
Fri, Jul 10, 2026
[Archive]
Volume 19, Issue 1 (2026)
J Med Edu Dev 2026, 19(1): 34-43 |
Back to browse issues page

Ethics code: 4108/B.1/KEPK-FKUMS/III/2022
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Zahra R C, Dewi E, Makajil J D, Hassan H. Unpacking readiness competence: a descriptive qualitative study of health students in interprofessional online learning. J Med Edu Dev 2026; 19 (1) :34-43
URL: http://edujournal.zums.ac.ir/article-1-2544-en.html
URL: http://edujournal.zums.ac.ir/article-1-2544-en.html

1- School of Nursing, Faculty of Health Science, Universitas Muhammadiyah Surakarta, Surakarta, Jawa Tengah. Indonesia
2- School of Nursing, Faculty of Health Science, Universitas Muhammadiyah Surakarta, Surakarta, Jawa Tengah. Indonesia ,ed172@ums.ac.id
3- Nursing Department, Faculty of Medicine and Health Sciences, Universiti Malaysia Sabah, Malaysia.
4- Department of Nursing, Faculty of Medicine and Health Sciences, Universiti Tunku Abdul Rahman, Selangor, Malaysia.
2- School of Nursing, Faculty of Health Science, Universitas Muhammadiyah Surakarta, Surakarta, Jawa Tengah. Indonesia ,
3- Nursing Department, Faculty of Medicine and Health Sciences, Universiti Malaysia Sabah, Malaysia.
4- Department of Nursing, Faculty of Medicine and Health Sciences, Universiti Tunku Abdul Rahman, Selangor, Malaysia.
Keywords: interprofessional online learning, interprofessional education, readiness competence, health students, qualitative study
Full-Text [PDF 492 kb]
(132 Downloads)
| Abstract (HTML) (525 Views)
Full-Text: (52 Views)
Abstract
Background & Objective: The COVID-19 pandemic shifted Interprofessional Education (IPE) from face-to-face to online. This transition introduced challenges and raised concerns about the achievement of IPE goals. Most studies assess students’ readiness competence through scores, limited contextual or experiential exploration in Interprofessional Online Learning (IOL). This study aims to explore the readiness competence of health students during IOL.
Materials & Methods: This is a descriptive qualitative study that enables in-depth exploration of health students’ readiness and competence for IOL. Participants were selected through maximum-variation sampling to ensure balanced representation of genders and study programs. Data saturation was achieved with sixteen students. Data were collected through online in-depth interviews and analyzed using thematic analysis. Findings are presented in tables outlining themes, categories, and supporting quotations.
Results: Five main themes representing a continuum of competency readiness were identified. The first four themes revealed barriers indicating limited readiness: disconnected team synergy, concealed professional role clarity, burden of responsibility capability, passive engagement barrier. Despite these challenges, emerging adaptability was found as the fifth theme. It highlighted positive experiences such as enjoyment, time efficiency, and connectedness with peers, reflecting adaptive and collaborative competencies development.
Conclusion: Students’ competency readiness in IOL does not develop instantly but rather evolves through both barriers and adaptive learning experiences. Strengthening structured facilitation and reflective practice is recommended to help students transform initial challenge into a process of professional growth in community-based learning.
Introduction
The IOL program applied a case-based learning approach, combining synchronous and asynchronous methods via Schoology, Google Meet, WhatsApp, and Zoom. Students were divided into groups of 10–12, with each group assigned two faculty mentors. Each group included students from nursing, nutrition, physiotherapy, and public health. The IOL program lasted four weeks in June 2021. Students were tasked with creating health promotion media focused on COVID-19 and other infectious or social-religious health issues. Final outputs included leaflets, posters, and educational videos, which were distributed to the public via Instagram, YouTube, and online sessions with Muhammadiyah community organizations.
Data collection methods
Each participant was scheduled for an individual online interview via Google Meet. Each session lasted 45–60 minutes and was audio-visually recorded using screen recording tools. Participants were allowed to turn off their cameras for comfort. Interviews were transcribed verbatim. Data saturation was confirmed when no new codes emerged after the final interviews. To ensure credibility, the research team conducted member checks by contacting each participant to confirm and revise their interview statements through Google Meet. Confirmability was established by consulting a qualitative research expert with a background in nursing.
Data analysis
Thematic analysis was carried out using Braun and Clarke [9] framework. All interviews were transcribed verbatim and read several times to allow the researchers to develop a deep and intuitive familiarity with the data. Key expressions related to the research questions were identified and carefully highlighted using a color-coded system to capture nuances of teamwork, professional identity, collaboration, and roles and responsibilities within the IOL setting. These coded segments were then organized into a structured table that included open codes, refined codes, categories, and early thematic patterns. As the analysis progressed, themes were reviewed, refined, and interpreted in relation to relevant theoretical concepts, supported by illustrative quotations from participants. The analytic process was conducted manually and discussed repeatedly among the research team, allowing space for reflection and ensuring consistency of interpretation. Rigor and trustworthiness were strengthened using Forero et al. [10] criteria. Credibility was enhanced through prolonged engagement during the 4–12-week data collection period, the use of a structured interview protocol, and ongoing peer debriefing within the author team. Dependability was supported by detailed documentation of the interview guide development, data collection procedures, and analytic decision-making. Confirmability was reinforced through triangulation of interview transcripts with archival documents from the program facilitator and through member checking via Google Meet to verify and refine emerging interpretations. Transferability was achieved through maximum-variation sampling across four disciplines and through rich contextual descriptions, with data saturation reached during the final stages of coding. Coding and theme development were undertaken collaboratively, with the first and second authors serving as the primary coders. Differences in interpretation were resolved through reflective team discussions, peer review, and member checking, which contributed to the credibility and transparency of the findings. During the manuscript revision process, further reflection and re-examination of the dataset led to the identification of an additional theme. This theme emerged from the same dataset through iterative coding and analytical refinement, revealing a set of positive experiences that had not been clearly distinguished in the initial analysis.
