
Sat, Aug 1, 2026
[Archive]
Volume 18, Issue 4 (2025)
J Med Edu Dev 2025, 18(4): 111-118 |
Back to browse issues page

Ethics code: IR.TBZMED.REC.1403.633
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Jabbari Beyrami H, Fathnezhad-Kazemi A, Aghaei S. Assessing knowledge and attitudes toward palliative care among internal medicine residents: a cross-sectional study. J Med Edu Dev 2025; 18 (4) :111-118
URL: http://edujournal.zums.ac.ir/article-1-2530-en.html
URL: http://edujournal.zums.ac.ir/article-1-2530-en.html

1- Tabriz Health Services Management Research Center, Tabriz University of Medical Sciences, Tabriz, Iran.
2- Department of Midwifery, TaMS.C., Islamic Azad University, Tabriz, Iran.
3- Student Research Committee, Tabriz University of Medical Sciences, Tabriz, Iran. ,shalalehaghaei@gmail.com
2- Department of Midwifery, TaMS.C., Islamic Azad University, Tabriz, Iran.
3- Student Research Committee, Tabriz University of Medical Sciences, Tabriz, Iran. ,
Full-Text [PDF 460 kb]
(206 Downloads)
| Abstract (HTML) (1193 Views)
Full-Text: (68 Views)
Abstract
Background & Objective: The aging population and the rising prevalence of chronic diseases have made palliative care a necessity for improving individuals' quality of life. Many healthcare professionals do not possess enough training and knowledge in this regard. The objective of this study was to check the attitudes and knowledge of internal medicine residents regarding palliative care.
Materials & Methods: A cross-sectional study was performed to check the knowledge and attitudes of internal medicine residents (n = 91). A validated, structured online questionnaire was used to check demographic characteristics, palliative care knowledge (30 items), and attitudes (37 items) across four domains. The data study was done using SPSS version 24, using both descriptive and inferential statistical methods, including t-tests, ANOVA, and multiple linear regression.
Results: The mean knowledge score was 19.66 ± 2.93, and the mean attitudes score was 139.47 ± 11.44). Prior training (p = 0.041) and male gender (p = 0.009) showed a significant correlation with higher attitude scores. Knowledge scores had a positive correlation with year of residency (p = 0.033) and a negative correlation with age (p = 0.004). Despite limited knowledge, 67% of participants stated that they needed training on palliative care.
Conclusion: Despite favorable attitudes toward palliative care, the lack of knowledge, particularly in conceptual and psychological domains, should be addressed. The findings highlight the necessity of palliative care training in internal medicine residency programs.
Introduction
Table 1. Comparison of attitude and knowledge scores according to demographic and educational characteristics (n = 91)

Note: Values are presented as Mean ± SD for continuous variables and n (%) for categorical variables. Independent-samples t-test and one-way ANOVA were used for
group comparisons. A p-value < 0.05 was considered statistically significant.
Abbreviations: n, number of participants; SD, standard deviation; Sig., significance; p, probability-value.
Table 2. Distribution of attitude and knowledge subscale scores
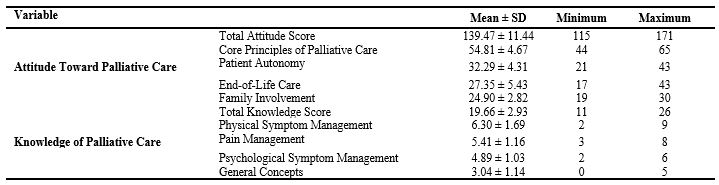
Note: Values are presented as Mean ± SD with watched minimum and maximum scores. Higher scores show more positive attitudes or greater knowledge regarding palliative care.
Abbreviations: SD, standard deviation.
Table 3. Predictors of attitude and knowledge scores: multiple linear regression analysis

Discussion
This study checked the understanding and perspectives of internal medicine residents regarding palliative care at Tabriz University of Medical Sciences, and provided valuable insights into the cognitive and affective dimensions of end-of-life care within Iran's postgraduate medical education and residency programs. The findings revealed a moderate level of knowledge and a generally positive attitude toward palliative care, though significant variations were observed among different demographic and professional subgroups.
The mean knowledge score (19.66 ± 2.93 out of 30) showed limited proficiency, especially in basic concepts of palliative care (3.04 ± 1.14), which is consistent with global literature reporting suboptimal palliative care literacy among medical trainees [24-26]. Low scores in the domains of psychological symptom management and general concepts suggest a significant gap in understanding the holistic nature of palliative care. This finding aligns with other studies showing that medical education often puts first pharmacological management, and underemphasizes topics such as grief, existential suffering, and interdisciplinary teamwork [27]. Similarly, a study among pediatric residents and fellows has shown not enough preparation in core aspects of palliative care, particularly in communication skills and pain management [28]. Despite their knowledge limitations, residents displayed generally positive attitudes, with a mean score of 139.47 ± 11.44 (out of 185). The highest attitudinal responses were observed in
the domain of basic principles. This finding shows deep ethical attention among residents toward patient-focused values such as respect, dignity, and compassion. However, lower scores in end-of-life decision-making and family engagement suggest discomfort or not training in managing the sophisticated psychosocial aspects of patient care. Previous studies also showed that medical trainees feel more confident in the theoretical and technical aspects of patient care than in communication and interpersonal relations [27, 29, 30]. Similarly, a study among pediatric residents reported minimal training, knowledge, and confidence across nearly all palliative care domains, with strong demand for further education in pain management and communication skills [31].
