
Sat, Jul 11, 2026
[Archive]
Volume 19, Issue 1 (2026)
J Med Edu Dev 2026, 19(1): 12-19 |
Back to browse issues page
Ethics code: 2024/35
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Zengin A, Ulfanov O, Bag Y M, Angin Y S, Ulas M. Effectiveness of video-assisted vs. face-to-face learning in surgical knot-tying skills: a randomized controlled pilot study. J Med Edu Dev 2026; 19 (1) :12-19
URL: http://edujournal.zums.ac.ir/article-1-2496-en.html
URL: http://edujournal.zums.ac.ir/article-1-2496-en.html

1- Department of Gastrointestinal Surgery, Eskisehir Osmangazi University, Eskisehir, Turkey , dr.akile.zengin@gmail.com
2- Department of General Surgery, Eskisehir Osmangazi University, Eskisehir, Turkey
3- Department of General Surgery, Ankara Training and Research Hospital, Ankara, Turkey
4- Department of Gastrointestinal Surgery, Eskisehir Osmangazi University, Eskisehir, Turkey
2- Department of General Surgery, Eskisehir Osmangazi University, Eskisehir, Turkey
3- Department of General Surgery, Ankara Training and Research Hospital, Ankara, Turkey
4- Department of Gastrointestinal Surgery, Eskisehir Osmangazi University, Eskisehir, Turkey
Keywords: surgical education, knot-tying, face-to-face learning, video-assisted learning, medical students, psychomotor skills
Full-Text [PDF 658 kb]
(193 Downloads)
| Abstract (HTML) (653 Views)
Full-Text: (51 Views)
Abstract
Background & Objective: In contemporary medical education, the shortage of instructors for basic skills training has led to a growing shift toward alternative instructional methods, among which video-based training is a notable approach. This study compared the results of Face-to-Face Learning (FtFL) and Video-Assisted Learning (VAssL) in the acquisition of surgical skills by medical students.
Materials & Methods: Our study was a prospective, single-blinded, randomized controlled pilot trial. 32 medical students were randomly allocated 1:1 to FtFL (n = 16) or VAssL (n = 16) using computer-generated random numbers and sealed opaque envelopes to ensure allocation concealment. The primary outcome was knot-setting success. Secondary outcomes included hand movement proficiency and the number of knots tied per minute. All assessments were performed using a structured scoring table by two blinded assessors.
Results: The mean number of knots tied per minute was 10.97 ± 4.13, and the median knot score was 4 (3–5), with no significant difference between groups (p = 0.476, p = 0.306, respectively). Over 90% of participants succeeded in hand movements, except for knot setting, which had a 65.6% success rate overall. The FtFL group showed significantly higher success in knot setting compared to the VAssL group (93.8% vs. 37.5%, p = 0.002, Cohen’s d = 1.60) and superior hand movement proficiency (median 5 )5–5(vs. 4 )4–5(, p = 0.001).
Conclusion: Face-to-face learning is more beneficial than video-assisted learning for correcting deficiencies and mistakes in medical students' acquisition of surgical skills.
Introduction
Surgical education has experienced a profound evolution in recent years, largely influenced by the growing focus on patient safety and outcomes-based competency training [1]. As a result, contemporary medical curricula increasingly emphasize the development of core psychomotor abilities before students are introduced to real clinical environments [2]. Among the fundamental manual skills, various surgical knots—such as the square knot, surgeon’s knot, and slip knot—are widely used to ligate vessels, secure tissues, and ensure wound stability [3]. Proper knot-tying offers critical benefits, including reliable wound closure, reduced risk of slippage, and improved procedural safety [4]. In general surgery, manual knot-tying is frequently preferred over instrument-assisted approaches, as it provides surgeons with enhanced tactile feedback and greater control over suture tension, thereby improving knot reliability. The square knot—recognized as the standard configuration—comprises consecutive throws aligned parallel to one another [5]. Inadequate mastery of this essential technique may result in knot slippage or failure, potentially leading to intraoperative complications and compromising patient outcomes and satisfaction [4]. Traditional Face-to-Face Learning (FtFL), based on the