Results
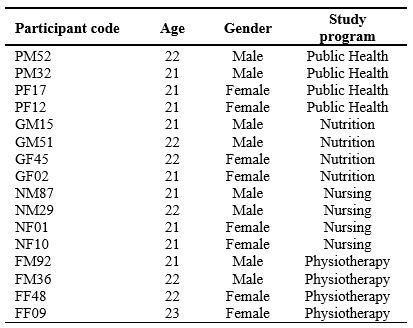
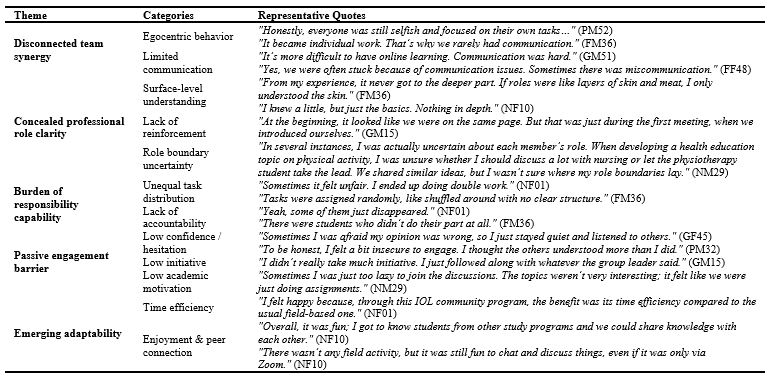
Participants varied in age, gender, and academic background (sociodemographic characteristic on Table 2). Nine students were 21 years old, six were 22, and one was 23. There was an even distribution of male and female participants. Each of the study programs, nursing, nutrition, physiotherapy, and public health, was represented by four students. The thematic analysis revealed five interrelated themes representing varying levels of students’ competency readiness in engaging with IOL. The first four themes illustrate the constraints and challenges reflecting disconnected team synergy, concealed professional role clarity, burden of responsibility capability, passive engagement barrier. Conversely, the fifth theme highlights emerging adaptability, indicating the development of positive learning dispositions and growing competency readiness (emergent themes on Table 3).
Table 2. Sociodemographic characteristics of participants
This theme reflects the students’ lack of readiness to build effective team synergy during IOL. Egocentric behavior emerged as a barrier, with many students focusing only on their individual tasks and showing little concern for team priorities. They struggled to prioritize group interests over personal responsibilities. Some participants said:
“Honestly, everyone was still selfish and focused on their own tasks. Like, ‘You have other assignments too” (PM52)
“… I didn’t really care either. Everyone seemed busy.” (FF09)
“It became individual work. That’s why we rarely have communication.” (FM36)
“Doing it online made it harder to coordinate because everyone was busy with their own task.” (FF09)
Limited communication also disrupted teamwork. Students cited technical and coordination problems in online settings. Communication was often ineffective or conducted on multiple platforms. They shared:
“It’s more difficult to have online learning. Communication was hard.” (GM51)
“Yes, we were often stuck because of communication issues. Sometimes there was miscommunication.” (FF48)
Concealed professional role clarity
This theme shows students’ limited understanding of the roles of other professions.
They mostly learned through written materials, without real-time interaction or explanations. Beyond this general lack of clarity, some students reflected on uncertainty about how their own professional boundaries overlapped with others, which sometimes led to hesitation or overstepping.
One nursing student noted:
“In several instances, I was actually uncertain about each member’s role. when developing a health education topic on physical activity, I was unsure whether I should discuss a lot with nursing or let the physiotherapy student take the lead. We shared similar ideas, but I wasn’t sure where my role boundaries lay.” (NM29)
A student described only a surface-level understanding of other professions:
“From my experience, it never got to the deeper part. If roles were like layers of skin and meat, I only understood the skin.” (FM36)
“I knew a little, but just the basics. Nothing in depth.” (NF10)
Others noted that introductions to professional identities only occurred at the start, with no follow-up or reinforcement:
“At the beginning, it looked like we were on the same page. But that was just during the first meeting, when we introduced ourselves.” (GM15)
Burden of responsibility capability
This theme illustrates the lack of accountability and uneven task sharing among students.
Several issues were raised, including delayed submissions, incomplete work, and unfair distribution of tasks:
“There were students who didn’t do their part at all.” (FM36)
“Yeah, some of them just disappeared.” (NF01)
“Tasks were assigned randomly, like shuffled around with no clear structure.” (FM36)
“Sometimes it felt unfair. I ended up doing a double work.” (NF01)
Passive engagement barrier
This theme reflects the students’ limited active involvement in IOL.
Several internal factors emerged, including low confidence, hesitation to speak, and lack of initiative. Students often remained passive or disengaged:
“Sometimes I was afraid my opinion was wrong, so I just stayed quiet and listened to others.” (GF45)
“To be honest, I felt a bit insecure to engage. I thought the others understood more than I did.” (PM32)
Students also noted poor participation in group discussions:
“Some group members were really quiet, which made it difficult to communicate—especially online.” (NM87)
“It didn’t feel fair because some people never responded.” (NM29)
“Yes, they weren’t active. They rarely joined the group chat, so sometimes discussions were skipped.” (FM36)
Lack of initiative also surfaced:
“I didn’t really take much initiative. I just followed along with whatever the group leader said.” (GM15)
In addition to personal barriers, low academic motivation contributed to disengagement. Some students felt the discussions were task-oriented and uninspiring:
“Sometimes I was just too lazy to join the discussions. The topics weren’t very interesting, it felt like we were just doing assignments.” (NM29).
Emerging adaptability
In addition to the challenges identified in earlier themes, several participants shared positive and adaptive experiences during IOL. These reflections revealed that students were able to find enjoyment, satisfaction, and a sense of efficiency in the online collaborative process. Some participants appreciated the flexibility and time-saving aspects of virtual engagement, while others highlighted the meaningful connections built with peers across different health disciplines. One participant mentioned:
“I felt happy because, through this IOL community program, the benefit was its time efficiency compared to the usual field-based one” (NF01). Another reflected, “Overall, it was fun; I got to know students from other study programs, and we could share knowledge with each other” (NF10).
Even without direct field exposure, students valued the opportunity to communicate and collaborate virtually:
“There wasn’t any field activity, but it was still fun to chat and discuss things, even if it was only via Zoom” (NF10).
These experiences demonstrate an emerging adaptability, as students began to recognize the potential of online IPE to foster interprofessional collaboration, cross-disciplinary engagement, and practical learning flexibility within a digital context.
