
Fri, Jul 10, 2026
[Archive]
Volume 18, Issue 4 (2025)
J Med Edu Dev 2025, 18(4): 119-139 |
Back to browse issues page

Ethics code: NOT (Review article)
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Mahdi R, Keykha A, Kaliisa R, Darabi F. Exploring applications of artificial intelligence in enhancing the quality of medical education: a mixed methods research synthesis. J Med Edu Dev 2025; 18 (4) :119-139
URL: http://edujournal.zums.ac.ir/article-1-2480-en.html
URL: http://edujournal.zums.ac.ir/article-1-2480-en.html

1- Department of Futures Studies, Institute for Cultural and Social Studies, Ministry of Science, Research and Technology, Tehran, Iran
2- Sharif Policy Research Institute, Sharif University of Technology, Tehran, Iran ,ahmad.keykha72@sharif.edu
3- Department of Education, University of Oslo, Oslo, Norway
4- Department of Educational Psychology, Islamic Azad University, Science and Research Branch, Tehran, Iran
2- Sharif Policy Research Institute, Sharif University of Technology, Tehran, Iran ,
3- Department of Education, University of Oslo, Oslo, Norway
4- Department of Educational Psychology, Islamic Azad University, Science and Research Branch, Tehran, Iran
Keywords: artificial intelligence (AI), medical education, educational technology, quality improvement, mixed methods synthesis
Full-Text [PDF 767 kb]
(675 Downloads)
| Abstract (HTML) (1116 Views)
Full-Text: (50 Views)
Abstract
Background & Objective: Academic systems are among the many spheres of human life highly influenced by artificial intelligence (AI). The idea of quality in medical education is changing as a result of AI-driven developments, creating both opportunities and difficulties. The purpose of this study is to investigate how AI might be used to improve the quality of medical education.
Materials & Methods: Mixed methods research synthesis was the approach taken. Relevant studies published in Science Direct, Springer, ERIC, Emerald, Sage Journals, Wiley Online Library, PubMed, and Google Scholar between 2015 and 2025 were found using targeted search terms. Quality was assessed through the Mixed Methods Appraisal Tool (MMAT) and selection process followed Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The final review included 49 studies that met the criteria. A model with eight dimensions of the quality of medical education was employed to analyze the data.
Results: The results were grouped into eight categories: mission and goals, organizational structure and governance, faculty members, students, teaching and learning processes, curricula, facilities, and research activities. AI was found to have a positive effect on all areas, with the most focus on faculty members (38 citations) and teaching-learning processes (36 citations). It was found that these themes were very important for making education better. By comparison, mission and objectives, and research activities received little reference (8 references each), indicating strategic and research-focused AI integration lacunae.
Conclusion: AI has the most potential to change how medical education is taught by using new teaching tools, better lesson plans, and personalized learning. But the fact that research and planning dimensions don't cover everything shows how important it is to do research and make policies with clear, well-defined goals. Balanced implementation of AI in all dimensions of quality is needed to bring sustainable and comprehensive transformations in medical education. The current study offers significant implications to educators, policymakers, and researchers for guiding AI-supported education reforms in the future.
Introduction
Medical education is a key part of higher education because it has a direct impact on the quality of care and patient outcomes. Unlike generic areas of education, medical education necessitates training of competent health professionals that combine extensive theoretical knowledge with practical as well as clinical competencies needed to contribute meaningfully to society [1]. So, the quality of medical education has a direct effect on the efficiency of the healthcare delivery system and public health [2]. There are many challenges to providing high-quality medical education, such as constantly updating the curriculum, training faculty, coming up with new ways to teach, and coming up with strong ways to test students. These efforts are meant to make sure that graduates have not only a lot of knowledge but also the important clinical and interpersonal skills they need.