Further study through multiple regression revealed the key predictors of knowledge and attitudes. Gender was a significant predictor of knowledge and attitudes toward palliative care. Interestingly, male residents showed more positive attitudes than their female peers. This observation contrasts with previous studies, where female healthcare professionals showed greater empathy and openness to the principles of palliative care [13, 32].
This inconsistency may be a result of contextual factors such as cultural norms, institutional roles, or differences in clinical experiences.
Furthermore, results showed that taking part in palliative care workshops was associated with higher attitude scores; however, it had little impact on knowledge levels.
This finding suggests that short-term educational interventions may improve affective learning but are not enough to create deep cognitive learning without long-term reinforcement [33, 34].
The relationship between age, prior clinical experience, and knowledge was intricate and non-linear. Older residents generally scored lower on knowledge, whereas the highest knowledge levels were seen in residents with 4–6 years of prior experience, suggesting an optimal experience window as an "experience sweet spot" where prior exposure may improve learning receptivity. These findings align with Bloom's taxonomy, which tells apart affective learning from cognitive growth. It emphasizes that deeper competencies are best built through longitudinal, experiential approaches such as clinical rotations, mentorship, and reflective practice [35].
Notably, only 9.9% of residents had received formal education in palliative care, and only 12.1% reported prior work experience in this field. However, 67% of the residents expressed a strong interest in further training in palliative care. This highlights a systemic gap in educational opportunities, showing the World Health Organization's call to add palliative care into all levels of medical education to help universal health coverage [2]. In Iran, the growth of palliative care services must be accompanied by training competent professionals [36]. In the end, these findings highlight the urgent need for curricular reform in postgraduate medical education. Internal medicine residency programs should add structured, longitudinal palliative care training that goes beyond mere knowledge transfer and fosters ethical decision-making, interdisciplinary teamwork, and compassionate clinical communication.
This study has several limitations. First, because of its design, causal relationships cannot be confidently created. Second, the study included residents from only one university with a relatively small sample size. Thus, the generalizability of the findings is limited. Despite necessary measures to make it easier for participants virtual take part virtually, the sampling method and the procedure for questionnaire completion added further limitations.
Conclusion
In conclusion, internal medicine residents at Tabriz University of Medical Sciences showed positive attitudes toward palliative care; however, large knowledge gaps existed, particularly in foundational concepts and psychosocial domains. Structured, longitudinal, and evidence-based educational interventions are needed to improve competencies regarding palliative care delivery and fulfill the social accountability of Iran's medical education system.
Ethical considerations
This study was approved by the Research Ethics Committee of Tabriz University of Medical Sciences with the code IR.TBZMED.REC.1403.633.
Artificial intelligence utilization for article writing
ChatGPT was exclusively used for English translation and language refinement of this manuscript. All content was checked, revised, and approved by the authors, who take full responsibility for the accuracy and integrity of the final work.
Acknowledgment
The research protocol was approved and supported by the Student Research Committee, Tabriz University of Medical Sciences, Tabriz, Iran (Registration code: 75229).
Conflict of interest statement
The authors declare no conflict of interest.
Author contributions
HJ and SA conceptualized and designed the study; SA collected and curated data; AF performed the study and visualization; all authors added to writing, reviewing, editing, and validation, with HJ supervising.
Funding
This study was funded by the Tabriz University of Medical Sciences (Grant ID: 75229).
Data availability statement
The datasets created and analyzed during the current study are available from the corresponding author upon reasonable request.
Background & Objective: The aging population and the rising prevalence of chronic diseases have made palliative care a necessity for improving individuals' quality of life. Many healthcare professionals do not possess enough training and knowledge in this regard. The objective of this study was to check the attitudes and knowledge of internal medicine residents regarding palliative care.
Materials & Methods: A cross-sectional study was performed to check the knowledge and attitudes of internal medicine residents (n = 91). A validated, structured online questionnaire was used to check demographic characteristics, palliative care knowledge (30 items), and attitudes (37 items) across four domains. The data study was done using SPSS version 24, using both descriptive and inferential statistical methods, including t-tests, ANOVA, and multiple linear regression.
Results: The mean knowledge score was 19.66 ± 2.93, and the mean attitudes score was 139.47 ± 11.44). Prior training (p = 0.041) and male gender (p = 0.009) showed a significant correlation with higher attitude scores. Knowledge scores had a positive correlation with year of residency (p = 0.033) and a negative correlation with age (p = 0.004). Despite limited knowledge, 67% of participants stated that they needed training on palliative care.
Conclusion: Despite favorable attitudes toward palliative care, the lack of knowledge, particularly in conceptual and psychological domains, should be addressed. The findings highlight the necessity of palliative care training in internal medicine residency programs.
Introduction
The growing elderly population and the rising prevalence of chronic diseases have made palliative care an important part of modern healthcare [1]. According to the World Health Organization (WHO), palliative care is a holistic way to improve the quality of life for patients and their families by addressing physical, emotional, social, and spiritual distress [2-4]. It supports working together decision-making and proactive care planning, particularly in end-of-life scenarios where complex ethical dilemmas often occur [5].