Across all four health disciplines, the five themes consistently reflected students' experiences of competency readiness during IOL. While individual experiences varied subtly, particularly in how teamwork, role understanding, and engagement were expressed, all students faced similar challenges related to coordination, role clarity, accountability, and active participation. Notably, emerging adaptability was observed across programs, reflecting students’ capacity to find enjoyment, flexibility, and meaningful collaboration despite the online format. These findings highlight both the common barriers and shared adaptive strategies in interprofessional online learning, providing a comprehensive view of students’ readiness for collaborative practice.
Discussion
This study identified five central themes including disconnected team synergy, concealed professional role clarity, burden of responsibility capability, passive engagement barrier, and emerging adaptability, illustrating the main challenges and early positive experiences shaping students’ readiness for IOL. Alongside the challenges, students reported positive experiences including enjoyment, time efficiency, and peer connection, directly reflecting Theme 5. These findings suggest that students’ competency readiness for interprofessional online learning is not static but rather developmental, progressing from initial confusion and passivity towards adaptive and reflective engagement. The emergence of positive adaptability indicates that even within challenging online environments, learners begin to demonstrate elements of interprofessional competence readiness such as teamwork resilience, role negotiation, and digital adaptability.
The first theme, disconnected team synergy, reflects students’ difficulty in building coordinated teamwork during IOL. Egocentric attitudes and a focus on individual tasks limit their ability to prioritize collective goals. Although IOL aimed to simulate interprofessional collaboration, asynchronous communication methods, such as WhatsApp discussions, provided limited space for real-time coordination. The lack of structured and facilitated group meetings further weakened team interaction.
As noted by Jun and Binrong [11], egocentrism can hinder shared responsibility and mutual planning, which are essential for effective teamwork. Similar studies have shown that IOL settings may unintentionally reinforce individualistic behaviors and weaken interdependence among learners [12]. The second theme, concealed professional role clarity, highlights students’ limited understanding of the scope and responsibilities of other professions.
Most learning occurred through written materials, with minimal opportunities for discussion or observation of professional practice. Students often reported only surface-level comprehension, e.g., “From my experience, it never got to the deeper part. If roles were like layers of skin and meat, I only understood the skin” (FM36).
This aligns with Lewis (2020) [13], emphasizing the importance of active role clarification and reflective dialogue in developing interprofessional identity. Initial introductions to professional roles were not followed by sustained engagement, resulting in uncertainty and superficial understanding, similar to findings from other studies on online IPE [12].
The third theme, burden of responsibility capability, reveals inconsistencies in accountability and task sharing. Students reported uneven distribution of work, unclear delegation, and lack of follow-up from facilitators. Ideally, interprofessional programs assign tasks according to professional scope and learning goals to ensure fairness and relevance [14]. However, in this context, task management relied heavily on student initiative without sufficient facilitator oversight. As Khan [15] notes, effective self-regulation in online learning requires structured support rather than full autonomy. The fourth theme, passive engagement barrier, points to both internal and contextual barriers to active participation. Many students hesitated to contribute ideas, often due to low confidence or fear of making mistakes. Poorly designed online discussions and repetitive activities further reduced motivation [16]. IOL also presents challenges in fostering peer bonding within teams [17]. Minimal feedback and limited interaction with facilitators also discouraged engagement [15]. Improving IOL design could include using scenario-based learning, profession-specific video cases, and regular live discussions through structured platforms such as Zoom or Microsoft Teams [18].
The fifth theme, emerging adaptability, illustrates students’ capacity to engage positively with online interprofessional learning despite challenges. Participants highlighted enjoyment, flexibility, and efficiency, e.g., “I felt happy because, through this IOL community program, the benefit was its time efficiency compared to the usual field-based one” (NF01), and “Overall, it was fun; I got to know students from other study programs and we could share knowledge with each other” (NF10).
These adaptive experiences demonstrate early readiness competence that can be fostered through structured facilitation and culturally responsive program design. Beyond these pedagogical factors, cultural values may also help explain students’ readiness competence patterns during IOL. In Indonesian society, collectivism is deeply rooted, emphasizing group harmony and shared responsibility over individual expression [19]. Maintaining positive relationships and avoiding conflict are often prioritized, which can make students hesitant to voice disagreement or assert differing opinions in group settings.
Additionally, respect for authority is a central cultural norm, shaping how students communicate with lecturers and peers who may be perceived as more knowledgeable or senior [19].
These cultural dimensions may contribute to students’ reluctance to speak up during discussions, not necessarily due to lack of interest, but as an effort to preserve group cohesion and show deference. Understanding these underlying cultural tendencies is crucial for educators designing interprofessional online learning, as it highlights the importance of creating psychologically safe spaces that encourage participation while respecting local communication norms.
Despite these challenges, participants reported positive experiences, including flexibility, independence, and exposure to other health professions, indicating early signs of readiness competence.
Overall, findings underscore refining online interprofessional programs with clear role distribution, active facilitation, meaningful collaborative tasks, and diverse media formats.
Continuous improvement informed by student feedback and local context is essential.
Readiness competence is not only cognitive but also relational, emotional, and contextual, reflecting the development of professional and interprofessional identities in digital learning.
Future longitudinal studies could explore how collaborative skills and confidence evolve as online IPE becomes integrated into Indonesian higher education.
This study has several limitations.
All data collection activities, including in-depth interviews and member checking were conducted entirely online, which introduced technical constraints such as unstable internet connectivity and occasional disruptions during Google Meet or WhatsApp calls.
Although these interruptions did not stop the data-gathering process, they may have subtly affected the natural flow of dialogue and opportunities for deeper probing.
In addition, the one-year gap between the implementation of the community-based IPE program and the data collection period may have influenced participants’ ability to recall specific details. Some initially provided general descriptions; however, with probing and reflective questioning, they were eventually able to articulate their experiences with greater clarity.
Conclusion
This study identified five themes: disconnected team synergy, concealed professional role clarity, burden of responsibility capability, passive engagement barrier, and emerging adaptability.
Students initially faced multiple barriers in teamwork, role clarity, and active participation.
However, through continued exposure to interprofessional online activities, they gradually demonstrated adaptability and emerging competency readiness, reporting positive experiences such as enjoyment, time efficiency, and peer connections.