Improving the quality of medical education has therefore become a priority for different stakeholders such as learners, teachers, patients, healthcare workers, regulatory agencies, and financiers [3]. To address this priority, quality in medical education has drawn significant scholarly attention as researchers seek to understand and maximize it amidst evolving health needs [4]. The quality of medical education is important beyond the academe since it is irrevocably entwined with the ability of health systems to deliver safe, effective, and equitable care. All stakeholders agree that without earnest dedication to the quality of medical education, quality improvements in healthcare delivery are not feasible [5]. High-quality medical education is characterized by well-structured educational systems, comprehensive curricula, qualified faculty, and enhanced teaching practices. Furthermore, medicine graduates need to attain a blend of soft skills, practical skills, and theory-based medical understanding [6]. However, "quality" is an aggregate and comparative term and is still challenging to define as there are multiple interpretations based on stakeholders' perceptions and standards [7]. Amidst rapidly evolving international trends shaping higher education today, quality has become increasingly critical. Universities are faced with complex issues with technological advancement accelerating, calling for adaptive interventions and revolutionary changes in their function as educators [8]. Artificial Intelligence (AI), a revolutionary technological innovation, also promises to enhance the quality of education in every discipline, including medical education. The application of AI—including intelligent tutoring systems, chatbots, adaptive learning platforms, automated grading, and learning analytics—enables individualized learning experiences, enhances teaching effectiveness, and streamlines academic administration [9-13]. In addition to its well-known applications in medical training, artificial intelligence is driving a wide range of innovations across the broader field of medicine. For instance, personalized medicine has been developed with the aim of providing drugs based on the individual characteristics of patients [14]. In addition to its well-known applications in medical training, artificial intelligence is driving a wide range of innovations across the broader field of medicine [15]. Yet another key focus area is the early diagnosis of various diseases, which results in improved prevention and reduced costs of treatment [16]. Also, advances in medical imaging have provided improved analysis of radiological data, thereby improving diagnostic efficiency [17]. In medical care, AI has proven to be an effective tool for patient monitoring and surveillance [18], while clinical decision-support systems have enhanced diagnostic and therapeutic processes [19].
Medical data management has also been streamlined through advanced algorithms, enabling the analysis of large-scale health datasets [20]. In addition, genome analysis and genetic medicine have opened new pathways for treatments based on patients’ genetic profiles [21]. Virtual medical consultations and AI-driven assistants have also played a substantial role in improving patient engagement and expanding access to healthcare services [22]. Finally, AI has contributed to optimizing therapeutic processes and improving the overall efficiency of healthcare systems [23]. Despite this potential, the integration of AI into education presents several challenges. Some of these are the danger of relying too much on AI tools, which could hurt academic standards, worries about student data privacy, and the possibility of biases being built into AI platforms through algorithms that reflect human biases [24, 25]. Therefore, AI should not be regarded as a universal remedy, but rather as a supportive instrument whose efficacy is contingent upon the establishment of suitable safeguards. Current studies underscore these dual facets of AI in education. Kabudi [26] identifies critical areas such as educator roles, support for special-needs students, racial and data bias in AI-based learning systems, and commercialization challenges. Flores-Viva and García-Peñalvo [27] emphasize ethical considerations in AI’s educational applications. Nkechi et al. [28] show how AI can help close the digital divide and overcome language barriers to make education more equal. Ajani et al. [29] talk about how AI can help with personalized learning, better teaching methods, and more efficient administration. They also talk about privacy and ethical issues. AlSagri and Sohail [30] argue that deeper understanding of AI capabilities can inform policies fostering equitable and sustainable education systems. This study employs a mixed methods research synthesis approach to address international research gaps regarding AI’s role in improving education quality, with a novel focus on medical education. The results give a broad, worldwide view of how AI could improve the quality of medical education. This study helps close the knowledge gap by giving educators, policymakers, and researchers who want to use AI to improve the quality of medical education useful information. This study adheres to the most prevalent framework for evaluating the intrinsic quality of university teaching [31–35]. There are eight principal dimensions in the conceptual model: Mission and Objectives, Organizational Structure and Management, Faculty Members and Students, Teaching-Learning Processes, Educational Programs and Curricula, Educational and Research Facilities, and Research Activities.