master-apprentice model, has been regarded as a standard teaching method for hands-on skills [6]. It provides learners with real-time feedback, immediate error correction, and instructor-guided repetition — all of which are essential for developing motor precision [7]. Yet, the growing number of medical students and the limited availability of surgical instructors have strained the sustainability of this model [8]. Meanwhile, advances in digital tools have paved the way for Video-Assisted Self-Directed Learning (VAssL), an increasingly popular method that enables flexible, repeatable, and accessible skill acquisition outside the traditional classroom [9]. In this context, VAssL is gaining increasing interest for its benefits, such as more efficient use of educational resources, improved accessibility, and the ability for learners to progress at their own pace. This approach offers greater flexibility, broader access to information, and the ability to complete coursework at a self-directed pace. Interaction with instructors is one of the distinctive advantages that make online learning appealing to many students [10]. Despite this, some argue that passive video training, lacking interactive feedback mechanisms, may be inadequate for teaching complex psychomotor skills such as surgery [11]. One of the most important advantages of face-to-face versus video-assisted is better skill acquisition. Previous research comparing face-to-face and video-based learning has shown that supervised instruction tends to yield better technical performance, while video-assisted methods provide comparable theoretical understanding but may fall short in manual precision. Educational programs designed to strengthen both theoretical understanding and practical ability are therefore indispensable in modern medical training [6,12]. Numerous studies indicate that many final-year medical students complete their training without achieving sufficient proficiency in these elementary technical tasks, revealing a persistent shortfall in undergraduate surgical education [13]. For centuries, surgical education has incorporated simulation-based training using animal models, cadavers, and various materials designed to mimic tissues and organs [14]. Enhancing students’ knowledge and skills through structured educational courses is essential [15]. In particular, carefully structured surgical skills courses—progressing from fundamental to advanced levels—provide a secure environment for experiential learning while ensuring that competence in essential techniques is achieved prior to graduation [16]. Surgical skills courses typically include modules such as suturing, knot-tying, instrument handling, tissue approximation, and basic laparoscopic tasks, enabling students to gradually develop psychomotor proficiency under standardized conditions [17]. Evidence suggests that structured skills training significantly enhances psychomotor competence, improves procedural confidence, and positively impacts subsequent clinical performance [18]. Surgical simulators provide a safe space where learners can experiment with procedures at their own pace, repeatedly refining their skills while learning from errors without pressure [19]. Notably, simulators are standardized, reproducible, measurable, precise, continuously accessible, and objective [20]. Basic surgical skills learned during medical education may make it easy to learn more advanced surgical techniques during surgical assistance [13]. Therefore, we argue that basic surgical skills should be taught to medical students. How this education should be delivered, and the effect of video-assisted/online education on this, are among the most popular issues today. The acceleration of digitalization in medical education has made the comparison of traditional and innovative teaching methods highly significant, as there are still regions in the world where the number of instructors is insufficient to meet the educational needs of medical students. In such contexts, new instructional models are needed to ensure equitable educational opportunities. However, despite the growing body of evidence, gaps remain in understanding the comparative effectiveness of face-to-face and video-assisted instruction, specifically in knot-tying performance, particularly among final-year medical students—a group expected to demonstrate clinical readiness. Clear evidence is still needed regarding which method better supports safe, standardized, and efficient acquisition of this essential skill. Therefore, this randomized controlled pilot study aims to compare the effectiveness of FtFL and VAssL methods in teaching surgical knot-tying to final-year medical students and to provide insights for optimizing future surgical training models.
Materials & Methods
Design and setting(s)
The study was experimental and conducted with final-year medical students who had not received any prior knot-tying education. Written informed consent was obtained from all participants prior to enrollment. The study was conducted between October 7, 2024, and October 14, 2024. The study was approved by the Eskisehir Osmangazi University Nonclinical Ethical Committee in accordance with the Declaration of Helsinki. The study was designed, conducted, and reported in accordance with the Consolidated Standards of Reporting Trials (CONSORT) 2010 guidelines. The completed CONSORT checklist is provided as Appendix 1.