Structured activities, active facilitation, reflective feedback, and psychologically safe spaces are recommended to further enhance readiness competence. Overall, readiness is a multidimensional construct encompassing relational, cognitive, psychological, and contextual aspects.
Future research should examine longitudinal development of interprofessional identity and readiness in Indonesian online IPE.
Ethical considerations
Ethical approval for this study was obtained from the Ethics Commission of the Faculty of Medicine, Universitas Muhammadiyah Surakarta, with approval number 4108/B.1/KEPK-FKUMS/III/2022.
Prior to data collection, each participant received a detailed explanation of the study procedures, objectives, potential benefits, and confidentiality assurances through individual online video conference sessions conducted by the researcher.
Informed consent was obtained from all participants after they had the opportunity to ask questions and fully understand their rights and the voluntary nature of participation.
Each participant signed the consent form, which was scanned and securely stored in encrypted digital format. Only after the signed informed consent was received did the research team proceed with data collection in accordance with approved ethical protocols.
Artificial intelligence utilization for article writing
This manuscript involved the use of artificial intelligence tools, specifically Grammarly AI, to enhance language clarity, grammar accuracy, and sentence readability. The use of this tool was limited to linguistic refinement and did not influence the intellectual content, data interpretation, or conceptual development of the manuscript.
All analytical reasoning, thematic interpretation, and conclusions were entirely the authors’ own work. The authors affirm that the use of AI assistance adhered strictly to ethical guidelines for academic writing and followed institutional and publisher policies regarding transparency and responsible use of artificial intelligence in scholarly communication.
Acknowledgment
The authors would like to express sincere gratitude to Universitas Muhammadiyah Surakarta, for the research support fund, and to the Faculty of Health Sciences (FIK UMS) for the support and facilitation throughout this study.
Conflict of interest statement
There is no conflict of interest.
Author contributions
RCZ contributed to study conceptualization, methodology, data collection, formal analysis, interpretation, writing the original draft, and gave final approval. ED contributed to study conceptualization, methodology, formal analysis, interpretation, writing the original draft, reviewing and editing the manuscript, and gave final approval. JDM contributed to reviewing and editing the manuscript and gave final approval. HH contributed to reviewing the manuscript and gave final approval.
Funding
This research was supported by Universitas Muhammadiyah Surakarta and Faculty of Health Sciences (FIK UMS).
Data availability statement
The data supporting the findings of this study consist of confidential interview transcripts containing personal and professional information from participants.
In accordance with ethical approval and participant consent, these data are stored securely in the private archive of the principal researcher and are accessible only to the research team. The datasets are therefore not publicly available and cannot be shared beyond the purposes of this study, to protect participant confidentiality and comply with institutional ethical requirements.
Background & Objective: The COVID-19 pandemic shifted Interprofessional Education (IPE) from face-to-face to online. This transition introduced challenges and raised concerns about the achievement of IPE goals. Most studies assess students’ readiness competence through scores, limited contextual or experiential exploration in Interprofessional Online Learning (IOL). This study aims to explore the readiness competence of health students during IOL.
Materials & Methods: This is a descriptive qualitative study that enables in-depth exploration of health students’ readiness and competence for IOL. Participants were selected through maximum-variation sampling to ensure balanced representation of genders and study programs. Data saturation was achieved with sixteen students. Data were collected through online in-depth interviews and analyzed using thematic analysis. Findings are presented in tables outlining themes, categories, and supporting quotations.
Results: Five main themes representing a continuum of competency readiness were identified. The first four themes revealed barriers indicating limited readiness: disconnected team synergy, concealed professional role clarity, burden of responsibility capability, passive engagement barrier. Despite these challenges, emerging adaptability was found as the fifth theme. It highlighted positive experiences such as enjoyment, time efficiency, and connectedness with peers, reflecting adaptive and collaborative competencies development.
Conclusion: Students’ competency readiness in IOL does not develop instantly but rather evolves through both barriers and adaptive learning experiences. Strengthening structured facilitation and reflective practice is recommended to help students transform initial challenge into a process of professional growth in community-based learning.
Introduction
Interprofessional Education (IPE) is an educational approach designed to bring together students from diverse health professions to learn with, from, and about one another [1]. Through IPE, students are expected to develop essential interprofessional competencies encompassing values and ethics, clarity of roles and responsibilities, effective communication, and teamwork; skills that underpin lifelong collaboration and shared accountability in healthcare practice [2]. The sudden onset of the COVID-19 pandemic prompted a rapid shift of IPE delivery from face-to-face sessions to online formats. While necessary, this shift raised critical questions about whether key interprofessional competencies could still be meaningfully achieved in virtual environments. Limited direct interaction, uneven technological preparedness, and insufficient experience among both students and facilitators in managing Interprofessional Online Learning (IOL) have been commonly reported as barriers [3]. Reeves et al. [4] noted that online learning environments may foster feelings of isolation and weaken social connectedness, which can in turn diminish learners’ motivation and engagement. Similarly, Heriot et al. [5] observed that students often find it challenging to sustain active participation and collaborative initiative during online discussions, resulting in lower engagement and a less comprehensive understanding of professional roles.
Against this background, understanding students’ competency readiness has become increasingly crucial.
Within IPE, readiness competence reflects the extent to which students are prepared to engage effectively in teamwork, recognize their professional roles, and assume shared responsibility within a collaborative context [6]. Prior research has demonstrated significant associations between readiness and collaborative competence, indicating that readiness competence plays an important role in supporting effective IOL [7].
However, much of this evidence has relied primarily on quantitative readiness scores, leaving the experiential dimensions of readiness competence underexplored.
To address this gap, the present study adopts a phenomenological qualitative approach to explore health students lived experiences of competency readiness in interprofessional online learning.
Materials & Methods
Design and setting(s)
This study employed a qualitative descriptive design to explore students’ experiences and perceived competence readiness for participating in community-based interprofessional education delivered online. The research took place at a higher education institution in Indonesia.
The study was conducted from 11 March 2022 to 30 July 2022, a period marked by the transition and adaptation to IOL following the COVID-19 pandemic.
