
Fri, Jul 10, 2026
[Archive]
Volume 18, Issue 4 (2025)
J Med Edu Dev 2025, 18(4): 52-62 |
Back to browse issues page

Ethics code: IR.LUMS.REC.1402.011
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Gholami M, Beiranvand S, Hasanvand S, Mokhayeri Y. The effects of blended learning on nursing students' cultural competence and empathy: a quasi-experimental study. J Med Edu Dev 2025; 18 (4) :52-62
URL: http://edujournal.zums.ac.ir/article-1-2557-en.html
URL: http://edujournal.zums.ac.ir/article-1-2557-en.html

1- Department of Nursing, Social Determinants of Health Research Center, Lorestan University of Medical Sciences, Khorramabad, Iran
2- Department of Nursing, Social Determinants of Health Research Center, Lorestan University of Medical Sciences, Khorramabad, Iran ,shorangizbiranvand@yahoo.com
3- Department of Nursing, Social Determinants of Health Research Center, Lorestan University of Medical Sciences, Khorramabad, Iran.
4- Department of Health and Nutrition, Cardiovascular Research Center, Shahid Rahimi Hospital, Lorestan University of Medical Sciences, Khorramabad, Iran
2- Department of Nursing, Social Determinants of Health Research Center, Lorestan University of Medical Sciences, Khorramabad, Iran ,
3- Department of Nursing, Social Determinants of Health Research Center, Lorestan University of Medical Sciences, Khorramabad, Iran.
4- Department of Health and Nutrition, Cardiovascular Research Center, Shahid Rahimi Hospital, Lorestan University of Medical Sciences, Khorramabad, Iran
Full-Text [PDF 624 kb]
(264 Downloads)
| Abstract (HTML) (1019 Views)
Full-Text: (82 Views)
Abstract
Background & Objective: Along with the recent trend of globalization, nursing students need to have high cultural competence to provide nursing care services to patients with diverse cultural backgrounds. The purposes of this study were to explore the effects of blended learning on nursing students' cultural competence and empathy.
Materials & Methods: In this pretest-post-test quasi-experimental study with control group, 65 senior third-year undergraduate nursing students were selected using whole enumeration sampling. They were divided into two groups: intervention (n = 30) and control (n = 35) non-randomly. Content of the blended learning program was based on the framework of the Campinha-Bacot cultural competence model. The intervention group completed the educational course that had three parts (face-to-face lecture, storytelling, and case-based learning). It was carried out once weekly for three weeks, with each session lasting 2 hours. A two-hour in-person workshop using a lecture method was held according to the approved undergraduate nursing curriculum. The outcomes, including cultural competence and empathy, were measured using the Perng and Watson’s (2012) Cultural Capacity Scale and the Jefferson Scale of Empathy Health Profession Students before and two weeks after the intervention. The data were analyzed using descriptive statistics, independent t-test, paired t test and ANCOVA analysis with Stata-17 software.
Results: Most of the participants were single (n = 58, %95), male (n =33, %54) and in the sixth semester of the bachelor of nursing (n = 34, %56). An analysis of covariance (ANCOVA) between the groups showed a statistically significant difference between the changes in the mean scores of all subscales of cultural competence and cultural competence total score (F = 22.19, p < 0.001, mean difference and standard deviation 14.96 ± 9.31). No significant difference was found for the changes in the mean scores of all subscales and the empathy total score in two groups (F = 1.19, p = 0.31 mean difference and standard deviation -2.45 ± 14.36).
Conclusion: The findings of this study showed that the blended learning program may be effective in improving cultural competence among nursing students. It is recommended that nursing program managers add multicultural educational programs into curricula they use.
Campinha-Bacote defines cultural competence as a continuous process with five constructs: cultural awareness, cultural knowledge, cultural skill, cultural encounters and cultural desire [5]. These concepts of Campinha-Bacote’s model have a symbiotic relationship with each other. Therefore, they must be addressed in every encounter with the client [6]. The nursing literature has shown that the Campinha-Bacote model is the most frequently used and frequently cited framework for research. Also, the Campinha-Bacote model holds more immediate appeal because it helps address cultural competence with respect to healthcare delivery [7]. Finally, several authors have shown that Campinha-Bacote model is suitable as a framework for adding cultural competence into their practice [8,9]. Nursing students from multicultural contexts experience challenges during transcultural nursing care, suggesting a lack of cultural competence [10]. They must be aware of cultural needs, cultural values and cultural differences of their clients to provide culturally appropriate care [11]. It has been shown that neglecting cultural competence in educational approaches, ignoring the significance of culturally congruent care in clinical settings, poor intercultural communication, and not enough skills in cultural humility are the challenges that affect the cultural competence of Iranian nursing students [12].
Empathy was recognized as one of the components of cultural competence of health care professionals. Empathy can make nurses sensitive to patients’ values and culture to provide care based on cultural competence [13]. Sohrabi et al. showed that cultural competence training increases learners’ empathy in clinical setting [14]. A recent qualitative study carried out on Iranian nurses showed that not enough cultural knowledge could be related to the reduction of their empathy. The nurses who took part in the study preferred to avoid caring for patients with different cultures [15]. Thus, a high level of empathy is essential for the professional development of students in preparation for healthcare professions [16].
It has also been reported that the current cultural education in the nursing curriculum needs certain changes to improve students’ cultural competence. As it has been stated in some studies, nursing students are not self-reliant even after completing the training course on providing culturally proper care [4]. Also, findings from a recent study by Nuuyoma et al. suggest that the cultural competence of undergraduate nursing students in low- and middle-income countries needs enrichment [10]. Cultural competence cannot be achieved through traditional classroom sessions, assignments, or activities [17].
A systematic review showed that blended teaching methods with active simulation and case study approaches are necessary to improve students’ cultural competence [1]. The results of the evidence-based meta-analysis study by Li et al. showed that blended learning can effectively improve the level of knowledge and satisfaction of nursing students. They stated that there is not enough research on this topic. Therefore, development and combination into study programs must be thought about in a clear educational approach to ensure a purposeful and meaningful learning process [18]. Blended learning, with the advantages of traditional and e-learning, is an effective approach to easy access to educational materials and increasing learning effectiveness. This approach, by providing different methods, increases the attractiveness of education and also pays attention to individual differences. Considering that not all students learn in the same way, using different methods for education seems necessary [19]. Combining technology with learning, which has recently received attention and emphasis from the Ministry of Health’s Education Department, makes it easier to achieve educational goals. It supports the development of learners through the use of educational media. Also, training programs based on specific cultural models and blended learning strategies have yet to be carried out in Iran.