Participants and sampling
This sample size calculation was performed using Minitab® Statistical Software version 16. The computation was based on values reported in the literature [21], assuming a mean difference of 15.68 between the two groups and a pooled standard deviation of 9.76. Using these parameters, the effect size (Cohen’s d) was calculated as 1.60, and the analyses revealed that, with a power of 99% (α = 0.05, 1-ß = 0.99), a total sample size of 32 (n1:16, n2:16) was needed. A total of 32 students were involved in the study (see Figure 1 for the CONSORT flow diagram). This pilot study was a randomized, single-blinded study. The randomization sequence was generated by an independent researcher using computer-generated random numbers. Allocation concealment was ensured through sequentially numbered, sealed, opaque envelopes prepared and stored by the same researcher. Immediately before the training, a second researcher—blinded to the randomization list—distributed the envelopes, and each participant opened their envelope to learn their assignment. In this way, students were allocated to the face-to-face group (n = 16) or the video group (n = 16). The assessors were fully blinded; evaluations were conducted individually using coded forms without group identifiers, and the allocation list was kept separately by an independent researcher. Both instructors rehearsed the knot-tying procedure prior to the study according to standardized steps and rules, and they cross-evaluated each other’s performance to ensure inter-rater reliability. Both groups received the same knot-tying instruction. In the FtFL group, two instructors (one gastrointestinal surgery specialist and one senior general surgery assistant) supervised 16 students for a single 60-minute session that included both teaching and hands-on practice. The VAssL group received an 87-second Turkish instructional video via WhatsApp, which they could watch, pause, and rewind as needed. Frequency and total viewing time were not monitored, so their effects on learning outcomes could not be assessed. The study flow is presented in Fig. 1. These procedures ensured consistent instruction and provided initial evidence of the training interventions' content validity and reliability.

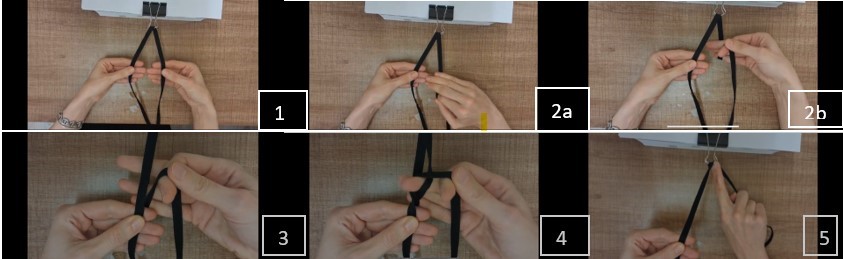
Figure 2. Visual depiction of the sequential steps for performing the square knot: (1) Correct initial grip of both rope ends, (2a, 2b) Formation of the first loop using a three-finger technique, (3) Transfer of the rope from the non-dominant to the dominant hand, (4) Execution of the cross‑tying maneuver, (5) Final knot setting and tightening.
Data collection methods
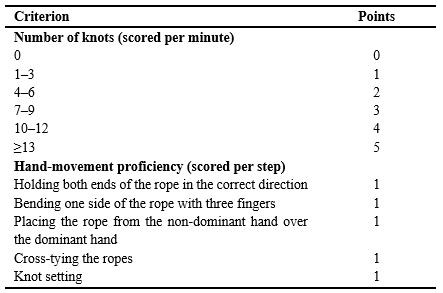
Researchers who were blinded to group assignment evaluated participants' knot-tying skills after one week of self‑practice. The researchers' unique scoring scale was used for evaluation. As a result of the validity and reliability analyses of this scale, the Cronbach’s α scale level was calculated as 0.8. The scale consists of two subcomponents: (1) Knot Score, ranging from 0 to 5 points based on the number of knots tied in one minute; (2) Hand Movement Proficiency Score, ranging from 0 to 5 points based on the correct execution of knot-tying steps (Table 1). The total score ranges from 0 to 10.
Participants who scored six or higher were considered "successful."
Table 1. Scoring system for knot‑tying performance assessment
Discussion
In our study, the most prominent finding was that participants in the FtFL group achieved more knots and demonstrated greater hand movement proficiency than those in the VAssL group. This result aligns with the expectation that direct instructor communication and real-time feedback enhance the acquisition of complex psychomotor skills. The absence of prior exposure to the alternative training method in both groups allowed us to more precisely observe the pure effect of each educational approach. These factors likely explain why the FtFL group outperformed the VAssL group.