Participants and sampling
The participants were third-year health students drawn from four study programs within the Faculty of Health. A maximum variation sampling strategy was employed to ensure diversity in both gender (male and female) and academic background, encompassing nursing, physiotherapy, public health, and nutrition. Eligible participants were those who had completed the IOL program, agreed to take part in the study, and provided informed consent. Data saturation was achieved with 16 participants, comprising four students from each study program. Each discipline was represented by two male and two female students.
Research team
The lead researcher (corresponding author) was a female lecturer with a master’s degree in nursing education and specific expertise in IPE.
She had prior experience conducting qualitative research and had completed several formal trainings in qualitative methodologies.
To minimize potential bias, she did not conduct the interviews herself, as she had previously taught the participants.
Instead, the interviews were carried out by the first author, who also possessed prior experience in qualitative interviewing.
The interviewers were not personally acquainted with the participants and were of a similar age group, which helped create a comfortable environment that encouraged open and honest dialogue.
The lead researcher acknowledged that her background in nursing education and her strong commitment to IPE could have influenced the interpretation of data. Prior to the data analysis, the research team engaged in a reflexive bracketing process to identify and set aside potential pre-understandings related to interprofessional education and online learning.
Each researcher wrote short reflexive memos documenting their assumptions, prior experiences, and expectations about students’ competency readiness.
These memos were shared and discussed during a preliminary meeting to ensure awareness of possible biases and to minimize their influence on the coding and theme development. Throughout the analysis, the team continued reflexive journaling to maintain analytic transparency.
The first and second authors also performed member checking with participants to validate interpretations and documented an audit trail to ensure transparency and trustworthiness in the analytical process.
In addition, the third and fourth authors, both holding doctoral degrees in Nursing and Health Professional Education, were not involved in data collection or analysis.
Instead, they contributed to manuscript writing, provided critical review, and ensured that the final interpretation and presentation of findings were conceptually coherent and academically rigorous.
Tools/Instruments
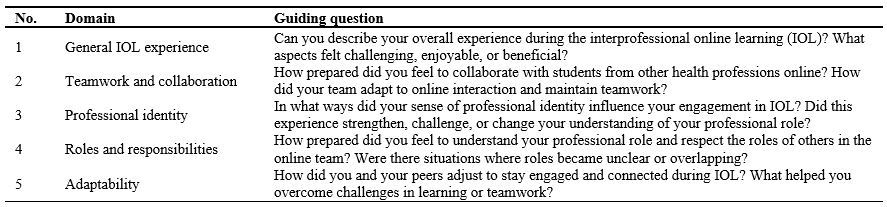
Data collection was conducted using a semi-structured interview guide.
The guide was adapted from the Readiness for Interprofessional Learning Scale (RIPLS) by Parsell & Bligh [6] and consisted of four core questions (The interview question on Table 1). The RIPLS, which had been previously translated into Indonesian [8] was used as the basis for developing the interview guide. The original 19 items were synthesized into key domains, teamwork and collaboration, professional identity, and roles and responsibilities, and rephrased into open-ended questions appropriate for in-depth interviews. The adaptation process involved a contextual review by the research team to ensure the guide's relevance to IOL within the Indonesian academic environment. Wording adjustments were made to improve cultural clarity and maintain the conceptual consistency of each domain. In addition, one probe question on adaptability was included to capture students’ adjustment and engagement experiences during IOL, reflecting the pandemic learning context.
Table 1. Semi-structured interview guide for in-depth interviews on competency readiness in interprofessional online learningAgainst this background, understanding students’ competency readiness has become increasingly crucial.
Within IPE, readiness competence reflects the extent to which students are prepared to engage effectively in teamwork, recognize their professional roles, and assume shared responsibility within a collaborative context [6]. Prior research has demonstrated significant associations between readiness and collaborative competence, indicating that readiness competence plays an important role in supporting effective IOL [7].
However, much of this evidence has relied primarily on quantitative readiness scores, leaving the experiential dimensions of readiness competence underexplored.
To address this gap, the present study adopts a phenomenological qualitative approach to explore health students lived experiences of competency readiness in interprofessional online learning.
Materials & Methods
Design and setting(s)
This study employed a qualitative descriptive design to explore students’ experiences and perceived competence readiness for participating in community-based interprofessional education delivered online. The research took place at a higher education institution in Indonesia.
The study was conducted from 11 March 2022 to 30 July 2022, a period marked by the transition and adaptation to IOL following the COVID-19 pandemic.
Participants and sampling
The participants were third-year health students drawn from four study programs within the Faculty of Health. A maximum variation sampling strategy was employed to ensure diversity in both gender (male and female) and academic background, encompassing nursing, physiotherapy, public health, and nutrition. Eligible participants were those who had completed the IOL program, agreed to take part in the study, and provided informed consent. Data saturation was achieved with 16 participants, comprising four students from each study program. Each discipline was represented by two male and two female students.
Research team
The lead researcher (corresponding author) was a female lecturer with a master’s degree in nursing education and specific expertise in IPE.
She had prior experience conducting qualitative research and had completed several formal trainings in qualitative methodologies.
To minimize potential bias, she did not conduct the interviews herself, as she had previously taught the participants.
Instead, the interviews were carried out by the first author, who also possessed prior experience in qualitative interviewing.
The interviewers were not personally acquainted with the participants and were of a similar age group, which helped create a comfortable environment that encouraged open and honest dialogue.
The lead researcher acknowledged that her background in nursing education and her strong commitment to IPE could have influenced the interpretation of data. Prior to the data analysis, the research team engaged in a reflexive bracketing process to identify and set aside potential pre-understandings related to interprofessional education and online learning.
Each researcher wrote short reflexive memos documenting their assumptions, prior experiences, and expectations about students’ competency readiness.
These memos were shared and discussed during a preliminary meeting to ensure awareness of possible biases and to minimize their influence on the coding and theme development. Throughout the analysis, the team continued reflexive journaling to maintain analytic transparency.
The first and second authors also performed member checking with participants to validate interpretations and documented an audit trail to ensure transparency and trustworthiness in the analytical process.
In addition, the third and fourth authors, both holding doctoral degrees in Nursing and Health Professional Education, were not involved in data collection or analysis.
Instead, they contributed to manuscript writing, provided critical review, and ensured that the final interpretation and presentation of findings were conceptually coherent and academically rigorous.
Tools/Instruments
Data collection was conducted using a semi-structured interview guide.