The lack of cultural competence training makes it difficult for Iranian nurses to answer to the increasing demands of foreign patients to provide culturally proper nursing care. To address this issue, it is essential to create a policy that helps with proper training in nursing schools. The present study aimed to find out the beneficial effects of the blended learning on the cultural competence and empathy of nursing students.
Materials & Methods
Design and setting(s)
This quasi-experimental study with a pre-test and post-test design and a control group was carried out at the School of Nursing and Midwifery, the Lorestan University of Medical Sciences, Khorramabad, Iran, From January 25, 2023 to July 2, 2023.
Participants and sampling
The study population was made up of all registered third-year undergraduate nursing students (n=70). Sixty-five nursing students were selected through a whole
enumeration method based on the study inclusion criteria. Then they were divided into two groups: intervention (n = 30) and control (n = 35) non-randomly. (Figure.1).
The inclusion criteria included the willingness to take part in the study and to complete at least three academic semesters of internship in clinical settings.
Exclusion criteria included absence of more than one session, participation in communication skills or promotion of transcultural awareness courses during the intervention and the failure to fill in the questionnaire.
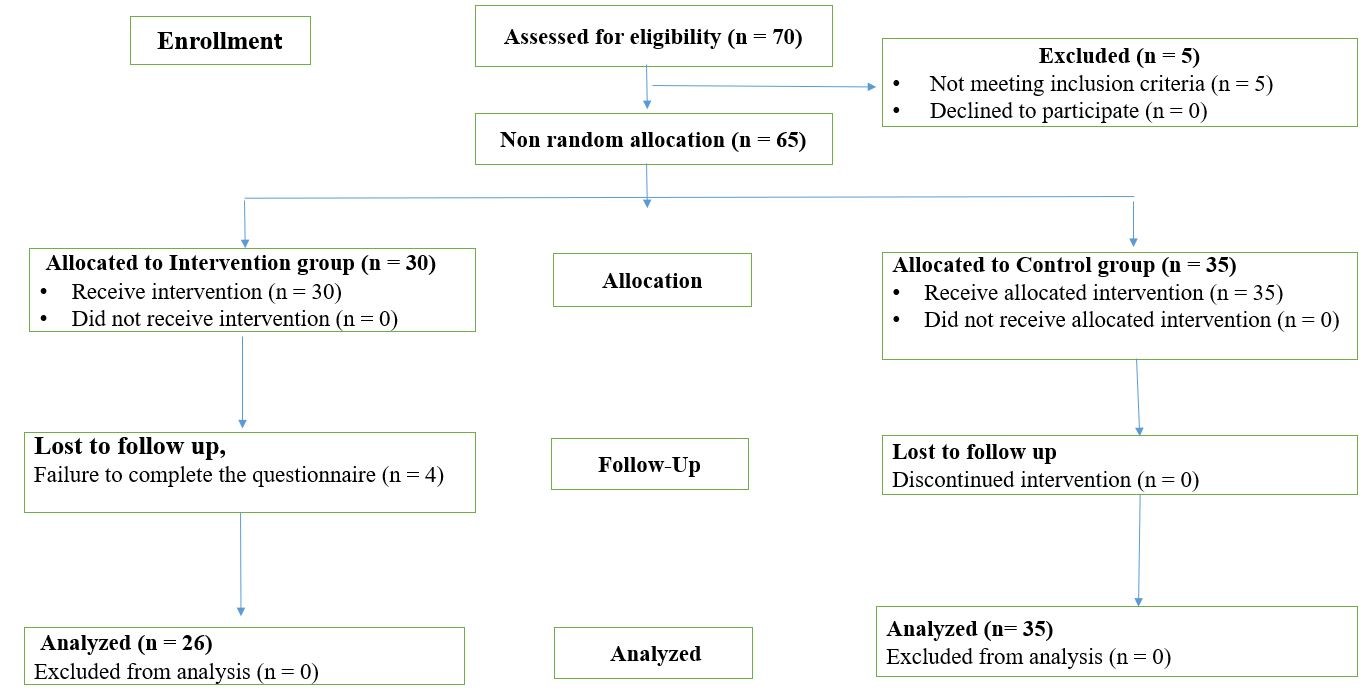
Table 1. Titles of educational content in the intervention group

Table 2. Sociodemographic characteristics of participants in intervention and control groups
A paired t-test was used to check the within-group difference in the cultural competence and empathy and its subscales before and after the intervention. In the intervention group, the results showed that the mean score on the cultural competence scale changed from 71.80 ± 9.34 in pretest to 76.84 ± 9.52 in posttest, which was a significant increase (p < 0.05, t = -2.19, Mean difference -5.03 ± 2.29). In the control group, the mean score on the cultural competence scale changed from 59.42 ± 15.5 in pretest to 61.88 ± 9.16 in posttest, which was not a significant increase (p = 0.36, t = -0.92, Mean difference -2.45).
In the intervention group, the results showed that the mean score on the empathy scale changed from 109.38 ± 14.29 in pretest to 113.92 ± 14.26 in posttest (p = 0.25, t = -1.16, Mean difference -4.53). In the control group, the mean score on the empathy changed from 116.62 ±15.5 in pretest to 116.37 ± 9.16 in posttest. In two groups, this did not show a statistically significant difference (p = 0.92, t = 0.09, Mean difference 0.257, Table 3). After adjusting the effect of the baseline competence score, between-group analysis of covariance showed a statistically significant difference between the changes in the mean scores of all subscales and the cultural competence total score of the two groups (F = 22.19, p < 0.001). However, between-group analysis of covariance did not show a statistically significant difference between the changes in the mean scores of all subscales and the empathy total score of the two groups (F = 1.19, p = 0.31, Table 4).