A second key finding was the superior hand skill proficiency scores in the FtFL group, emphasizing the importance of instructor-provided feedback for mastering surgical knot-tying. Similarly, Tejos et al. [11]
found that traditional education was more effective than video-based learning in teaching basic surgical skills. They also reported that a video-guided learning approach without feedback is insufficient compared to expert or
peer feedback when developing an optimized teaching program for suturing skills. However, a limitation of that study was the potential difference in training and practice durations between the video-based and traditional groups, as the self-directed video group’s study time was not verified. The lack of precise data on students’ practice times in our study is a comparable limitation that may partly explain variations in performance. Another important observation is that face-to-face teaching continues to show advantages in performance-based clinical skills. In the study by Shen et al. [6], two groups completing a neurosurgery clerkship—one online and one face-to-face—were compared. Although no significant difference was found in theoretical knowledge, the face-to-face group performed better on clinical practice tasks, such as history-taking and physical examination. The authors concluded that while online teaching can serve as a valuable supplementary tool, it cannot fully replace face-to-face instruction in the development of clinical practical skills. Our findings are consistent with this view, as the VAssL group lacked immediate corrective feedback, which may have hindered their psychomotor learning. Contrary to studies supporting the necessity of feedback, in the study of Kumins [7] et al. in which knot-tying and suturing training was given online, they stated that the feedback provided by the trainers may not be considered necessary for learning. This difference is thought to be due to factors such as variations in practice duration and differences in the availability of individualized feedback. In a randomized study, no difference was found between the face-to-face and video-assisted education groups in terms of surgical skill improvement [9]. A systematic review found that video-assisted and traditional education did not differ in teaching basic surgical skills [8]. As a result of these studies, video-assisted education may be considered an alternative to face-to-face education. However, in this randomized controlled study, both groups received face-to-face training first, and then one group received video-assisted training; after that, the evaluation was made between the groups. The study by Raythatha et al. [22] was parallel to the previous one; both groups received face-to-face education, and only one group had the opportunity to receive video-assisted education. The results were better for the video-assisted group. Yet, those studies differed from ours because both groups first received face-to-face instruction before video reinforcement, making it difficult to isolate the true comparative effects of the methods. In our study, groups were trained exclusively with a single method, allowing us to directly compare their isolated effects, which may explain why FtFL demonstrated superiority in our study. A further finding of our analysis suggests that VAssL may be improved by refining instructional content. Providing videos with detailed explanations targeting commonly observed weaknesses could improve both hand movement proficiency and the number of knots tied. This may help narrow the performance gap between VAssL and FtFL methods. The limitations of this study include the fact that it was a pilot study conducted in a small study group. The total time that the students practiced knot-tying on their own and the number of times the educational video was watched were not known. This represents a limitation in terms of the objectivity and measurement power of the obtained scores. However, all evaluations were conducted by an observer unaware of the group assignments (blinded), thereby reducing the risk of bias in scoring. Based on the experiences gained from this pilot study, it is planned that, in future surgical knot-tying training videos, common student mistakes will be visually presented, and interactive feedback mechanisms will be included.
Conclusion
While VAssL provides accessibility and flexibility, FtFL remains superior in surgical skill acquisition due to direct feedback and expert guidance. Future studies should focus on hybrid training models incorporating both methods to maximize educational outcomes.
Ethical considerations
The study was approved by the Eskisehir Osmangazi University Nonclinical Ethical Committee in accordance with the Declaration of Helsinki (Approval No. 2024/35).
Artificial intelligence utilization for article writing
None.
Acknowledgment
Special thanks to Prof Dr Cengiz Bal for statistical analysis.
Conflict of interest statement
There is no conflict of interest.
Author contributions
AZ and OU conceived and designed the study. OU, AZ, and YSA were responsible for data acquisition. YMB analyzed the data. MU responsible for supervision. All authors interpreted the results, critically revised the manuscript for intellectual content, and approved the final version.
Funding
No funding was received for this study.
Data availability statement
Data are available upon reasonable request from the corresponding author due to ethical and privacy considerations.
Background & Objective: In contemporary medical education, the shortage of instructors for basic skills training has led to a growing shift toward alternative instructional methods, among which video-based training is a notable approach. This study compared the results of Face-to-Face Learning (FtFL) and Video-Assisted Learning (VAssL) in the acquisition of surgical skills by medical students.
Materials & Methods: Our study was a prospective, single-blinded, randomized controlled pilot trial. 32 medical students were randomly allocated 1:1 to FtFL (n = 16) or VAssL (n = 16) using computer-generated random numbers and sealed opaque envelopes to ensure allocation concealment. The primary outcome was knot-setting success. Secondary outcomes included hand movement proficiency and the number of knots tied per minute. All assessments were performed using a structured scoring table by two blinded assessors.