The worldwide demand for palliative care is escalating. The WHO estimates that more than 50 million people around the world need palliative care annually, yet only about 14% receive it. About 78% of those in need live in low- and middle-income countries, where access to these services is still limited [6]. The epidemiologic transition toward non-communicable diseases and longer life expectancies in many countries has intensified this need [7]. In Iran, the increasing prevalence of chronic conditions such as cancer, cardiovascular diseases, and diabetes places a large burden on patients, their families, and the healthcare system [8].
Despite its importance, several obstacles hinder the growth and integration of palliative care within healthcare systems [9]. These challenges include a lack of awareness among healthcare providers and the general public, restricted access to specialized palliative care services, especially in rural or underserved regions, and a lack of trained professionals, including physicians, nurses, social workers, and psychologists with expertise in this field [10-12].
Furthermore, the absence of formal palliative care education in medical curricula adds to a competency gap among healthcare providers [13-15]. Due to their direct involvement in the management of complex and terminally ill patients, internal medicine residents represent a particularly important group in this context [16].
As frontline caregivers, they need not only clinical expertise but also proficiency in communication, ethical reasoning, and compassionate care delivery.
Checking their preparedness to deliver high-quality palliative care is needed to guide future educational reforms and policy decisions to support social accountability [17].
Previous studies in Iran have shown that healthcare providers have limited knowledge of palliative care and often feel underprepared to manage patients with advanced illnesses [13, 18].
A review of the current status of palliative care in Iran by Baraste et al. highlighted the need for formal education in this field [18]. In a descriptive–comparative study, Ebadi Nejad et al. identified physician education as one of the most significant needs in palliative care [19]. Another study reported that physicians themselves acknowledged their limited knowledge in this field [20]. Similarly, a descriptive cross-sectional study showed that both nurses and physicians in Iran have only moderate levels of knowledge and attitudes toward palliative care [13].
Sadigh et al. found that none of the emergency medicine residents in the study had prior formal training in palliative care [21].
Similarly, Hashemi et al. looked into the knowledge, attitudes, and practices of resident physicians concerning pain management in cancer patients, concluding that improving the educational curriculum and its application in clinical settings is crucial for improving patient outcomes [22]. Given their pivotal role in patient management, particularly for older individuals or patients with terminal diseases, internal medicine residents represent a key group whose knowledge and attitudes toward palliative care can significantly affect the quality of care provided [16].
Checking their current level of knowledge and attitudes is needed to identify deficiencies and make necessary modifications to residency training programs.
However, to date, no study has specifically looked for this topic among internal medicine residents in Iran.
Accordingly, this study aims to check the knowledge and attitudes of internal medicine residents at Tabriz University of Medical Sciences regarding palliative care.
Materials & Methods
Design and setting(s)
This study was done from 22 September 2024 to 10 September 2025, and used a cross-sectional web-based survey design to check the knowledge and attitudes of internal medicine residents toward palliative care at Tabriz University of Medical Sciences.
The study adhered to the Checklist for Reporting Results of Internet E-Surveys (CHERRIES) guidelines to ensure complete and transparent reporting [23].
Participants and sampling
Sampling was done through a census method, and all 116 internal medicine residents at Tabriz University of Medical Sciences were invited to take part. The inclusion rules for the study were internal medicine resident students enrolled, and the exclusion criterion was unwillingness to take part in the study.
Tools/Instruments
A structured, validated online questionnaire was used to collect data.
The instrument comprised three parts:
Demographic and professional background includes age, gender, marital status, residency year, work experience, palliative care work experience, workshop taking part, formal training, and need for training.
Health Care Providers' Knowledge of Palliative Care Questionnaire is a 30-item questionnaire covering four domains: general palliative concepts, pain management, physical symptom management, and psychological symptom management.
Each correct answer was awarded one point, and total scores ranged from 0 to 30.
Eleven items were reverse-scored to control for response bias.
Health Care Providers' Attitudes of Palliative Care Questionnaire is a 37-item questionnaire structured across four subdomains: core principles, patient autonomy, end-of-life care, and family involvement. Items were rated on a 5-point Likert scale (1 = strongly disagree to 5 = strongly agree). Nine items were reverse-scored. The total score ranged from 37 to 185.
The knowledge and attitudes questionnaires were designed and psychometrically checked by Ashrafizadeh et al. In 2022 in Iran [15].
They reported that the Cronbach's alpha of the whole tool was α = 0.75, and its dimensions were 0.70 to 0.83. In our study, the reliability of the questionnaire was determined by using the test–retest method after doing a pilot study on 20 internal medicine resident students. and its internal consistency was assessed with Cronbach's alpha coefficient.
For the knowledge questionnaire on palliative care among health care providers, the ICC was 0.83 (95% CI: 0.79–0.87), and Cronbach's alpha was 0.81. For the attitude questionnaire, the ICC was 0.81 (95% CI: 0.76–0.84), and Cronbach's alpha was 0.85.
Data collection methods
Data were collected using a questionnaire that was designed in Google Forms. The survey link was shared with internal medicine residents through official Telegram and WhatsApp groups. Two reminder messages were sent at two-week intervals. Taking part was voluntary, and residents were told that their responses would remain confidential and be used only for research purposes.
Data analysis
Data were analyzed using SPSS version 24. Continuous variables were described using mean ± standard deviation along with their range (minimum-maximum), and categorical variables were reported as frequencies and percentages.