Table 3. Within-group comparisons of cultural competence and empathy scores before and after intervention
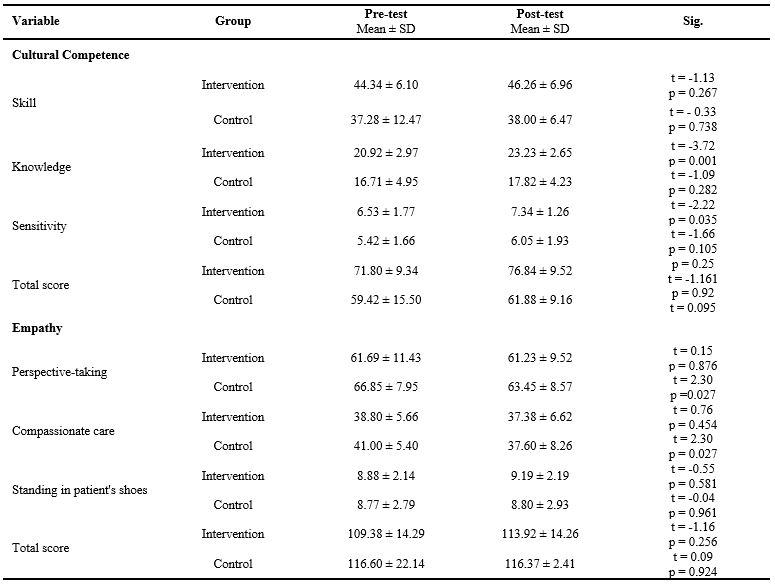
Note: Paired t-test was used for within-group comparisons.
Abbreviations: SD, standard deviation; t, paired t-test statistic; Sig., statistical significance; p, probability value.
Table 4. Between-group comparisons of cultural competence and empathy scores at posttest using ANCOVA

Note: Analysis of covariance (ANCOVA) was used for between-group comparisons, adjusting for baseline scores.
Abbreviations: SD, standard deviation; F, F-statistic from ANCOVA; p, probability value.
Discussion
In the present study, a short-term intervention with three components was carried out. This program increased nursing students' overall cultural competence and its subscales. However, it did not significantly affect their cultural skills or empathy. The study results showed that this program can be effective in improving nursing students' cultural competence. These findings were consistent with the results of a randomized controlled trial carried out by Kula et al. They found that the intervention of cultural awareness effectively strengthened the cognitive aspect of cultural competence, particularly with regard to knowledge and basic understanding [30]. The Campinha-Bacote model is complete enough to guide empirical research and the development of educational interventions. It can make significant contributions to nursing education and practice. Thus, an educational program based on an appropriate model could be useful to improve students' cultural competence and involving them in taking care of patients with different cultures [31]. Shih et al. carried out a transcultural educational program in Taiwan and Australia. Blended learning programs based on cultural competency model for health care professionals and students reduce health inequity and effectively improve the quality of health care services for migrant populations with diverse cultural norms [32]. Also, the results of this study revealed that this program could not increase either the total scores of empathy or the scores of the three related dimensions. The findings of the study by Sohrabi et al. showed that cultural competence training based on the Campinha-Bacote model increases learners' empathy in clinical settings [14]. The results of a literature review of 20 articles showed that teaching empathy, interpersonal communication skills, empathy based on mindfulness, transcultural nursing, and cultural competence had positive relationships with the level of empathy [16]. Hostility towards patients or victim blaming is a negative consequence of not enough cultural knowledge. Understanding people's behavior can be achieved by knowing the historical context, health beliefs, and practices of a specific cultural population [33]. However, theories and empirical research looking at the relationship between cultural competence and empathy are limited.
The present study used a self-report questionnaire to check the participants' empathy, which may have indirectly affected the results by response bias and social desirability bias. Fisher and Katz have described this social desirability bias in self-reported assessments [34]. Also, since a short-term intervention was carried out in the present study, this short duration of time may not have been enough to encourage empathy. In addition, study design (non-random allocation) can also affect the results. Thus, effective strategies to strengthen empathy among nursing students, as well as measures to prevent its decrease, should be implemented promptly. This issue is critical because interaction with patients is essential to patients' emotional workload and recovery process. The present study was limited to a nursing school in Western Iran. This study did not use a large sample or long-term follow-up phase. Since people were non-randomly assigned to two groups, the results and statistical inferences should be understood cautiously, and the results cannot be generalized to all nursing students. Studies with a more robust design are recommended. A larger sample size should be used in future studies. More samples from multiple sites and recruitment of nursing student participants from faculties with various backgrounds are needed. The participants of the present study expressed their willingness to take part, and their results may differ from non-volunteers due to selection bias. Therefore, further research is needed to improve our understanding of the causes of decreased empathy among nursing students.
Conclusion
The blended learning program carried out in the present study had a beneficial effect on the cultural competence of nursing students. Even though this program increased nursing students' total cultural competence significantly after the intervention, this study did not prove the effect of the blended learning program on nursing students' empathy. However, it can be a basis for future research in this field. This study has several implications. Patient culture is one of the main foundations of clinical nursing. In order to provide culturally responsive care based on this model, educational administrators should add cultural competence and empathy into the curriculum. Cultural competence and empathy can be developed in nursing students through appropriate educational strategies. Combining various strategies into the teaching-learning process appears to increase students' understanding of patients. These strategies allow for the achievement of higher cultural competence and empathy, which leads to positive outcomes for patients. Finally, this blended learning program played a crucial role in improving students' cultural competence. Students were exposed to a wide range of cultural perspectives by listening to people's experiences and engaging in case-based learning. Therefore, it is suggested that nursing program managers add multicultural educational programs into curricula they use.
Ethical considerations
This study followed the rules of the World Medical Associations or the Helsinki Declaration. This study was approved by the Ethics Committee of Lorestan University of Medical Sciences (IR.LUMS.REC.1402.011). The researchers clearly explained the research objectives and process to the participants to ensure that the data would be collected anonymously. Each participant was given a code to protect their identity. All the information obtained from the questionnaire will be kept safe to be used only for scientific research. All participants signed written informed consent forms prior to random allocation. The participants could withdraw from the study anytime during the research period without harm.
Artificial intelligence utilization for article writing
No AI tools were used for content generation, data analysis, interpretation, and English language editing.
Acknowledgment
The author gives grateful thanks to all nursing students who took part, as well as Mr. Farzad Aghaei, an experienced Iranian nurse, who lived in Germany and was invited as a guest to express his experiences.
Conflict of interest statement
The authors declare that they have no competing interests.