Results: The mean number of knots tied per minute was 10.97 ± 4.13, and the median knot score was 4 (3–5), with no significant difference between groups (p = 0.476, p = 0.306, respectively). Over 90% of participants succeeded in hand movements, except for knot setting, which had a 65.6% success rate overall. The FtFL group showed significantly higher success in knot setting compared to the VAssL group (93.8% vs. 37.5%, p = 0.002, Cohen’s d = 1.60) and superior hand movement proficiency (median 5 )5–5(vs. 4 )4–5(, p = 0.001).
Conclusion: Face-to-face learning is more beneficial than video-assisted learning for correcting deficiencies and mistakes in medical students' acquisition of surgical skills.
Introduction
master-apprentice model, has been regarded as a standard teaching method for hands-on skills [6]. It provides learners with real-time feedback, immediate error correction, and instructor-guided repetition — all of which are essential for developing motor precision [7]. Yet, the growing number of medical students and the limited availability of surgical instructors have strained the sustainability of this model [8]. Meanwhile, advances in digital tools have paved the way for Video-Assisted Self-Directed Learning (VAssL), an increasingly popular method that enables flexible, repeatable, and accessible skill acquisition outside the traditional classroom [9]. In this context, VAssL is gaining increasing interest for its benefits, such as more efficient use of educational resources, improved accessibility, and the ability for learners to progress at their own pace. This approach offers greater flexibility, broader access to information, and the ability to complete coursework at a self-directed pace. Interaction with instructors is one of the distinctive advantages that make online learning appealing to many students [10]. Despite this, some argue that passive video training, lacking interactive feedback mechanisms, may be inadequate for teaching complex psychomotor skills such as surgery [11]. One of the most important advantages of face-to-face versus video-assisted is better skill acquisition. Previous research comparing face-to-face and video-based learning has shown that supervised instruction tends to yield better technical performance, while video-assisted methods provide comparable theoretical understanding but may fall short in manual precision. Educational programs designed to strengthen both theoretical understanding and practical ability are therefore indispensable in modern medical training [6,12]. Numerous studies indicate that many final-year medical students complete their training without achieving sufficient proficiency in these elementary technical tasks, revealing a persistent shortfall in undergraduate surgical education [13]. For centuries, surgical education has incorporated simulation-based training using animal models, cadavers, and various materials designed to mimic tissues and organs [14]. Enhancing students’ knowledge and skills through structured educational courses is essential [15]. In particular, carefully structured surgical skills courses—progressing from fundamental to advanced levels—provide a secure environment for experiential learning while ensuring that competence in essential techniques is achieved prior to graduation [16]. Surgical skills courses typically include modules such as suturing, knot-tying, instrument handling, tissue approximation, and basic laparoscopic tasks, enabling students to gradually develop psychomotor proficiency under standardized conditions [17]. Evidence suggests that structured skills training significantly enhances psychomotor competence, improves procedural confidence, and positively impacts subsequent clinical performance [18]. Surgical simulators provide a safe space where learners can experiment with procedures at their own pace, repeatedly refining their skills while learning from errors without pressure [19]. Notably, simulators are standardized, reproducible, measurable, precise, continuously accessible, and objective [20]. Basic surgical skills learned during medical education may make it easy to learn more advanced surgical techniques during surgical assistance [13]. Therefore, we argue that basic surgical skills should be taught to medical students. How this education should be delivered, and the effect of video-assisted/online education on this, are among the most popular issues today. The acceleration of digitalization in medical education has made the comparison of traditional and innovative teaching methods highly significant, as there are still regions in the world where the number of instructors is insufficient to meet the educational needs of medical students. In such contexts, new instructional models are needed to ensure equitable educational opportunities. However, despite the growing body of evidence, gaps remain in understanding the comparative effectiveness of face-to-face and video-assisted instruction, specifically in knot-tying performance, particularly among final-year medical students—a group expected to demonstrate clinical readiness. Clear evidence is still needed regarding which method better supports safe, standardized, and efficient acquisition of this essential skill. Therefore, this randomized controlled pilot study aims to compare the effectiveness of FtFL and VAssL methods in teaching surgical knot-tying to final-year medical students and to provide insights for optimizing future surgical training models.
Materials & Methods
Design and setting(s)
The study was experimental and conducted with final-year medical students who had not received any prior knot-tying education. Written informed consent was obtained from all participants prior to enrollment. The study was conducted between October 7, 2024, and October 14, 2024. The study was approved by the Eskisehir Osmangazi University Nonclinical Ethical Committee in accordance with the Declaration of Helsinki. The study was designed, conducted, and reported in accordance with the Consolidated Standards of Reporting Trials (CONSORT) 2010 guidelines. The completed CONSORT checklist is provided as Appendix 1.