The normality of the data was checked using the Shapiro–Wilk test. Independent t-tests and one-way ANOVA were used to check associations between demographic/professional variables and palliative care knowledge and attitude scores. Post-hoc study was performed using Tukey's test. Multiple Linear regression study using the Enter method was used to identify predictors of knowledge and attitude. Statistical significance was set at p < 0.05.
Results
Response rate was 78.45% and a total of 91 participants were included in the final study. The mean age of participants was 32.57 ± 5.61 years, ranging from 26 to 50 years, with most residents (53.8%) falling within the 30–39 age group. The majority were female (67%) and married (56%). First- and third-year residents each comprised about 29% of the sample. Only 10% of participants reported no work experience before residency, with the total range of experience spanning 0 to 28 years.
Most participants (87.9%) had no prior work experience in palliative care, and 72.5% had not taken part in relevant workshops. Nonetheless, 67% expressed a need for additional training.
The Shapiro–Wilk test confirmed the normal distribution of both knowledge (p = 0.071) and attitude (p = 0.164) scores toward palliative care. Statistical study revealed that both gender and prior participation in palliative care workshops were significantly associated with attitude scores.
Male participants had higher mean attitude scores than females (143.90 vs. 137.30, p = 0.009). Similarly, participants with workshop experience had higher attitude scores than those without (143.44 vs. 137.97, p = 0.041). No statistically significant associations were found between these variables and knowledge scores, except for age group (p = 0.047) and work experience (p = 0.017), which showed significant associations with knowledge scores (Table 1).
The data study showed that the mean ± SD of the total attitude and knowledge scores toward palliative care was 139.47 ± 11.44 and 19.66 ± 2.93, respectively (Table 2).
Multiple linear regression study in model 1 showed that 10.1% of the variance in attitude scores was explained by variables including age, year of training, gender, marital status, workshop attendance, formal training, perception of training need, and prior experience (R=0.437, R2= 0.191, R²adj = 0.101, F= 2.128, p = 0.036). Among these, gender emerged as the only statistically significant predictor.
Male gender was associated with significantly higher attitude scores (β = -0.331, 95% CI: -13.236 to -2.769, p = 0.003).
Similarly, in Model 2, 14.7% of the variance in knowledge scores was handled by the same set of predictors (R=0.482, R2= 0.232, R²adj = 0.147, F=2.720, p = 0.008). Age and training year were significantly associated with knowledge scores.
Specifically, age had the strongest negative predictive effect (β = -0.463, 95% CI: -3.389 to -0.660, p = 0.004), showing that for every one standard deviation increase in age, knowledge scores decreased by 0.463 standard deviations.
The academic year was also positively associated with knowledge (p = 0.033) (Table 3)
The worldwide demand for palliative care is escalating. The WHO estimates that more than 50 million people around the world need palliative care annually, yet only about 14% receive it. About 78% of those in need live in low- and middle-income countries, where access to these services is still limited [6]. The epidemiologic transition toward non-communicable diseases and longer life expectancies in many countries has intensified this need [7]. In Iran, the increasing prevalence of chronic conditions such as cancer, cardiovascular diseases, and diabetes places a large burden on patients, their families, and the healthcare system [8].
Despite its importance, several obstacles hinder the growth and integration of palliative care within healthcare systems [9]. These challenges include a lack of awareness among healthcare providers and the general public, restricted access to specialized palliative care services, especially in rural or underserved regions, and a lack of trained professionals, including physicians, nurses, social workers, and psychologists with expertise in this field [10-12].
Furthermore, the absence of formal palliative care education in medical curricula adds to a competency gap among healthcare providers [13-15]. Due to their direct involvement in the management of complex and terminally ill patients, internal medicine residents represent a particularly important group in this context [16].
As frontline caregivers, they need not only clinical expertise but also proficiency in communication, ethical reasoning, and compassionate care delivery.
Checking their preparedness to deliver high-quality palliative care is needed to guide future educational reforms and policy decisions to support social accountability [17].
Previous studies in Iran have shown that healthcare providers have limited knowledge of palliative care and often feel underprepared to manage patients with advanced illnesses [13, 18].
A review of the current status of palliative care in Iran by Baraste et al. highlighted the need for formal education in this field [18]. In a descriptive–comparative study, Ebadi Nejad et al. identified physician education as one of the most significant needs in palliative care [19]. Another study reported that physicians themselves acknowledged their limited knowledge in this field [20]. Similarly, a descriptive cross-sectional study showed that both nurses and physicians in Iran have only moderate levels of knowledge and attitudes toward palliative care [13].
Sadigh et al. found that none of the emergency medicine residents in the study had prior formal training in palliative care [21].
Similarly, Hashemi et al. looked into the knowledge, attitudes, and practices of resident physicians concerning pain management in cancer patients, concluding that improving the educational curriculum and its application in clinical settings is crucial for improving patient outcomes [22]. Given their pivotal role in patient management, particularly for older individuals or patients with terminal diseases, internal medicine residents represent a key group whose knowledge and attitudes toward palliative care can significantly affect the quality of care provided [16].
Checking their current level of knowledge and attitudes is needed to identify deficiencies and make necessary modifications to residency training programs.
However, to date, no study has specifically looked for this topic among internal medicine residents in Iran.
Accordingly, this study aims to check the knowledge and attitudes of internal medicine residents at Tabriz University of Medical Sciences regarding palliative care.