Author contributions
All authors took part in the design and creation of the study. ShB, and MGh. were responsible for study idea or design. ShH. and ShB.
performed the data collection. YM. analyzed and explained the participant's data. ShB, MGh, ShH and YM, were significant contributors to writing the manuscript, manuscript preparation, review, and editing. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data availability statement
Requests can be made to the corresponding author for the datasets used and analyses.
Background & Objective: Along with the recent trend of globalization, nursing students need to have high cultural competence to provide nursing care services to patients with diverse cultural backgrounds. The purposes of this study were to explore the effects of blended learning on nursing students' cultural competence and empathy.
Materials & Methods: In this pretest-post-test quasi-experimental study with control group, 65 senior third-year undergraduate nursing students were selected using whole enumeration sampling. They were divided into two groups: intervention (n = 30) and control (n = 35) non-randomly. Content of the blended learning program was based on the framework of the Campinha-Bacot cultural competence model. The intervention group completed the educational course that had three parts (face-to-face lecture, storytelling, and case-based learning). It was carried out once weekly for three weeks, with each session lasting 2 hours. A two-hour in-person workshop using a lecture method was held according to the approved undergraduate nursing curriculum. The outcomes, including cultural competence and empathy, were measured using the Perng and Watson’s (2012) Cultural Capacity Scale and the Jefferson Scale of Empathy Health Profession Students before and two weeks after the intervention. The data were analyzed using descriptive statistics, independent t-test, paired t test and ANCOVA analysis with Stata-17 software.
Results: Most of the participants were single (n = 58, %95), male (n =33, %54) and in the sixth semester of the bachelor of nursing (n = 34, %56). An analysis of covariance (ANCOVA) between the groups showed a statistically significant difference between the changes in the mean scores of all subscales of cultural competence and cultural competence total score (F = 22.19, p < 0.001, mean difference and standard deviation 14.96 ± 9.31). No significant difference was found for the changes in the mean scores of all subscales and the empathy total score in two groups (F = 1.19, p = 0.31 mean difference and standard deviation -2.45 ± 14.36).
Conclusion: The findings of this study showed that the blended learning program may be effective in improving cultural competence among nursing students. It is recommended that nursing program managers add multicultural educational programs into curricula they use.
Introduction
Along with the recent trend of globalization and increasing cultural exchanges among countries, Asian countries are also becoming multicultural [1]. Iran has also historically been a multiethnic, multi-religious, and multilingual society in which people from diverse cultures live together with their distinct sets of values [2]. Nursing students, during their clinical courses, meet different linguistic backgrounds, religious affiliations, ethnic or racial origins, immigrants, migrants, and refugees. So, their proper preparation can ensure the quality of nursing practices in the future and reduce the gaps in healthcare caused by cultural diversity. There is a need for healthcare professionals, including students, to be properly trained to be able to provide culturally competent care [3]. Nursing educators encourage nursing students to take part in extracurricular activities with people from other countries to share cultural experiences, adding this to organized lectures on cultural education [4].Campinha-Bacote defines cultural competence as a continuous process with five constructs: cultural awareness, cultural knowledge, cultural skill, cultural encounters and cultural desire [5]. These concepts of Campinha-Bacote’s model have a symbiotic relationship with each other. Therefore, they must be addressed in every encounter with the client [6]. The nursing literature has shown that the Campinha-Bacote model is the most frequently used and frequently cited framework for research. Also, the Campinha-Bacote model holds more immediate appeal because it helps address cultural competence with respect to healthcare delivery [7]. Finally, several authors have shown that Campinha-Bacote model is suitable as a framework for adding cultural competence into their practice [8,9]. Nursing students from multicultural contexts experience challenges during transcultural nursing care, suggesting a lack of cultural competence [10]. They must be aware of cultural needs, cultural values and cultural differences of their clients to provide culturally appropriate care [11]. It has been shown that neglecting cultural competence in educational approaches, ignoring the significance of culturally congruent care in clinical settings, poor intercultural communication, and not enough skills in cultural humility are the challenges that affect the cultural competence of Iranian nursing students [12].
Empathy was recognized as one of the components of cultural competence of health care professionals. Empathy can make nurses sensitive to patients’ values and culture to provide care based on cultural competence [13]. Sohrabi et al. showed that cultural competence training increases learners’ empathy in clinical setting [14]. A recent qualitative study carried out on Iranian nurses showed that not enough cultural knowledge could be related to the reduction of their empathy. The nurses who took part in the study preferred to avoid caring for patients with different cultures [15]. Thus, a high level of empathy is essential for the professional development of students in preparation for healthcare professions [16].
It has also been reported that the current cultural education in the nursing curriculum needs certain changes to improve students’ cultural competence. As it has been stated in some studies, nursing students are not self-reliant even after completing the training course on providing culturally proper care [4]. Also, findings from a recent study by Nuuyoma et al. suggest that the cultural competence of undergraduate nursing students in low- and middle-income countries needs enrichment [10]. Cultural competence cannot be achieved through traditional classroom sessions, assignments, or activities [17].
A systematic review showed that blended teaching methods with active simulation and case study approaches are necessary to improve students’ cultural competence [1]. The results of the evidence-based meta-analysis study by Li et al. showed that blended learning can effectively improve the level of knowledge and satisfaction of nursing students. They stated that there is not enough research on this topic. Therefore, development and combination into study programs must be thought about in a clear educational approach to ensure a purposeful and meaningful learning process [18]. Blended learning, with the advantages of traditional and e-learning, is an effective approach to easy access to educational materials and increasing learning effectiveness. This approach, by providing different methods, increases the attractiveness of education and also pays attention to individual differences. Considering that not all students learn in the same way, using different methods for education seems necessary [19]. Combining technology with learning, which has recently received attention and emphasis from the Ministry of Health’s Education Department, makes it easier to achieve educational goals. It supports the development of learners through the use of educational media. Also, training programs based on specific cultural models and blended learning strategies have yet to be carried out in Iran.
The lack of cultural competence training makes it difficult for Iranian nurses to answer to the increasing demands of foreign patients to provide culturally proper nursing care. To address this issue, it is essential to create a policy that helps with proper training in nursing schools. The present study aimed to find out the beneficial effects of the blended learning on the cultural competence and empathy of nursing students.