Materials & Methods
Design and setting(s)
Since both quantitative and qualitative studies, as well as those employing mixed-method research designs, are available for examining the applications of artificial intelligence in quality of medical education, we chose an integrated Mixed-Methods Research Synthesis (MMRS) design as the methodological framework for our review. A mixed-methods research synthesis is a form of systematic review that applies the principles of mixed-methods inquiry. In essence, such a study is expected not only to include two distinct strands—one qualitative and one quantitative—each with its own questions, data, analyses, and conclusions—but also to integrate, link, or connect these strands in a meaningful way [36]. Specifically, we adopted the MMRS framework developed by Heyvaert and colleagues [37]. A diagrammatic overview of this framework can be found in Figure 1. Considering the multidimensional complexity of artificial intelligence applications quality of medical education, it seems essential to employ a mixed-methods approach in the synthesis of the studies (Figure 1). Quantitative studies primarily seek to investigate the effectiveness of AI tools by measuring the performance improvement of learners, or system accuracy, while qualitative studies evaluate attitudes, experiences, and ethical and educational dilemmas with the implementation of this technology. A synthesis of these two types of data provides a richer understanding of the phenomenon. On one hand, quantitative data provide empirical and objective evidence about efficiency and outcomes; on the other hand, qualitative data primarily offer enhanced insights into the contexts, meanings, and processes associated with the use of AI in quality of medical education. In a methodological sense, a mixed synthesis approach is especially relevant for publishing the synthesis or results of qualitative and quantitative studies, as it allows for interpretation of these diverse findings within a unifying framework. In this manuscript, and as shown in Figure 1, data from the base qualitative and quantitative studies were first synthesized in their separate studies. In the last stage, through an integrative synthesis, similarities, differences, and complementarity across the two strands were assessed. The framework provides a six-stage process [37], and subsequent sections of this report describe the process we undertook for each of the particular six stages of this study.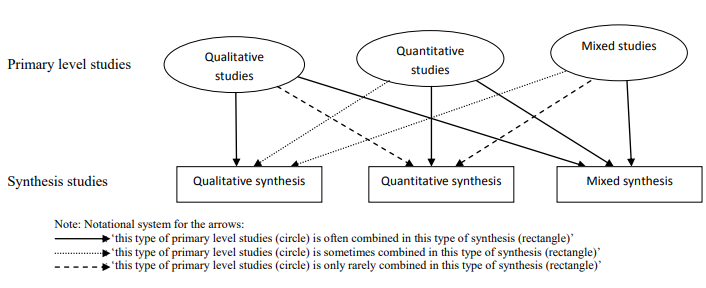
Figure 1. Qualitative, quantitative, and mixed methods research synthesis
The problem identification and question formulation stage
The research question was designed using the standard PICo/PICO framework, which helps researchers define the scope and objectives of their study with precision and clarity. In this study, Population (P) refers to students, faculty members, administrators, and other stakeholders in both medical and non-medical education systems, who are considered the primary users or beneficiaries of AI applications. Interest/Intervention (I) represents the phenomenon under study, namely the application of Artificial Intelligence in improving the quality of medical education. Context (C) refers to the academic settings, including higher education institutions and medical training centers where AI technologies have been integrated into educational processes. To ensure methodological rigor, the search strategy was explicitly derived from this framework. The Population (P) was operationalized into keywords such as “medical students,” “residents,” “faculty,” and “medical education stakeholders.” The Intervention (I) generated terms including “artificial intelligence,” “AI,” “machine learning,” “deep learning,” “chatbots,” and “educational technology.” The Comparison (C) dimension was not uniformly applicable across studies due to the heterogeneity of their designs. However, where relevant, comparative terms such as “traditional education,” “non-AI learning,” or “conventional teaching” were included. Finally, the Outcomes (O) were framed in terms of “quality improvement,” “learning outcomes,” “teaching effectiveness,” and “educational quality,” which were translated into keywords such as “quality of medical education,” “teaching quality,” and “educational improvement.” By systematically mapping these PICo/PICO elements into database search strings, we ensured comprehensive coverage of the literature relevant to AI applications in enhancing the quality of medical education. Grounded on such considerations, this research question was formulated: What are the applications of AI in enhancing the quality of medical education? To ensure accuracy in answering this question, key constructs were operationally defined to provide consistency and clarity in study selection and data analysis. AI applications were classified as any digital or computational systems that utilize machine learning, natural language processing, deep learning, expert systems, or other associated intelligent technologies that are applied within educational environments. These included, but were not limited to, intelligent tutoring systems, adaptive learning systems, chatbots, automated grading systems, virtual or augmented reality made easier by AI, predictive analytics, and AI-driven academic management systems. We looked at the following categories when it came to levels of medical education: Undergraduate Medical Education (UME): Basic programs that lead to the first medical degrees (like MBBS or MD); Postgraduate Medical Education (Residency and Fellowship): Structured training programs for specialists after undergraduate medical education; Continuing Medical Education (CME): Formal and informal learning activities that help practicing doctors and other healthcare professionals keep their skills up to date and improve them; Interprofessional Education (IPE): Learning spaces where medical students and allied health professionals learn together using AI-enabled tools. Only research that specifically addressed the application of AI at one or more of these levels of medical education, with a clear connection to quality improvement, was considered eligible for analysis.
