunction rather than isolated incidents, emphasizing the pervasiveness of these power dynamics [57].
The findings underscore the urgent need for transformative educational reform. Hidden curricula rooted in fear, humiliation, and silence risk producing future health professionals who replicate similar oppressive behaviors in clinical practice. Participants highlighted the necessity of learning environments grounded in empathy, dialogue, and respect. Institutional leaders should establish transparent feedback mechanisms, enforce clear misconduct policies, and implement pedagogical training emphasizing emotional intelligence and ethical accountability. Only by addressing these structural and relational factors can allied medical education in Nigeria cultivate competent, compassionate, and socially responsible professionals. This study has several limitations. Its qualitative design and focus on a single Nigerian university limit the generalizability of the findings. Data relied on student self-reports within FGDs, a method which, while invaluable for capturing shared social experiences, may have limited the disclosure of highly personal views. Furthermore, the perspectives of lecturers were not included. Despite these limitations, the study provides in-depth, contextual insights into a critical aspect of allied medical education.
Conclusion
This study concludes that lecturer–student dynamics within allied medical education at the University of Calabar are structurally shaped by hierarchical power relations that manifest as emotional domination, academic intimidation, and institutionalized silence. The findings establish that public humiliation, punitive grading, and communication breakdowns are not isolated incidents but systematic practices embedded within the hidden curriculum that reproduce fear-based learning and moral desensitization. The study, therefore, concludes that these entrenched patterns undermine the core objectives of professional education by eroding psychological safety, intrinsic motivation, and ethical development among students.
This evidence underscores an urgent need for institutional transformation, anchored on pedagogical transparency, feedback justice, and relational ethics, to restore balance, autonomy, and trust within the educational process.
In essence, the study provides empirical confirmation that unless hierarchical abuse is confronted as an academic pathology, allied medical education risks perpetuating a generation of technically competent but ethically impaired healthcare professionals.
Ethical considerations
Ethical approval was obtained from the Cross River State Ethics Review Committee (Reference No: CRS/ERC/2024/008). Participation was voluntary, and informed consent was obtained before FGDs. Confidentiality and anonymity were strictly maintained throughout data collection, transcription, and analysis. Additional safeguards included offering breaks or referrals to professional counselling to participants who showed distress.
Measures to minimize coercion included conducting off-campus FGDs, using neutral language, and emphasizing voluntary participation before, during, and after sessions.
Artificial intelligence utilization for article writing
No artificial intelligence tools were used in the design, data collection, analysis, or writing of this manuscript. The authors confirm that all interpretations, analyses, and written content are solely the result of human scholarly effort.
Acknowledgment
The authors express profound gratitude to the allied medical students from the Departments of Physiotherapy, Nursing Science, Radiography, and Nutrition & Dietetics at the University of Calabar who generously shared their lived experiences.
Appreciation is also extended to faculty mentors who provided valuable feedback during data validation and to the Department of Physiotherapy for institutional and logistical support throughout the research process.
Conflict of interest statement
The authors declare no conflict of interest.
Author contributions
The author contributions are as follows: EOE was responsible for conceptualization, methodology, qualitative study design, data collection, formal analysis, interpretation of findings, writing the original draft, reviewing and editing, and project administration. SAI contributed to methodology, data collection, qualitative coding support, and review and editing. EOM handled data collection, supervision, validation of themes, and review and editing.
EOL performed data analysis, thematic interpretation, and review and editing. BE assisted with data collection, transcription, and critical revision of the manuscript for intellectual content. TAA provided methodological oversight and data curation.
Funding
This research received no external funding. All expenses were personally covered by the authors.
Data availability statement
The data supporting the findings of this study are not publicly available due to confidentiality agreements with participants, but may be accessed from the corresponding author upon reasonable request and with appropriate ethical clearance.
Article Type : Orginal Research |
Subject:
Medical Education
Received: 2025/10/17 | Accepted: 2025/12/14 | Published: 2026/01/1
Received: 2025/10/17 | Accepted: 2025/12/14 | Published: 2026/01/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