Materials & Methods
Design and setting(s)
This quasi-experimental study with a pre-test and post-test design and a control group was carried out at the School of Nursing and Midwifery, the Lorestan University of Medical Sciences, Khorramabad, Iran, From January 25, 2023 to July 2, 2023.
Participants and sampling
The study population was made up of all registered third-year undergraduate nursing students (n=70). Sixty-five nursing students were selected through a whole
enumeration method based on the study inclusion criteria. Then they were divided into two groups: intervention (n = 30) and control (n = 35) non-randomly. (Figure.1).
The inclusion criteria included the willingness to take part in the study and to complete at least three academic semesters of internship in clinical settings.
Exclusion criteria included absence of more than one session, participation in communication skills or promotion of transcultural awareness courses during the intervention and the failure to fill in the questionnaire.
Figure 1. Flowchart of the study
Table 1. Titles of educational content in the intervention group
Part 1: Introduced information on the definitions of concepts of cultural competence based on the Campinha Bacot model, communication skills, unique challenges of students in showing communication skills, an introduction to the cultural competence of nursing students, cultural diversity issues, strategies and techniques for providing culturally proper care, and an understanding of the importance of empathy and active listening taught through lectures and discussions.
Part 2: The learning content was passed on through sharing personal experiences as part of storytelling. Storytelling is defined as when nursing educators relate their clinical or other experiences to improve student learning.
The literature suggests that storytelling by nursing educators can help students combine what they learn in the classroom with what they learn in clinical settings [28]. In this stage, nursing experts (2 persons) experienced in the interaction and care of foreign immigrant families and different Iranian ethnicities were invited to express about diverse cultural backgrounds and cultural considerations. An experienced Iranian nurse living in Germany was invited through the Adobe Connect online as a guest. An Iranian nurse living in Iran with the experience of taking care of patients with different ethnicities and religions was also invited. They shared their clinical experiences taking care of patients of different races and ethnicities internationally based on the Campinha Bacot model cultural competency concepts with the students.
They were expected to train the participants how to improve their empathy toward new immigrants through storytelling.
The discussion, and questions and answers of the students with the guests of the meeting who were experienced in delivering nursing care services at international and national levels were actively guided by two nursing lecturers.
Part 3: The nursing students were involved in case-based learning. Nursing instructors used several paper-based case studies about cultural diversity for further practice and providing feedback to the participants. The students were divided into three small groups (n = 10). After reviewing the cases for about 30 to 40 minutes, the students’ answers and strategies regarding cultural care were evaluated and analyzed at the end of this unit. The cases were real and relevant [29].
The case study is an example of the application of concepts based on the Campinhabacot model that shows all its defining attributes of the concepts and helps to better express the meaning of the model concepts.
The nursing instructors approved the design of the cases and their contents. For the control group, a two-hour in-person workshop using a lecture method was held according to the approved undergraduate nursing curriculum. All courses were taught by the first author and the corresponding author currently working toward a Ph.D. in nursing education and case-based learning who were trained in cultivating multicultural competence.
Data collection methods
After getting the approval of the study from the Ethics Committee of Lorestan University of Medical Sciences, the students who provided written informed consent to take part in this study were selected. Both of the groups completed a pre-test questionnaire to collect baseline data before the intervention.
The intervention group received 6 hours of cultural competence intervention in three consecutive weeks, two hours each week. The post-test questionnaire was completed by both of the groups two weeks after the training. The participants could have been influenced by the researchers’ behavior while completing the questionnaire.
Data analysis
The data were analyzed using SPSS software version 17. Descriptive parameters such as mean and standard deviation were used.
Kolmogorov-Smirnov test was used to ensure the normality of data distribution. Independent tests, paired t-tests and the chi-square test were used for intergroup and intragroup comparisons. For the means after the intervention between the study groups, ANCOVA was used by controlling the baseline values (before the intervention). P<0.05 was considered statistically significant.
Results
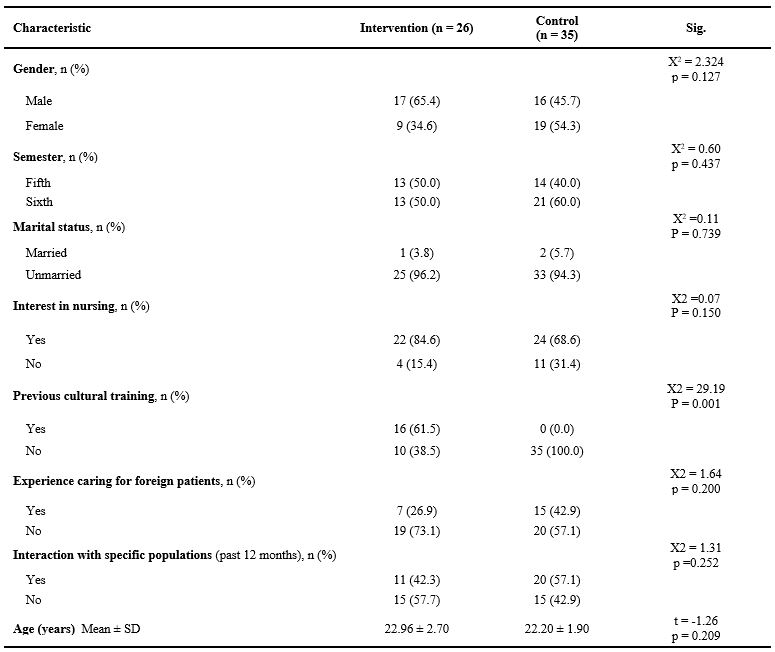
The ages of the participants ranged with the mean age of 22.52 ± 2.32 years. Most of the participants were single (n = 58, %95), male (n =33, %54) and in the sixth semester of the bachelor of nursing (n = 34, %56). program. Seventy-five percent of the participants were interested in nursing. No significant difference was found between the two groups in terms of all demographic characteristics between the two groups (p > 0.05, Table 2).
Part 2: The learning content was passed on through sharing personal experiences as part of storytelling. Storytelling is defined as when nursing educators relate their clinical or other experiences to improve student learning.