Materials & Methods
Design and setting(s)
This study was done from 22 September 2024 to 10 September 2025, and used a cross-sectional web-based survey design to check the knowledge and attitudes of internal medicine residents toward palliative care at Tabriz University of Medical Sciences.
The study adhered to the Checklist for Reporting Results of Internet E-Surveys (CHERRIES) guidelines to ensure complete and transparent reporting [23].
Participants and sampling
Sampling was done through a census method, and all 116 internal medicine residents at Tabriz University of Medical Sciences were invited to take part. The inclusion rules for the study were internal medicine resident students enrolled, and the exclusion criterion was unwillingness to take part in the study.
Tools/Instruments
A structured, validated online questionnaire was used to collect data.
The instrument comprised three parts:
Demographic and professional background includes age, gender, marital status, residency year, work experience, palliative care work experience, workshop taking part, formal training, and need for training.
Health Care Providers' Knowledge of Palliative Care Questionnaire is a 30-item questionnaire covering four domains: general palliative concepts, pain management, physical symptom management, and psychological symptom management.
Each correct answer was awarded one point, and total scores ranged from 0 to 30.
Eleven items were reverse-scored to control for response bias.
Health Care Providers' Attitudes of Palliative Care Questionnaire is a 37-item questionnaire structured across four subdomains: core principles, patient autonomy, end-of-life care, and family involvement. Items were rated on a 5-point Likert scale (1 = strongly disagree to 5 = strongly agree). Nine items were reverse-scored. The total score ranged from 37 to 185.
The knowledge and attitudes questionnaires were designed and psychometrically checked by Ashrafizadeh et al. In 2022 in Iran [15].
They reported that the Cronbach's alpha of the whole tool was α = 0.75, and its dimensions were 0.70 to 0.83. In our study, the reliability of the questionnaire was determined by using the test–retest method after doing a pilot study on 20 internal medicine resident students. and its internal consistency was assessed with Cronbach's alpha coefficient.
For the knowledge questionnaire on palliative care among health care providers, the ICC was 0.83 (95% CI: 0.79–0.87), and Cronbach's alpha was 0.81. For the attitude questionnaire, the ICC was 0.81 (95% CI: 0.76–0.84), and Cronbach's alpha was 0.85.
Data collection methods
Data were collected using a questionnaire that was designed in Google Forms. The survey link was shared with internal medicine residents through official Telegram and WhatsApp groups. Two reminder messages were sent at two-week intervals. Taking part was voluntary, and residents were told that their responses would remain confidential and be used only for research purposes.
Data analysis
Data were analyzed using SPSS version 24. Continuous variables were described using mean ± standard deviation along with their range (minimum-maximum), and categorical variables were reported as frequencies and percentages.
The normality of the data was checked using the Shapiro–Wilk test. Independent t-tests and one-way ANOVA were used to check associations between demographic/professional variables and palliative care knowledge and attitude scores. Post-hoc study was performed using Tukey's test. Multiple Linear regression study using the Enter method was used to identify predictors of knowledge and attitude. Statistical significance was set at p < 0.05.
Results
Response rate was 78.45% and a total of 91 participants were included in the final study. The mean age of participants was 32.57 ± 5.61 years, ranging from 26 to 50 years, with most residents (53.8%) falling within the 30–39 age group. The majority were female (67%) and married (56%). First- and third-year residents each comprised about 29% of the sample. Only 10% of participants reported no work experience before residency, with the total range of experience spanning 0 to 28 years.
Most participants (87.9%) had no prior work experience in palliative care, and 72.5% had not taken part in relevant workshops. Nonetheless, 67% expressed a need for additional training.
The Shapiro–Wilk test confirmed the normal distribution of both knowledge (p = 0.071) and attitude (p = 0.164) scores toward palliative care. Statistical study revealed that both gender and prior participation in palliative care workshops were significantly associated with attitude scores.
Male participants had higher mean attitude scores than females (143.90 vs. 137.30, p = 0.009). Similarly, participants with workshop experience had higher attitude scores than those without (143.44 vs. 137.97, p = 0.041). No statistically significant associations were found between these variables and knowledge scores, except for age group (p = 0.047) and work experience (p = 0.017), which showed significant associations with knowledge scores (Table 1).
The data study showed that the mean ± SD of the total attitude and knowledge scores toward palliative care was 139.47 ± 11.44 and 19.66 ± 2.93, respectively (Table 2).
Multiple linear regression study in model 1 showed that 10.1% of the variance in attitude scores was explained by variables including age, year of training, gender, marital status, workshop attendance, formal training, perception of training need, and prior experience (R=0.437, R2= 0.191, R²adj = 0.101, F= 2.128, p = 0.036). Among these, gender emerged as the only statistically significant predictor.
Male gender was associated with significantly higher attitude scores (β = -0.331, 95% CI: -13.236 to -2.769, p = 0.003).
Similarly, in Model 2, 14.7% of the variance in knowledge scores was handled by the same set of predictors (R=0.482, R2= 0.232, R²adj = 0.147, F=2.720, p = 0.008). Age and training year were significantly associated with knowledge scores.
Specifically, age had the strongest negative predictive effect (β = -0.463, 95% CI: -3.389 to -0.660, p = 0.004), showing that for every one standard deviation increase in age, knowledge scores decreased by 0.463 standard deviations.