The guide was adapted from the Readiness for Interprofessional Learning Scale (RIPLS) by Parsell & Bligh [6] and consisted of four core questions (The interview question on Table 1). The RIPLS, which had been previously translated into Indonesian [8] was used as the basis for developing the interview guide. The original 19 items were synthesized into key domains, teamwork and collaboration, professional identity, and roles and responsibilities, and rephrased into open-ended questions appropriate for in-depth interviews. The adaptation process involved a contextual review by the research team to ensure the guide's relevance to IOL within the Indonesian academic environment. Wording adjustments were made to improve cultural clarity and maintain the conceptual consistency of each domain. In addition, one probe question on adaptability was included to capture students’ adjustment and engagement experiences during IOL, reflecting the pandemic learning context.
Note: The interview guide was adapted from the Readiness for Interprofessional Learning Scale (RIPLS) and contextualized for the online learning environment.
Abbreviation: IOL, interprofessional online learning.
The interprofessional online learning processAbbreviation: IOL, interprofessional online learning.
The IOL program applied a case-based learning approach, combining synchronous and asynchronous methods via Schoology, Google Meet, WhatsApp, and Zoom. Students were divided into groups of 10–12, with each group assigned two faculty mentors. Each group included students from nursing, nutrition, physiotherapy, and public health. The IOL program lasted four weeks in June 2021. Students were tasked with creating health promotion media focused on COVID-19 and other infectious or social-religious health issues. Final outputs included leaflets, posters, and educational videos, which were distributed to the public via Instagram, YouTube, and online sessions with Muhammadiyah community organizations.
Data collection methods
Each participant was scheduled for an individual online interview via Google Meet. Each session lasted 45–60 minutes and was audio-visually recorded using screen recording tools. Participants were allowed to turn off their cameras for comfort. Interviews were transcribed verbatim. Data saturation was confirmed when no new codes emerged after the final interviews. To ensure credibility, the research team conducted member checks by contacting each participant to confirm and revise their interview statements through Google Meet. Confirmability was established by consulting a qualitative research expert with a background in nursing.
Data analysis
Thematic analysis was carried out using Braun and Clarke [9] framework. All interviews were transcribed verbatim and read several times to allow the researchers to develop a deep and intuitive familiarity with the data. Key expressions related to the research questions were identified and carefully highlighted using a color-coded system to capture nuances of teamwork, professional identity, collaboration, and roles and responsibilities within the IOL setting. These coded segments were then organized into a structured table that included open codes, refined codes, categories, and early thematic patterns. As the analysis progressed, themes were reviewed, refined, and interpreted in relation to relevant theoretical concepts, supported by illustrative quotations from participants. The analytic process was conducted manually and discussed repeatedly among the research team, allowing space for reflection and ensuring consistency of interpretation. Rigor and trustworthiness were strengthened using Forero et al. [10] criteria. Credibility was enhanced through prolonged engagement during the 4–12-week data collection period, the use of a structured interview protocol, and ongoing peer debriefing within the author team. Dependability was supported by detailed documentation of the interview guide development, data collection procedures, and analytic decision-making. Confirmability was reinforced through triangulation of interview transcripts with archival documents from the program facilitator and through member checking via Google Meet to verify and refine emerging interpretations. Transferability was achieved through maximum-variation sampling across four disciplines and through rich contextual descriptions, with data saturation reached during the final stages of coding. Coding and theme development were undertaken collaboratively, with the first and second authors serving as the primary coders. Differences in interpretation were resolved through reflective team discussions, peer review, and member checking, which contributed to the credibility and transparency of the findings. During the manuscript revision process, further reflection and re-examination of the dataset led to the identification of an additional theme. This theme emerged from the same dataset through iterative coding and analytical refinement, revealing a set of positive experiences that had not been clearly distinguished in the initial analysis.
Results
Participants varied in age, gender, and academic background (sociodemographic characteristic on Table 2). Nine students were 21 years old, six were 22, and one was 23. There was an even distribution of male and female participants. Each of the study programs, nursing, nutrition, physiotherapy, and public health, was represented by four students. The thematic analysis revealed five interrelated themes representing varying levels of students’ competency readiness in engaging with IOL. The first four themes illustrate the constraints and challenges reflecting disconnected team synergy, concealed professional role clarity, burden of responsibility capability, passive engagement barrier. Conversely, the fifth theme highlights emerging adaptability, indicating the development of positive learning dispositions and growing competency readiness (emergent themes on Table 3).
Table 2. Sociodemographic characteristics of participants
Note: The table presents the sociodemographic profile of the 16 participants interviewed in this qualitative study. Participant codes denote: Study Program (P: Public Health, G: Nutrition, N: Nursing, F: Physiotherapy), Gender (M: Male, F: Female), and a unique attendance number. This diverse sample was purposefully selected to capture a range of perspectives across four health-related disciplines.
Table 3. Emergent themes, categories, and representative quotes on competency readiness in interprofessional online learningNote: Data were analyzed using thematic analysis. Quotes are presented verbatim; identifying codes are in parentheses.
Abbreviation: IOL, interprofessional online learning.
Disconnected team synergyAbbreviation: IOL, interprofessional online learning.
This theme reflects the students’ lack of readiness to build effective team synergy during IOL. Egocentric behavior emerged as a barrier, with many students focusing only on their individual tasks and showing little concern for team priorities. They struggled to prioritize group interests over personal responsibilities. Some participants said:
“Honestly, everyone was still selfish and focused on their own tasks. Like, ‘You have other assignments too” (PM52)
“… I didn’t really care either. Everyone seemed busy.” (FF09)
“It became individual work. That’s why we rarely have communication.” (FM36)
“Doing it online made it harder to coordinate because everyone was busy with their own task.” (FF09)
Limited communication also disrupted teamwork. Students cited technical and coordination problems in online settings. Communication was often ineffective or conducted on multiple platforms. They shared:
“It’s more difficult to have online learning. Communication was hard.” (GM51)
“Yes, we were often stuck because of communication issues. Sometimes there was miscommunication.” (FF48)
Concealed professional role clarity
This theme shows students’ limited understanding of the roles of other professions.