The literature suggests that storytelling by nursing educators can help students combine what they learn in the classroom with what they learn in clinical settings [28]. In this stage, nursing experts (2 persons) experienced in the interaction and care of foreign immigrant families and different Iranian ethnicities were invited to express about diverse cultural backgrounds and cultural considerations. An experienced Iranian nurse living in Germany was invited through the Adobe Connect online as a guest. An Iranian nurse living in Iran with the experience of taking care of patients with different ethnicities and religions was also invited. They shared their clinical experiences taking care of patients of different races and ethnicities internationally based on the Campinha Bacot model cultural competency concepts with the students.
They were expected to train the participants how to improve their empathy toward new immigrants through storytelling.
The discussion, and questions and answers of the students with the guests of the meeting who were experienced in delivering nursing care services at international and national levels were actively guided by two nursing lecturers.
Part 3: The nursing students were involved in case-based learning. Nursing instructors used several paper-based case studies about cultural diversity for further practice and providing feedback to the participants. The students were divided into three small groups (n = 10). After reviewing the cases for about 30 to 40 minutes, the students’ answers and strategies regarding cultural care were evaluated and analyzed at the end of this unit. The cases were real and relevant [29].
The case study is an example of the application of concepts based on the Campinhabacot model that shows all its defining attributes of the concepts and helps to better express the meaning of the model concepts.
The nursing instructors approved the design of the cases and their contents. For the control group, a two-hour in-person workshop using a lecture method was held according to the approved undergraduate nursing curriculum. All courses were taught by the first author and the corresponding author currently working toward a Ph.D. in nursing education and case-based learning who were trained in cultivating multicultural competence.
Data collection methods
After getting the approval of the study from the Ethics Committee of Lorestan University of Medical Sciences, the students who provided written informed consent to take part in this study were selected. Both of the groups completed a pre-test questionnaire to collect baseline data before the intervention.
The intervention group received 6 hours of cultural competence intervention in three consecutive weeks, two hours each week. The post-test questionnaire was completed by both of the groups two weeks after the training. The participants could have been influenced by the researchers’ behavior while completing the questionnaire.
Data analysis
The data were analyzed using SPSS software version 17. Descriptive parameters such as mean and standard deviation were used.
Kolmogorov-Smirnov test was used to ensure the normality of data distribution. Independent tests, paired t-tests and the chi-square test were used for intergroup and intragroup comparisons. For the means after the intervention between the study groups, ANCOVA was used by controlling the baseline values (before the intervention). P<0.05 was considered statistically significant.
Results
The ages of the participants ranged with the mean age of 22.52 ± 2.32 years. Most of the participants were single (n = 58, %95), male (n =33, %54) and in the sixth semester of the bachelor of nursing (n = 34, %56). program. Seventy-five percent of the participants were interested in nursing. No significant difference was found between the two groups in terms of all demographic characteristics between the two groups (p > 0.05, Table 2).
Table 2. Sociodemographic characteristics of participants in intervention and control groups
Note: Chi-square test (X²) was used for categorical variables; independent t-test was used for age comparison.
Abbreviations: n, number of participants; SD, standard deviation; X², Chi-square test; t, independent t-test; Sig., statistical significance; p, probability value.
Abbreviations: n, number of participants; SD, standard deviation; X², Chi-square test; t, independent t-test; Sig., statistical significance; p, probability value.
A paired t-test was used to check the within-group difference in the cultural competence and empathy and its subscales before and after the intervention. In the intervention group, the results showed that the mean score on the cultural competence scale changed from 71.80 ± 9.34 in pretest to 76.84 ± 9.52 in posttest, which was a significant increase (p < 0.05, t = -2.19, Mean difference -5.03 ± 2.29). In the control group, the mean score on the cultural competence scale changed from 59.42 ± 15.5 in pretest to 61.88 ± 9.16 in posttest, which was not a significant increase (p = 0.36, t = -0.92, Mean difference -2.45).
In the intervention group, the results showed that the mean score on the empathy scale changed from 109.38 ± 14.29 in pretest to 113.92 ± 14.26 in posttest (p = 0.25, t = -1.16, Mean difference -4.53). In the control group, the mean score on the empathy changed from 116.62 ±15.5 in pretest to 116.37 ± 9.16 in posttest. In two groups, this did not show a statistically significant difference (p = 0.92, t = 0.09, Mean difference 0.257, Table 3). After adjusting the effect of the baseline competence score, between-group analysis of covariance showed a statistically significant difference between the changes in the mean scores of all subscales and the cultural competence total score of the two groups (F = 22.19, p < 0.001). However, between-group analysis of covariance did not show a statistically significant difference between the changes in the mean scores of all subscales and the empathy total score of the two groups (F = 1.19, p = 0.31, Table 4).
Table 3. Within-group comparisons of cultural competence and empathy scores before and after intervention
Note: Paired t-test was used for within-group comparisons.
Abbreviations: SD, standard deviation; t, paired t-test statistic; Sig., statistical significance; p, probability value.
Table 4. Between-group comparisons of cultural competence and empathy scores at posttest using ANCOVA
Note: Analysis of covariance (ANCOVA) was used for between-group comparisons, adjusting for baseline scores.
Abbreviations: SD, standard deviation; F, F-statistic from ANCOVA; p, probability value.
Discussion
In the present study, a short-term intervention with three components was carried out. This program increased nursing students' overall cultural competence and its subscales. However, it did not significantly affect their cultural skills or empathy. The study results showed that this program can be effective in improving nursing students' cultural competence. These findings were consistent with the results of a randomized controlled trial carried out by Kula et al. They found that the intervention of cultural awareness effectively strengthened the cognitive aspect of cultural competence, particularly with regard to knowledge and basic understanding [30]. The Campinha-Bacote model is complete enough to guide empirical research and the development of educational interventions. It can make significant contributions to nursing education and practice. Thus, an educational program based on an appropriate model could be useful to improve students' cultural competence and involving them in taking care of patients with different cultures [31]. Shih et al. carried out a transcultural educational program in Taiwan and Australia. Blended learning programs based on cultural competency model for health care professionals and students reduce health inequity and effectively improve the quality of health care services for migrant populations with diverse cultural norms [32]. Also, the results of this study revealed that this program could not increase either the total scores of empathy or the scores of the three related dimensions. The findings of the study by Sohrabi et al. showed that cultural competence training based on the Campinha-Bacote model increases learners' empathy in clinical settings [14]. The results of a literature review of 20 articles showed that teaching empathy, interpersonal communication skills, empathy based on mindfulness, transcultural nursing, and cultural competence had positive relationships with the level of empathy [16]. Hostility towards patients or victim blaming is a negative consequence of not enough cultural knowledge. Understanding people's behavior can be achieved by knowing the historical context, health beliefs, and practices of a specific cultural population [33]. However, theories and empirical research looking at the relationship between cultural competence and empathy are limited.