The development of a review protocol and the literature search
The study protocol was crafted to facilitate mixed methods research synthesis MMRS framework regarding the utilization of AI in the enhancement of medical education quality. The creation of the protocol needed multiple steps: crafting the research question and study objectives; choosing a conceptual framework; setting up inclusion and exclusion criteria; devising the search strategy and resource retrieval techniques; delineating the screening and selection process for studies; choosing tools to evaluate study quality; deciding on the data analysis method; and validating and confirming the results. We did a systematic search of the literature for peer-reviewed articles that were published in English between 2015 and 2025. This decade was chosen to include the era of large progress in machine learning, deep learning, and natural language processing, which have become essential in revolutionizing educational assessment and improving quality. The electronic databases Science Direct, Springer, ERIC, Emerald, Sage Journals, Wiley Online Library, PubMed, and Google Scholar were all searched. With an emphasis on (O) Quality Improvement, the search strategy combined keywords associated with (I) Artificial Intelligence and (P) Medical Education in a Boolean query based on the PICO framework. For every database, the search string
was modified. Below is a representative example: An example of a search query is: ("artificial intelligence" OR AI OR "machine learning" OR chatbot*). AND ("clinical training" OR "medical student*" OR "medical education") AND ("learning outcome*" OR "educational quality" OR "quality improvement")
The following standards served as a guide for choosing the study: Criteria for inclusion: publications from 2015–2025 that are peer-reviewed in English, specifically address AI applications in medical education, and use either mixed-methods, quantitative, or qualitative research.
Exclusion criteria include: studies done outside of the designated time frame; editorials, opinion pieces, and non-peer-reviewed literature; and articles that do not focus on improving educational quality.
Look at the selection procedure: As shown in Figure 2, the PRISMA guidelines were followed during the study selection process. 187 records were found in the first database search. 77 studies were excluded after the titles and abstracts of these records were screened and duplicates were removed. After abstract review, 43 of the 110 remaining studies were eliminated. Following a full-text evaluation of the 67 studies that were found, 18 articles that did not fit the inclusion criteria were eliminated.
The MMAT (Mixed Methods Appraisal Tool, 2018 version) was adopted to assess the quality of the methodological approach of all the studies included in this synthesis. Each study was reviewed based on five criteria followed by a score of between zero to five. The criteria cut-off was defined to be any study that scored three or above, which is demonstrative of a compromise between quality and feasibility. Lower scores indicate methodological concerns with confidence and an increased risk of bias which may affect confidence in the findings from this synthesis.