They mostly learned through written materials, without real-time interaction or explanations. Beyond this general lack of clarity, some students reflected on uncertainty about how their own professional boundaries overlapped with others, which sometimes led to hesitation or overstepping.
One nursing student noted:
“In several instances, I was actually uncertain about each member’s role. when developing a health education topic on physical activity, I was unsure whether I should discuss a lot with nursing or let the physiotherapy student take the lead. We shared similar ideas, but I wasn’t sure where my role boundaries lay.” (NM29)
A student described only a surface-level understanding of other professions:
“From my experience, it never got to the deeper part. If roles were like layers of skin and meat, I only understood the skin.” (FM36)
“I knew a little, but just the basics. Nothing in depth.” (NF10)
Others noted that introductions to professional identities only occurred at the start, with no follow-up or reinforcement:
“At the beginning, it looked like we were on the same page. But that was just during the first meeting, when we introduced ourselves.” (GM15)
Burden of responsibility capability
This theme illustrates the lack of accountability and uneven task sharing among students.
Several issues were raised, including delayed submissions, incomplete work, and unfair distribution of tasks:
“There were students who didn’t do their part at all.” (FM36)
“Yeah, some of them just disappeared.” (NF01)
“Tasks were assigned randomly, like shuffled around with no clear structure.” (FM36)
“Sometimes it felt unfair. I ended up doing a double work.” (NF01)
Passive engagement barrier
This theme reflects the students’ limited active involvement in IOL.
Several internal factors emerged, including low confidence, hesitation to speak, and lack of initiative. Students often remained passive or disengaged:
“Sometimes I was afraid my opinion was wrong, so I just stayed quiet and listened to others.” (GF45)
“To be honest, I felt a bit insecure to engage. I thought the others understood more than I did.” (PM32)
Students also noted poor participation in group discussions:
“Some group members were really quiet, which made it difficult to communicate—especially online.” (NM87)
“It didn’t feel fair because some people never responded.” (NM29)
“Yes, they weren’t active. They rarely joined the group chat, so sometimes discussions were skipped.” (FM36)
Lack of initiative also surfaced:
“I didn’t really take much initiative. I just followed along with whatever the group leader said.” (GM15)
In addition to personal barriers, low academic motivation contributed to disengagement. Some students felt the discussions were task-oriented and uninspiring:
“Sometimes I was just too lazy to join the discussions. The topics weren’t very interesting, it felt like we were just doing assignments.” (NM29).
Emerging adaptability
In addition to the challenges identified in earlier themes, several participants shared positive and adaptive experiences during IOL. These reflections revealed that students were able to find enjoyment, satisfaction, and a sense of efficiency in the online collaborative process. Some participants appreciated the flexibility and time-saving aspects of virtual engagement, while others highlighted the meaningful connections built with peers across different health disciplines. One participant mentioned:
“I felt happy because, through this IOL community program, the benefit was its time efficiency compared to the usual field-based one” (NF01). Another reflected, “Overall, it was fun; I got to know students from other study programs, and we could share knowledge with each other” (NF10).
Even without direct field exposure, students valued the opportunity to communicate and collaborate virtually:
“There wasn’t any field activity, but it was still fun to chat and discuss things, even if it was only via Zoom” (NF10).
These experiences demonstrate an emerging adaptability, as students began to recognize the potential of online IPE to foster interprofessional collaboration, cross-disciplinary engagement, and practical learning flexibility within a digital context.
Across all four health disciplines, the five themes consistently reflected students' experiences of competency readiness during IOL. While individual experiences varied subtly, particularly in how teamwork, role understanding, and engagement were expressed, all students faced similar challenges related to coordination, role clarity, accountability, and active participation. Notably, emerging adaptability was observed across programs, reflecting students’ capacity to find enjoyment, flexibility, and meaningful collaboration despite the online format. These findings highlight both the common barriers and shared adaptive strategies in interprofessional online learning, providing a comprehensive view of students’ readiness for collaborative practice.
Discussion
This study identified five central themes including disconnected team synergy, concealed professional role clarity, burden of responsibility capability, passive engagement barrier, and emerging adaptability, illustrating the main challenges and early positive experiences shaping students’ readiness for IOL. Alongside the challenges, students reported positive experiences including enjoyment, time efficiency, and peer connection, directly reflecting Theme 5. These findings suggest that students’ competency readiness for interprofessional online learning is not static but rather developmental, progressing from initial confusion and passivity towards adaptive and reflective engagement. The emergence of positive adaptability indicates that even within challenging online environments, learners begin to demonstrate elements of interprofessional competence readiness such as teamwork resilience, role negotiation, and digital adaptability.
The first theme, disconnected team synergy, reflects students’ difficulty in building coordinated teamwork during IOL. Egocentric attitudes and a focus on individual tasks limit their ability to prioritize collective goals. Although IOL aimed to simulate interprofessional collaboration, asynchronous communication methods, such as WhatsApp discussions, provided limited space for real-time coordination. The lack of structured and facilitated group meetings further weakened team interaction.
As noted by Jun and Binrong [11], egocentrism can hinder shared responsibility and mutual planning, which are essential for effective teamwork. Similar studies have shown that IOL settings may unintentionally reinforce individualistic behaviors and weaken interdependence among learners [12]. The second theme, concealed professional role clarity, highlights students’ limited understanding of the scope and responsibilities of other professions.
Most learning occurred through written materials, with minimal opportunities for discussion or observation of professional practice. Students often reported only surface-level comprehension, e.g., “From my experience, it never got to the deeper part. If roles were like layers of skin and meat, I only understood the skin” (FM36).
This aligns with Lewis (2020) [13], emphasizing the importance of active role clarification and reflective dialogue in developing interprofessional identity. Initial introductions to professional roles were not followed by sustained engagement, resulting in uncertainty and superficial understanding, similar to findings from other studies on online IPE [12].
The third theme, burden of responsibility capability, reveals inconsistencies in accountability and task sharing. Students reported uneven distribution of work, unclear delegation, and lack of follow-up from facilitators. Ideally, interprofessional programs assign tasks according to professional scope and learning goals to ensure fairness and relevance [14]. However, in this context, task management relied heavily on student initiative without sufficient facilitator oversight. As Khan [15] notes, effective self-regulation in online learning requires structured support rather than full autonomy. The fourth theme, passive engagement barrier, points to both internal and contextual barriers to active participation. Many students hesitated to contribute ideas, often due to low confidence or fear of making mistakes. Poorly designed online discussions and repetitive activities further reduced motivation [16]. IOL also presents challenges in fostering peer bonding within teams [17]. Minimal feedback and limited interaction with facilitators also discouraged engagement [15]. Improving IOL design could include using scenario-based learning, profession-specific video cases, and regular live discussions through structured platforms such as Zoom or Microsoft Teams [18].