The present study used a self-report questionnaire to check the participants' empathy, which may have indirectly affected the results by response bias and social desirability bias. Fisher and Katz have described this social desirability bias in self-reported assessments [34]. Also, since a short-term intervention was carried out in the present study, this short duration of time may not have been enough to encourage empathy. In addition, study design (non-random allocation) can also affect the results. Thus, effective strategies to strengthen empathy among nursing students, as well as measures to prevent its decrease, should be implemented promptly. This issue is critical because interaction with patients is essential to patients' emotional workload and recovery process. The present study was limited to a nursing school in Western Iran. This study did not use a large sample or long-term follow-up phase. Since people were non-randomly assigned to two groups, the results and statistical inferences should be understood cautiously, and the results cannot be generalized to all nursing students. Studies with a more robust design are recommended. A larger sample size should be used in future studies. More samples from multiple sites and recruitment of nursing student participants from faculties with various backgrounds are needed. The participants of the present study expressed their willingness to take part, and their results may differ from non-volunteers due to selection bias. Therefore, further research is needed to improve our understanding of the causes of decreased empathy among nursing students.
Conclusion
The blended learning program carried out in the present study had a beneficial effect on the cultural competence of nursing students. Even though this program increased nursing students' total cultural competence significantly after the intervention, this study did not prove the effect of the blended learning program on nursing students' empathy. However, it can be a basis for future research in this field. This study has several implications. Patient culture is one of the main foundations of clinical nursing. In order to provide culturally responsive care based on this model, educational administrators should add cultural competence and empathy into the curriculum. Cultural competence and empathy can be developed in nursing students through appropriate educational strategies. Combining various strategies into the teaching-learning process appears to increase students' understanding of patients. These strategies allow for the achievement of higher cultural competence and empathy, which leads to positive outcomes for patients. Finally, this blended learning program played a crucial role in improving students' cultural competence. Students were exposed to a wide range of cultural perspectives by listening to people's experiences and engaging in case-based learning. Therefore, it is suggested that nursing program managers add multicultural educational programs into curricula they use.
Ethical considerations
This study followed the rules of the World Medical Associations or the Helsinki Declaration. This study was approved by the Ethics Committee of Lorestan University of Medical Sciences (IR.LUMS.REC.1402.011). The researchers clearly explained the research objectives and process to the participants to ensure that the data would be collected anonymously. Each participant was given a code to protect their identity. All the information obtained from the questionnaire will be kept safe to be used only for scientific research. All participants signed written informed consent forms prior to random allocation. The participants could withdraw from the study anytime during the research period without harm.
Artificial intelligence utilization for article writing
No AI tools were used for content generation, data analysis, interpretation, and English language editing.
Acknowledgment
The author gives grateful thanks to all nursing students who took part, as well as Mr. Farzad Aghaei, an experienced Iranian nurse, who lived in Germany and was invited as a guest to express his experiences.
Conflict of interest statement
The authors declare that they have no competing interests.
Author contributions
All authors took part in the design and creation of the study. ShB, and MGh. were responsible for study idea or design. ShH. and ShB.
performed the data collection. YM. analyzed and explained the participant's data. ShB, MGh, ShH and YM, were significant contributors to writing the manuscript, manuscript preparation, review, and editing. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data availability statement
Requests can be made to the corresponding author for the datasets used and analyses.
Article Type : Orginal Research |
Subject:
Education
Received: 2025/08/6 | Accepted: 2025/11/14 | Published: 2025/11/19
Received: 2025/08/6 | Accepted: 2025/11/14 | Published: 2025/11/19
References
1. Albougami AS, Pounds KG, Alotaibi JS. Comparison of four cultural competence models in transcultural nursing: a discussion paper. Int Arch Nurs Health Care. 2016;2(4):1-5. [DOI:10.23937/2469-5823/1510053]
2. Almutairi AF, McCarthy A, Gardner GE. Understanding cultural competence in a multicultural nursing workforce: registered nurses' experience in Saudi Arabia. J Transcult Nurs. 2015;26(1):16-23. [DOI:10.1177/1043659614523992] [PMID]
3. Amiri R, Heydari A. Nurses' experiences of caring for patients with different cultures in Mashhad, Iran. Iran J Nurs Midwifery Res. 2017;22(3):232-236.
4. Arbour M, Kaspar RW, Teall AM. Strategies to promote cultural competence in distance education. J Transcult Nurs. 2015;26(4):436-440. [DOI:10.1177/1043659614547201] [PMID]
5. Attenborough J, Abbott S. Using storytelling in nurse education: the experiences and views of lecturers in a higher education institution in the United Kingdom. Nurse Educ Pract. 2020;44:102762. [DOI:10.1016/j.nepr.2020.102762] [PMID]
6. Bauer K, Bai Y. Using a model to design activity-based educational experiences to improve cultural competency among graduate students. Pharmacy (Basel). 2018;6(2):48. [DOI:10.3390/pharmacy6020048] [PMID] []
7. Cai D, Kunaviktikul W, Klunklin A, Sripusanapan A, Avant PK. Identifying the essential components of cultural competence in a Chinese nursing context: a qualitative study. Nurs Health Sci. 2017;19(2):157-162. [DOI:10.1111/nhs.12308] [PMID]
8. Choi JS, Kim JS. Effects of cultural education and cultural experiences on the cultural competence among undergraduate nursing students. Nurse Educ Pract. 2018;29:159-162. [DOI:10.1016/j.nepr.2018.01.007] [PMID]
9. De Beer J, Chipps J. A survey of cultural competence of critical care nurses in KwaZulu-Natal. SAJCC. 2014;30(2):50-54. [DOI:10.7196/SAJCC.188]
10. Fisher RJ, Katz JE. Social-desirability bias and the validity of self-reported values. Psychol Mark. 2000;17(2):105-120.
https://doi.org/10.1002/(SICI)1520-6793(200002)17:2<105::AID-MAR3>3.0.CO;2-9 [DOI:10.1002/(SICI)1520-6793(200002)17:23.0.CO;2-9]
11. Hafeez M, Akhter Y. Effects of blended learning in comparison of traditional learning to provide safer learning environment-a comparative review. IJERSC. 2021;2(6):1604-1615. [DOI:10.51601/ijersc.v2i6.209]
12. Hashemipour M, Karami M. Validity and reliability of the Persian version of JSPE-HP questionnaire (Jefferson scale of physician empathy-health professional's version). J Kerman Univ Med Sci. 2012;19(6):201-211.