Participants and sampling
This sample size calculation was performed using Minitab® Statistical Software version 16. The computation was based on values reported in the literature [21], assuming a mean difference of 15.68 between the two groups and a pooled standard deviation of 9.76. Using these parameters, the effect size (Cohen’s d) was calculated as 1.60, and the analyses revealed that, with a power of 99% (α = 0.05, 1-ß = 0.99), a total sample size of 32 (n1:16, n2:16) was needed. A total of 32 students were involved in the study (see Figure 1 for the CONSORT flow diagram). This pilot study was a randomized, single-blinded study. The randomization sequence was generated by an independent researcher using computer-generated random numbers. Allocation concealment was ensured through sequentially numbered, sealed, opaque envelopes prepared and stored by the same researcher. Immediately before the training, a second researcher—blinded to the randomization list—distributed the envelopes, and each participant opened their envelope to learn their assignment. In this way, students were allocated to the face-to-face group (n = 16) or the video group (n = 16). The assessors were fully blinded; evaluations were conducted individually using coded forms without group identifiers, and the allocation list was kept separately by an independent researcher. Both instructors rehearsed the knot-tying procedure prior to the study according to standardized steps and rules, and they cross-evaluated each other’s performance to ensure inter-rater reliability. Both groups received the same knot-tying instruction. In the FtFL group, two instructors (one gastrointestinal surgery specialist and one senior general surgery assistant) supervised 16 students for a single 60-minute session that included both teaching and hands-on practice. The VAssL group received an 87-second Turkish instructional video via WhatsApp, which they could watch, pause, and rewind as needed. Frequency and total viewing time were not monitored, so their effects on learning outcomes could not be assessed. The study flow is presented in Fig. 1. These procedures ensured consistent instruction and provided initial evidence of the training interventions' content validity and reliability.
Figure 1. Flowchart diagram of the study.
Tools/Instruments
A shoestring and a file clip were used for knot-tying in the education video, and the same materials were given education were provided by the authors. The training setup and the training steps in which manual skills were evaluated are shown in Figure 2.
Figure 2. Visual depiction of the sequential steps for performing the square knot: (1) Correct initial grip of both rope ends, (2a, 2b) Formation of the first loop using a three-finger technique, (3) Transfer of the rope from the non-dominant to the dominant hand, (4) Execution of the cross‑tying maneuver, (5) Final knot setting and tightening.
Data collection methods
Researchers who were blinded to group assignment evaluated participants' knot-tying skills after one week of self‑practice. The researchers' unique scoring scale was used for evaluation. As a result of the validity and reliability analyses of this scale, the Cronbach’s α scale level was calculated as 0.8. The scale consists of two subcomponents: (1) Knot Score, ranging from 0 to 5 points based on the number of knots tied in one minute; (2) Hand Movement Proficiency Score, ranging from 0 to 5 points based on the correct execution of knot-tying steps (Table 1). The total score ranges from 0 to 10.
Participants who scored six or higher were considered "successful."
Data analysis
The normality of the distribution of continuous data was analyzed via the Kolmogorov-Smirnov test. When normally distributed, they were reported as mean ± SD and compared using Student's t-test. If they were non-normally distributed, they were presented as median (25–75 interquartile range), and Mann-Whitney’s U test was performed for comparisons. Categorical data were given as frequency (percentage) and were compared by the Chi-square test or Fisher’s exact test. A p-value of < 0.05 was considered statistically significant. Analyses were performed using IBM SPSS Statistics for Windows, version 25.0 (IBM Corp., Armonk, N.Y., USA), and Minitab 16 statistical software.Table 1. Scoring system for knot‑tying performance assessment
Note: The total score ranges from 0 to 10 (Knot Score + Hand‑movement Proficiency Score). A total score of ≥6 was considered “successful”.
Abbreviations: n, number; vs., versus.