The fifth theme, emerging adaptability, illustrates students’ capacity to engage positively with online interprofessional learning despite challenges. Participants highlighted enjoyment, flexibility, and efficiency, e.g., “I felt happy because, through this IOL community program, the benefit was its time efficiency compared to the usual field-based one” (NF01), and “Overall, it was fun; I got to know students from other study programs and we could share knowledge with each other” (NF10).
These adaptive experiences demonstrate early readiness competence that can be fostered through structured facilitation and culturally responsive program design. Beyond these pedagogical factors, cultural values may also help explain students’ readiness competence patterns during IOL. In Indonesian society, collectivism is deeply rooted, emphasizing group harmony and shared responsibility over individual expression [19]. Maintaining positive relationships and avoiding conflict are often prioritized, which can make students hesitant to voice disagreement or assert differing opinions in group settings.
Additionally, respect for authority is a central cultural norm, shaping how students communicate with lecturers and peers who may be perceived as more knowledgeable or senior [19].
These cultural dimensions may contribute to students’ reluctance to speak up during discussions, not necessarily due to lack of interest, but as an effort to preserve group cohesion and show deference. Understanding these underlying cultural tendencies is crucial for educators designing interprofessional online learning, as it highlights the importance of creating psychologically safe spaces that encourage participation while respecting local communication norms.
Despite these challenges, participants reported positive experiences, including flexibility, independence, and exposure to other health professions, indicating early signs of readiness competence.
Overall, findings underscore refining online interprofessional programs with clear role distribution, active facilitation, meaningful collaborative tasks, and diverse media formats.
Continuous improvement informed by student feedback and local context is essential.
Readiness competence is not only cognitive but also relational, emotional, and contextual, reflecting the development of professional and interprofessional identities in digital learning.
Future longitudinal studies could explore how collaborative skills and confidence evolve as online IPE becomes integrated into Indonesian higher education.
This study has several limitations.
All data collection activities, including in-depth interviews and member checking were conducted entirely online, which introduced technical constraints such as unstable internet connectivity and occasional disruptions during Google Meet or WhatsApp calls.
Although these interruptions did not stop the data-gathering process, they may have subtly affected the natural flow of dialogue and opportunities for deeper probing.
In addition, the one-year gap between the implementation of the community-based IPE program and the data collection period may have influenced participants’ ability to recall specific details. Some initially provided general descriptions; however, with probing and reflective questioning, they were eventually able to articulate their experiences with greater clarity.
Conclusion
This study identified five themes: disconnected team synergy, concealed professional role clarity, burden of responsibility capability, passive engagement barrier, and emerging adaptability.
Students initially faced multiple barriers in teamwork, role clarity, and active participation.
However, through continued exposure to interprofessional online activities, they gradually demonstrated adaptability and emerging competency readiness, reporting positive experiences such as enjoyment, time efficiency, and peer connections.
Structured activities, active facilitation, reflective feedback, and psychologically safe spaces are recommended to further enhance readiness competence. Overall, readiness is a multidimensional construct encompassing relational, cognitive, psychological, and contextual aspects.
Future research should examine longitudinal development of interprofessional identity and readiness in Indonesian online IPE.
Ethical considerations
Ethical approval for this study was obtained from the Ethics Commission of the Faculty of Medicine, Universitas Muhammadiyah Surakarta, with approval number 4108/B.1/KEPK-FKUMS/III/2022.
Prior to data collection, each participant received a detailed explanation of the study procedures, objectives, potential benefits, and confidentiality assurances through individual online video conference sessions conducted by the researcher.
Informed consent was obtained from all participants after they had the opportunity to ask questions and fully understand their rights and the voluntary nature of participation.
Each participant signed the consent form, which was scanned and securely stored in encrypted digital format. Only after the signed informed consent was received did the research team proceed with data collection in accordance with approved ethical protocols.
Artificial intelligence utilization for article writing
This manuscript involved the use of artificial intelligence tools, specifically Grammarly AI, to enhance language clarity, grammar accuracy, and sentence readability. The use of this tool was limited to linguistic refinement and did not influence the intellectual content, data interpretation, or conceptual development of the manuscript.
All analytical reasoning, thematic interpretation, and conclusions were entirely the authors’ own work. The authors affirm that the use of AI assistance adhered strictly to ethical guidelines for academic writing and followed institutional and publisher policies regarding transparency and responsible use of artificial intelligence in scholarly communication.
Acknowledgment
The authors would like to express sincere gratitude to Universitas Muhammadiyah Surakarta, for the research support fund, and to the Faculty of Health Sciences (FIK UMS) for the support and facilitation throughout this study.
Conflict of interest statement
There is no conflict of interest.
Author contributions
RCZ contributed to study conceptualization, methodology, data collection, formal analysis, interpretation, writing the original draft, and gave final approval. ED contributed to study conceptualization, methodology, formal analysis, interpretation, writing the original draft, reviewing and editing the manuscript, and gave final approval. JDM contributed to reviewing and editing the manuscript and gave final approval. HH contributed to reviewing the manuscript and gave final approval.
Funding
This research was supported by Universitas Muhammadiyah Surakarta and Faculty of Health Sciences (FIK UMS).
Data availability statement
The data supporting the findings of this study consist of confidential interview transcripts containing personal and professional information from participants.
In accordance with ethical approval and participant consent, these data are stored securely in the private archive of the principal researcher and are accessible only to the research team. The datasets are therefore not publicly available and cannot be shared beyond the purposes of this study, to protect participant confidentiality and comply with institutional ethical requirements.
Article Type : Orginal Research |
Subject:
Medical Education
Received: 2025/07/25 | Accepted: 2025/12/3 | Published: 2026/01/1
Received: 2025/07/25 | Accepted: 2025/12/3 | Published: 2026/01/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