13. Henderson S, Horne M, Hills R, Kendall E. Cultural competence in healthcare in the community: a concept analysis. Health Soc Care Community. 2018;26(4):590-603. [DOI:10.1111/hsc.12556] [PMID]
14. Hojat M, Louis DZ, Markham FW, Wender R, Rabinowitz C, Gonnella JS. Physicians' empathy and clinical outcomes for diabetic patients. Acad Med. 2011;86(3):359-364. [DOI:10.1097/ACM.0b013e3182086fe1] [PMID]
15. Hsiao CY, Tsai YF, Kao YC. Psychometric properties of a Chinese version of the Jefferson Scale of Empathy-Health Profession Students. J Psychiatr Ment Health Nurs. 2013;20(10):866-873. [DOI:10.1111/jpm.12024] [PMID]
16. Jongen C, McCalman J, Bainbridge R. Health workforce cultural competency interventions: a systematic scoping review. BMC Health Serv Res. 2018;18(1):232. [DOI:10.1186/s12913-018-3001-5] [PMID] []
17. Johnson JM, MacDonald CD, Oliver L. Recommendations for healthcare providers preparing to work in the Middle East: a Campinha-Bacote cultural competence model approach. J Nurs Educ Pract. 2017;7(2):25-30. [DOI:10.5430/jnep.v7n2p25]
18. Khachian A, Zarei MR, Haghani H, Khani F. The correlation between the cultural competence of nurses with their care behaviors in the teaching health centers affiliated to Iran university of medical sciences. Iran J Nurs. 2020;33(124):70-81.
19. Kula Y, Cohen O, Clempert N, Grinstein-Cohen O, Slobodin O. Educating nursing students for cultural competence in emergencies: a randomized controlled trial. BMC Nurs. 2021;20(1):143. [DOI:10.1186/s12912-021-00704-1] [PMID] []
20. Li C, He J, Yuan C, Chen B, Sun Z. The effects of blended learning on knowledge, skills, and satisfaction in nursing students: a meta-analysis. Nurse Educ Today. 2019;82:51-57. [DOI:10.1016/j.nedt.2019.08.004] [PMID]
21. Ličen S, Prosen M. The development of cultural competences in nursing students and their significance in shaping the future work environment: a pilot study. BMC Med Educ. 2023;23(1):819. [DOI:10.1186/s12909-023-04800-5] [PMID] []
22. Mahmoodi A, Khani L, Ghaffari M. The Relationship of cultural competence and responsibility with nurses attitude toward patient's right: the mediating role of ethical beliefs. Iran J Med Ethics Hist Med. 2017;9(5):39-51.
23. Marja SL, Suvi A. Cultural competence learning of the health care students using simulation pedagogy: an integrative review. Nurse Educ Pract. 2021;52:103044. [DOI:10.1016/j.nepr.2021.103044] [PMID]
24. Nematollahi M, Farokhzadian J, Nayeri ND, Darban F, Faramarzpour M. Explaining the educational challenges in the path of cultural competence: the experiences of Iranian nursing students. J Prof Nurs. 2022;42:140-147. [DOI:10.1016/j.profnurs.2022.06.011] [PMID]
25. Nuuyoma V, Muvumwaeni S, Chihururu L. Transcultural nursing: a qualitative analysis of nursing students' experiences in a multicultural context in North-Eastern Namibia. BMC Nurs. 2024;23(1):123. [DOI:10.1186/s12912-024-01773-8] [PMID] []
26. Perng SJ, Watson R. Construct validation of the nurse cultural competence scale: a hierarchy of abilities. J Clin Nurs. 2012;21(11-12):1678-84. [DOI:10.1111/j.1365-2702.2011.03933.x] [PMID]
27. Permana B, Pandin MGR. How to Enhance Empathy Nursing Students in Education: literature Review. medRxiv [Preprint]. 2022 [cited 2024 May 15]. Available from: [DOI:10.1101/2022.01.01.22268600]
28. Sharifi N, Adib-Hajbaghery M, Najafi M. Cultural competence in nursing: a concept analysis. Int J Nurs Stud. 2019;99:103386. [DOI:10.1016/j.ijnurstu.2019.103386] [PMID]
29. Shih HI, Cheung CHA, Huang IH, Huang MC, Kao CY. Development of a transcultural nursing program for nursing students in Taiwan. J Med Educ. 2019;23(2):86-97.
30. Shopo KD, Nuuyoma V, Chihururu L. Enhancing cultural competence in undergraduate nursing students: an integrative literature review of strategies for institutions of higher education. J Transcult Nurs. 2025;36(4):412-428. [DOI:10.1177/10436596241301407] [PMID] []
31. Sohrabi Z, Zabihi Zazoly A, Alizadeh S, Norouzi A, Ramezani G, Zhianifard A. The effect of cultural competence training on empathy of medical residents. Strides Dev Med Educ. 2022;19(1):138-144.
32. Soleimani M, Yarahmadi S. Cultural competence in critical care nurses and its relationships with empathy, job conflict, and work engagement: a cross-sectional descriptive study. BMC Nurs. 2023;22(1):113. [DOI:10.1186/s12912-023-01285-x] [PMID] []
33. Stubbe DE. Practicing cultural competence and cultural humility in the care of diverse patients. Focus (Am Psychiatr Publ). 2020;18(1):49-51. [DOI:10.1176/appi.focus.20190041] [PMID] []
34. Williams B, Brown T, Boyle M, Dousek S. Psychometric testing of the Jefferson Scale of Empathy Health Profession Students' version with Australian paramedic students. Nurs Health Sci. 2013;15(1):45-50. [DOI:10.1111/j.1442-2018.2012.00719.x] [PMID]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