The academic year was also positively associated with knowledge (p = 0.033) (Table 3)
Table 1. Comparison of attitude and knowledge scores according to demographic and educational characteristics (n = 91)
Note: Values are presented as Mean ± SD for continuous variables and n (%) for categorical variables. Independent-samples t-test and one-way ANOVA were used for
group comparisons. A p-value < 0.05 was considered statistically significant.
Abbreviations: n, number of participants; SD, standard deviation; Sig., significance; p, probability-value.
Table 2. Distribution of attitude and knowledge subscale scores
Note: Values are presented as Mean ± SD with watched minimum and maximum scores. Higher scores show more positive attitudes or greater knowledge regarding palliative care.
Abbreviations: SD, standard deviation.
Table 3. Predictors of attitude and knowledge scores: multiple linear regression analysis
Note: A Multiple linear regression study was performed to check predictors of palliative care attitudes and knowledge. Model 1 included demographic and experiential variables, while Model 2 additionally considered educational factors. A p-value < 0.05 was considered statistically significant.
Abbreviations: B, unstandardized regression coefficient; S.E., standard error; β, standardized regression coefficient; CI, confidence interval; R, correlation coefficient; R², coefficient of determination; R² adj, adjusted coefficient of determination; F, F-test statistic; p, probability value.
Abbreviations: B, unstandardized regression coefficient; S.E., standard error; β, standardized regression coefficient; CI, confidence interval; R, correlation coefficient; R², coefficient of determination; R² adj, adjusted coefficient of determination; F, F-test statistic; p, probability value.
Discussion
This study checked the understanding and perspectives of internal medicine residents regarding palliative care at Tabriz University of Medical Sciences, and provided valuable insights into the cognitive and affective dimensions of end-of-life care within Iran's postgraduate medical education and residency programs. The findings revealed a moderate level of knowledge and a generally positive attitude toward palliative care, though significant variations were observed among different demographic and professional subgroups.
The mean knowledge score (19.66 ± 2.93 out of 30) showed limited proficiency, especially in basic concepts of palliative care (3.04 ± 1.14), which is consistent with global literature reporting suboptimal palliative care literacy among medical trainees [24-26]. Low scores in the domains of psychological symptom management and general concepts suggest a significant gap in understanding the holistic nature of palliative care. This finding aligns with other studies showing that medical education often puts first pharmacological management, and underemphasizes topics such as grief, existential suffering, and interdisciplinary teamwork [27]. Similarly, a study among pediatric residents and fellows has shown not enough preparation in core aspects of palliative care, particularly in communication skills and pain management [28]. Despite their knowledge limitations, residents displayed generally positive attitudes, with a mean score of 139.47 ± 11.44 (out of 185). The highest attitudinal responses were observed in
the domain of basic principles. This finding shows deep ethical attention among residents toward patient-focused values such as respect, dignity, and compassion. However, lower scores in end-of-life decision-making and family engagement suggest discomfort or not training in managing the sophisticated psychosocial aspects of patient care. Previous studies also showed that medical trainees feel more confident in the theoretical and technical aspects of patient care than in communication and interpersonal relations [27, 29, 30]. Similarly, a study among pediatric residents reported minimal training, knowledge, and confidence across nearly all palliative care domains, with strong demand for further education in pain management and communication skills [31].
Further study through multiple regression revealed the key predictors of knowledge and attitudes. Gender was a significant predictor of knowledge and attitudes toward palliative care. Interestingly, male residents showed more positive attitudes than their female peers. This observation contrasts with previous studies, where female healthcare professionals showed greater empathy and openness to the principles of palliative care [13, 32].
This inconsistency may be a result of contextual factors such as cultural norms, institutional roles, or differences in clinical experiences.
Furthermore, results showed that taking part in palliative care workshops was associated with higher attitude scores; however, it had little impact on knowledge levels.
This finding suggests that short-term educational interventions may improve affective learning but are not enough to create deep cognitive learning without long-term reinforcement [33, 34].
The relationship between age, prior clinical experience, and knowledge was intricate and non-linear. Older residents generally scored lower on knowledge, whereas the highest knowledge levels were seen in residents with 4–6 years of prior experience, suggesting an optimal experience window as an "experience sweet spot" where prior exposure may improve learning receptivity. These findings align with Bloom's taxonomy, which tells apart affective learning from cognitive growth. It emphasizes that deeper competencies are best built through longitudinal, experiential approaches such as clinical rotations, mentorship, and reflective practice [35].
Notably, only 9.9% of residents had received formal education in palliative care, and only 12.1% reported prior work experience in this field. However, 67% of the residents expressed a strong interest in further training in palliative care. This highlights a systemic gap in educational opportunities, showing the World Health Organization's call to add palliative care into all levels of medical education to help universal health coverage [2]. In Iran, the growth of palliative care services must be accompanied by training competent professionals [36]. In the end, these findings highlight the urgent need for curricular reform in postgraduate medical education. Internal medicine residency programs should add structured, longitudinal palliative care training that goes beyond mere knowledge transfer and fosters ethical decision-making, interdisciplinary teamwork, and compassionate clinical communication.
This study has several limitations. First, because of its design, causal relationships cannot be confidently created. Second, the study included residents from only one university with a relatively small sample size. Thus, the generalizability of the findings is limited. Despite necessary measures to make it easier for participants virtual take part virtually, the sampling method and the procedure for questionnaire completion added further limitations.