Results
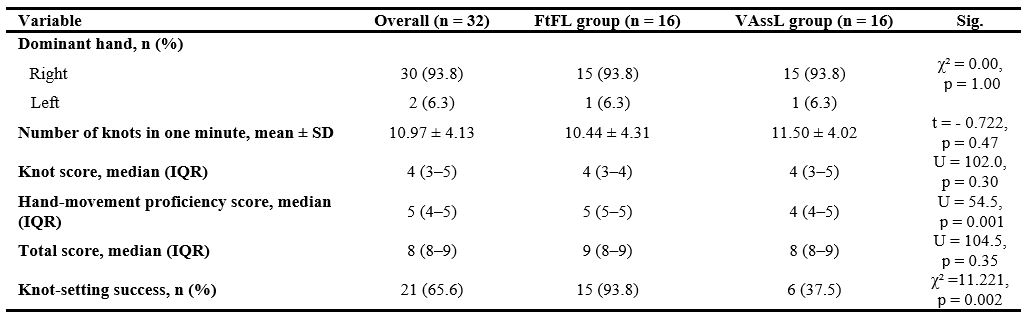
Table 2 presents the results and comparisons of the evaluation criteria for the study group and subgroups. The mean number of knots in one minute was 10.97 ± 4.13, and the median knot score was 4 (3–5) with no statistically significant difference between the groups (p = 0.476). More than 90% of participants were successful in hand movements, except for knot setting. The success rate of knot setting was 65.6% across the entire study group. The FtFL group was found to be statistically significantly more successful at knot setting than the VAssL group (n = 15 (93.8%) vs. n = 6 (37.5%), p = 0.002). Similarly, the FtFL group achieved a significantly higher median hand‑movement proficiency score compared to the VAssL group (5 (IQR: 5–5) vs. 4 (IQR: 4–5), p = 0.001). A participant in the VAssL group tied only three knots and scored just 1 point; in the hand movement proficiency assessment, they received no points. This outcome may be attributed to the inability of video‑assisted training to accommodate individual differences in learning pace and the absence of real‑time instructor feedback. Feedback gathered from participants after the training supports these findings. Students in the VAssL group expressed that video training was useful for transferring basic knowledge; however, they emphasized that a significant drawback was the inability to verify the accuracy of the knot tied by an expert. On the other hand, participants in the FtFL group stated that they were pleased to have direct communication with the instructor, but they viewed the inability to rewatch the training as a disadvantage.
Table 2. Comparison of knot‑tying performance outcomes between the FtFL and VAssL groupsAbbreviations: n, number; vs., versus.
Results
Table 2 presents the results and comparisons of the evaluation criteria for the study group and subgroups. The mean number of knots in one minute was 10.97 ± 4.13, and the median knot score was 4 (3–5) with no statistically significant difference between the groups (p = 0.476). More than 90% of participants were successful in hand movements, except for knot setting. The success rate of knot setting was 65.6% across the entire study group. The FtFL group was found to be statistically significantly more successful at knot setting than the VAssL group (n = 15 (93.8%) vs. n = 6 (37.5%), p = 0.002). Similarly, the FtFL group achieved a significantly higher median hand‑movement proficiency score compared to the VAssL group (5 (IQR: 5–5) vs. 4 (IQR: 4–5), p = 0.001). A participant in the VAssL group tied only three knots and scored just 1 point; in the hand movement proficiency assessment, they received no points. This outcome may be attributed to the inability of video‑assisted training to accommodate individual differences in learning pace and the absence of real‑time instructor feedback. Feedback gathered from participants after the training supports these findings. Students in the VAssL group expressed that video training was useful for transferring basic knowledge; however, they emphasized that a significant drawback was the inability to verify the accuracy of the knot tied by an expert. On the other hand, participants in the FtFL group stated that they were pleased to have direct communication with the instructor, but they viewed the inability to rewatch the training as a disadvantage.
Note: Continuous data are presented as mean ± standard deviation (SD) or median (interquartile range, IQR), as appropriate. Categorical data are presented a s frequency (percentage). The Mann‑Whitney U test was used for non‑normally distributed continuous variables, and the Chi‑square or Fisher’s exact test was used for categorical comparisons.
Abbreviations: FtFL, face‑to‑face learning; VAssL, video‑assisted self‑directed learning; n, number; SD, standard deviation; IQR, interquartile range; Sig., Statistical Significance; p, probability-value.
Abbreviations: FtFL, face‑to‑face learning; VAssL, video‑assisted self‑directed learning; n, number; SD, standard deviation; IQR, interquartile range; Sig., Statistical Significance; p, probability-value.
Discussion
In our study, the most prominent finding was that participants in the FtFL group achieved more knots and demonstrated greater hand movement proficiency than those in the VAssL group. This result aligns with the expectation that direct instructor communication and real-time feedback enhance the acquisition of complex psychomotor skills. The absence of prior exposure to the alternative training method in both groups allowed us to more precisely observe the pure effect of each educational approach. These factors likely explain why the FtFL group outperformed the VAssL group.