Conclusion
In conclusion, internal medicine residents at Tabriz University of Medical Sciences showed positive attitudes toward palliative care; however, large knowledge gaps existed, particularly in foundational concepts and psychosocial domains. Structured, longitudinal, and evidence-based educational interventions are needed to improve competencies regarding palliative care delivery and fulfill the social accountability of Iran's medical education system.
Ethical considerations
This study was approved by the Research Ethics Committee of Tabriz University of Medical Sciences with the code IR.TBZMED.REC.1403.633.
Artificial intelligence utilization for article writing
ChatGPT was exclusively used for English translation and language refinement of this manuscript. All content was checked, revised, and approved by the authors, who take full responsibility for the accuracy and integrity of the final work.
Acknowledgment
The research protocol was approved and supported by the Student Research Committee, Tabriz University of Medical Sciences, Tabriz, Iran (Registration code: 75229).
Conflict of interest statement
The authors declare no conflict of interest.
Author contributions
HJ and SA conceptualized and designed the study; SA collected and curated data; AF performed the study and visualization; all authors added to writing, reviewing, editing, and validation, with HJ supervising.
Funding
This study was funded by the Tabriz University of Medical Sciences (Grant ID: 75229).
Data availability statement
The datasets created and analyzed during the current study are available from the corresponding author upon reasonable request.
Article Type : Orginal Research |
Subject:
Medical Education
Received: 2025/07/14 | Accepted: 2025/10/20 | Published: 2025/11/19
Received: 2025/07/14 | Accepted: 2025/10/20 | Published: 2025/11/19
References
1. Chan KS. Palliative care: the need of the modern era. Hong Kong Med J. 2018;24(4):391-9. [DOI:10.12809/hkmj187310] [PMID]
2. World Health Organization. Planning and implementing palliative care services: a guide for programme managers [Internet]. Geneva: WHO; 2016. [cited 2025 Aug 3]. Available from:
3. Odukwe F, Ezeh F. What is palliative care? InnovAiT. 2021;14(1):19-26. [DOI:10.1177/1755738020966780]
4. Abrahm JL. Update in palliative medicine and end-of-life care. Annu Rev Med. 2003;54(1):53-72. [DOI:10.1146/annurev.med.54.101601.152218] [PMID]
5. Alanazi MA, Shaban MM, Ramadan OE, Alzahrani A, Alshehri A, Alotaibi M, et al. Navigating end-of-life decision-making in nursing: a systematic review of ethical challenges and palliative care practices. BMC Nurs. 2024;23(1):467. [DOI:10.1186/s12912-024-02087-5] [PMID] []
6. World Health Organization. Palliative care [Internet]. Geneva: WHO; 2020. [cited 2025 Aug 3]. Available from:
7. Lu Y, Gu Y, Yu W. Hospice and palliative care in China: development and challenges. Asia Pac J Oncol Nurs. 2018;5(1):26-32. [DOI:10.4103/apjon.apjon_72_17] [PMID] []
8. Naghavi M, Shahraz S, Sepanlou SG, Dicker D, Naghavi P, Pourmalek F, et al. Health transition in Iran toward chronic diseases based on results of Global Burden of Disease 2010. Arch Iran Med. 2014;17(5):321-35.
9. Amroud MS, Raeissi P, Hashemi SM, Reisi N, Ahmadi SA. Investigating the challenges and barriers of palliative care delivery in Iran and the world: a systematic review study. J Educ Health Promot. 2021;10:246. [DOI:10.4103/jehp.jehp_1325_20] [PMID] []
10. Ansari M, Rassouli M, Akbari ME, Abbaszadeh A, Akbari Sari A. Process challenges in palliative care for cancer patients: a qualitative study. Middle East J Cancer. 2019;10(1):43-53.
11. Azami-Aghdash S, Jabbari H, Bakhshian F, Mohammadzadeh N, Mohseni M. Attitudes and knowledge of Iranian nurses about hospice care. Indian J Palliat Care. 2015;21(2):209-13. [DOI:10.4103/0973-1075.156505] [PMID] []
12. Banazadeh M, Azizzadeh Foroozy M, Iranmanesh S. Assessment of barriers in providing end of life care to terminally ill pediatric patients from the perspective of nursing staff. J Pediatr Nurs. 2015;1(2):74.