A second key finding was the superior hand skill proficiency scores in the FtFL group, emphasizing the importance of instructor-provided feedback for mastering surgical knot-tying. Similarly, Tejos et al. [11]
found that traditional education was more effective than video-based learning in teaching basic surgical skills. They also reported that a video-guided learning approach without feedback is insufficient compared to expert or
peer feedback when developing an optimized teaching program for suturing skills. However, a limitation of that study was the potential difference in training and practice durations between the video-based and traditional groups, as the self-directed video group’s study time was not verified. The lack of precise data on students’ practice times in our study is a comparable limitation that may partly explain variations in performance. Another important observation is that face-to-face teaching continues to show advantages in performance-based clinical skills. In the study by Shen et al. [6], two groups completing a neurosurgery clerkship—one online and one face-to-face—were compared. Although no significant difference was found in theoretical knowledge, the face-to-face group performed better on clinical practice tasks, such as history-taking and physical examination. The authors concluded that while online teaching can serve as a valuable supplementary tool, it cannot fully replace face-to-face instruction in the development of clinical practical skills. Our findings are consistent with this view, as the VAssL group lacked immediate corrective feedback, which may have hindered their psychomotor learning. Contrary to studies supporting the necessity of feedback, in the study of Kumins [7] et al. in which knot-tying and suturing training was given online, they stated that the feedback provided by the trainers may not be considered necessary for learning. This difference is thought to be due to factors such as variations in practice duration and differences in the availability of individualized feedback. In a randomized study, no difference was found between the face-to-face and video-assisted education groups in terms of surgical skill improvement [9]. A systematic review found that video-assisted and traditional education did not differ in teaching basic surgical skills [8]. As a result of these studies, video-assisted education may be considered an alternative to face-to-face education. However, in this randomized controlled study, both groups received face-to-face training first, and then one group received video-assisted training; after that, the evaluation was made between the groups. The study by Raythatha et al. [22] was parallel to the previous one; both groups received face-to-face education, and only one group had the opportunity to receive video-assisted education. The results were better for the video-assisted group. Yet, those studies differed from ours because both groups first received face-to-face instruction before video reinforcement, making it difficult to isolate the true comparative effects of the methods. In our study, groups were trained exclusively with a single method, allowing us to directly compare their isolated effects, which may explain why FtFL demonstrated superiority in our study. A further finding of our analysis suggests that VAssL may be improved by refining instructional content. Providing videos with detailed explanations targeting commonly observed weaknesses could improve both hand movement proficiency and the number of knots tied. This may help narrow the performance gap between VAssL and FtFL methods. The limitations of this study include the fact that it was a pilot study conducted in a small study group. The total time that the students practiced knot-tying on their own and the number of times the educational video was watched were not known. This represents a limitation in terms of the objectivity and measurement power of the obtained scores. However, all evaluations were conducted by an observer unaware of the group assignments (blinded), thereby reducing the risk of bias in scoring. Based on the experiences gained from this pilot study, it is planned that, in future surgical knot-tying training videos, common student mistakes will be visually presented, and interactive feedback mechanisms will be included.
Conclusion
While VAssL provides accessibility and flexibility, FtFL remains superior in surgical skill acquisition due to direct feedback and expert guidance. Future studies should focus on hybrid training models incorporating both methods to maximize educational outcomes.
Ethical considerations
The study was approved by the Eskisehir Osmangazi University Nonclinical Ethical Committee in accordance with the Declaration of Helsinki (Approval No. 2024/35).
Artificial intelligence utilization for article writing
None.
Acknowledgment
Special thanks to Prof Dr Cengiz Bal for statistical analysis.
Conflict of interest statement
There is no conflict of interest.
Author contributions
AZ and OU conceived and designed the study. OU, AZ, and YSA were responsible for data acquisition. YMB analyzed the data. MU responsible for supervision. All authors interpreted the results, critically revised the manuscript for intellectual content, and approved the final version.
Funding
No funding was received for this study.
Data availability statement
Data are available upon reasonable request from the corresponding author due to ethical and privacy considerations.
Article Type : Orginal Research |
Subject:
Medical Education
Received: 2025/06/4 | Accepted: 2025/11/29 | Published: 2026/01/1
Received: 2025/06/4 | Accepted: 2025/11/29 | Published: 2026/01/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