13. Khanali-Mojen L, Akbari ME, Ashrafizadeh H, Rassouli M, Sari AA. Caregivers' knowledge of and attitude towards palliative care in Iran. Asian Pac J Cancer Prev. 2022;23(11):3743-51. [DOI:10.31557/APJCP.2022.23.11.3743] [PMID] []
14. Aghaei MH, Mohajjel Aghdam A, Bodaghi S, Azami Agdash S. Knowledge and attitude of nurses toward caring for end of life patients. Iran J Nurs. 2017;30(107):74-82. [DOI:10.29252/ijn.30.107.74]
15. Ashrafizadeh H, Mojen L, Barasteh S, Rassouli M, Tabatabaee A. Factors related to nurses and physicians' knowledge and attitudes towards palliative care. Int J Cancer Manag. 2022;15(2):e122653. [DOI:10.5812/ijcm-122653]
16. Kawaguchi S, Mirza R, Nissim R, Ridley J. Internal medicine residents' beliefs, attitudes, and experiences relating to palliative care: a qualitative study. Am J Hosp Palliat Care. 2017;34(4):366-72. [DOI:10.1177/1049909116628799] [PMID]
17. Frydman JL, Hauck K, Lowy J, Gelfman LP. Improving the care of patients with serious illness: what are the palliative care education needs of internal medicine residents? Am J Hosp Palliat Care. 2021;38(10):1218-24. [DOI:10.1177/1049909120987207] [PMID] []
18. Barasteh S, Rassouli M, Parandeh A, Ebadi A, Vahedian-Azimi A, Zaboli R, et al. Palliative care in the health system of Iran: a review of the present status and the future challenges. Asian Pac J Cancer Prev. 2020;21(3):845-51. [DOI:10.31557/APJCP.2020.21.3.845] [PMID] []
19. Ebadinejad Z, Rassouli M, Fakhr-Movahedi A. Assessing the compliance of educational curricula of selected disciplines with the content standards of cancer-related palliative care. J Educ Health Promot. 2021;10:247. [DOI:10.4103/jehp.jehp_1415_20] [PMID] []
20. Jabbari H, Piri R, Bakhshian F, Mohammadzadeh N, Mohseni M. End-of-life care: beliefs, attitudes, and experiences of Iranian physicians. Indian J Palliat Care. 2018;24(4):431-5. [DOI:10.4103/IJPC.IJPC_74_18] [PMID] []
21. Sadigh N, Seyedhosseini J, Tahmasebi M, Shirani F. Attitude toward end-of-life care in emergency medicine residents-can a short workshop make a difference? PLoS One. 2023;18(1):e0280229. [DOI:10.1371/journal.pone.0280229] [PMID] []
22. Hashemi M, Akbari ME, Razavi SS, Saadat-Niaki A, Hoseini Khameneh SM. Evaluating resident physicians' knowledge, attitude, and practice regarding the pain control in cancer patients. Iran J Cancer Prev. 2015;8(1):1-10.
23. Eysenbach G. Improving the quality of Web surveys: the Checklist for Reporting Results of Internet E-Surveys (CHERRIES). J Med Internet Res. 2004;6(3):e34. [DOI:10.2196/jmir.6.3.e34] [PMID] []
24. Al-Drees O, AlHubail M, Elzubair AG. Palliative care: knowledge and attitude among Saudi residents, 2016. J Palliat Med. 2019;22(11):1401-9. [DOI:10.1089/jpm.2018.0437] [PMID]
25. Eyigor S. Fifth-year medical students' knowledge of palliative care and their views on the subject. J Palliat Med. 2013;16(8):941-6. [DOI:10.1089/jpm.2012.0627] [PMID]
26. Fernando GVMC, Prathapan S. What do young doctors know of palliative care; how do they expect the concept to work? BMC Res Notes. 2019;12(1):419. [DOI:10.1186/s13104-019-4462-2] [PMID] []
27. Pieters J, Dolmans D, Verstegen DML, Warmenhoven FC, Courtens AM, van den Beuken-van Everdingen MHJ. Palliative care education in the undergraduate medical curricula: students' views on the importance of, their confidence in, and knowledge of palliative care. BMC Palliat Care. 2019;18(1):72. [DOI:10.1186/s12904-019-0458-x] [PMID] []
28. Michelson KN, Ryan AD, Jovanovic B, Frader J. Pediatric residents' and fellows' perspectives on palliative care education. J Palliat Med. 2009;12(5):451-7. [DOI:10.1089/jpm.2008.0263] [PMID] []
29. Budkaew J, Chumworathayi B. Knowledge and attitudes toward palliative terminal cancer care among Thai generalists. Asian Pac J Cancer Prev. 2013;14(10):6173-80. [DOI:10.7314/APJCP.2013.14.10.6173] [PMID]
30. Tait V, Higgs M, Magann L, Dixon J, Davis JM, Fernandez R. Attitudes of nonpalliative care nurses towards palliative care. Int J Palliat Care. 2015;2015:469174. [DOI:10.1155/2015/469174]
31. Kolarik RC, Walker G, Arnold RM. Pediatric resident education in palliative care: a needs assessment. Pediatrics. 2006;117(6):1949-54. [DOI:10.1542/peds.2005-1111] [PMID]
32. Younis WY, Hamdan-Mansour AM. Status and predictors of medical students' knowledge and attitude towards palliative care in Jordan: a cross-sectional study. BMC Palliat Care. 2024;23(1):9. [DOI:10.1186/s12904-023-01338-7] [PMID] []
33. Gerhardt CA, Grollman JA, Baughcum AE, Young-Saleme T, Stefanik R, Klopfenstein KJ. Longitudinal evaluation of a pediatric palliative care educational workshop for oncology fellows. J Palliat Med. 2009;12(4):323-8. [DOI:10.1089/jpm.2008.0285] [PMID]
34. Pulsford D, Jackson G, O'Brien T, Yates S, Duxbury J. Classroom-based and distance learning education and training courses in end-of-life care for health and social care staff: a systematic review. Palliat Med. 2013;27(3):221-35. [DOI:10.1177/0269216311429496] [PMID]
35. Cannon HM, Feinstein AH. Bloom beyond bloom: using the revised taxonomy to develop experiential learning strategies. Dev Bus Simul Experiential Learn. 2005;32:348-56. [cited 2025 Aug 3]. Available from:
36. Barasteh S, Parandeh A, Rassouli M, Ebadi A, Vahedian-Azimi A, Zaboli R, et al. Integration of palliative care into the primary health care of Iran: a document analysis. Middle East J Cancer. 2021;12(2):292-300.
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