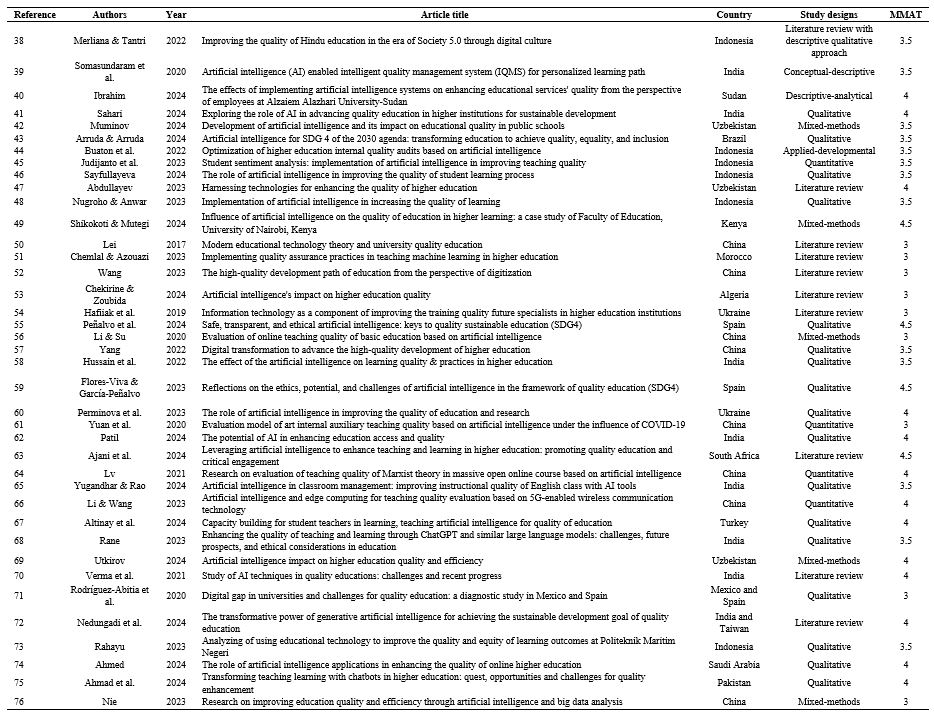
As such a score of three or above is the minimum standard of quality and validity to avoid studies that demonstrate methodological concerns from being included in the synthesis. The MMAT scores for studies included in this synthesis are shown in Table 1.

Figure 2. PRISMA flowchart for screening the articles
Table 1. Bibliography of the selected articles
The selection of an appropriate design and method
The third phase of this investigation selected the mixed content analysis approach as the primary analytical lens in order to determine the appropriate synthesis design and method.
The goal of the research is to achieve an in-depth understanding of the uses of artificial intelligence in medical education through the integration of quantitative and qualitative evidence, and as such, content analysis offers a mechanism by which to provide shared meaning units to represent the diverse findings of primary studies, and identify categories and themes from the units.
Further, within this methodological approach, data from quantitative studies have also been transformed into classizable units of meaning via content-based extraction and description—for example, by identifying indicators, variables, statistical findings or evidence statements—that can also be analyzed alongside qualitative findings. This methodological approach design has constituted a synthesis that is grounded in meaning and content as opposed to data type, thus generating a coherent and multi-faceted account of applications of artificial intelligence in the quality of medical education.
The data extraction and evaluation stage
The articles' texts were read several times to help readers become fully immersed in the content before the data was extracted.
Key sections of the articles were documented in a structured format using Microsoft Word. For identifying key concepts—those conveying the most significant meanings—the paragraph was utilized as the unit of analysis, from which the most critical concepts were extracted.
Throughout the analysis process, memos were employed extensively.
During the initial reading of the texts, researchers made notes on key points, trends, or potential connections.
The notes included preliminary impressions of the focal issues of the articles, key ideas related to the research issue, and emerging ideas or issues worth investigating.
During coding, memos aided the recording of the rationale for why the codes were chosen, meaning-making, and interconnection, thus promoting conversation among the researchers.
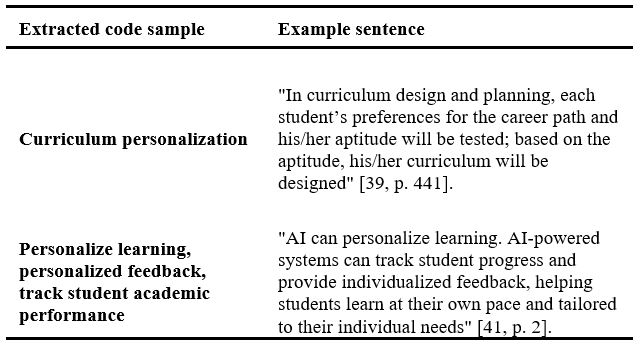
In later data organization and extraction, memos proved helpful to aid the research team to compile suitable codes to create categories and overall themes. Examples of how to extract codes are shown in Table 2.
Table 2. Examples of how to extract codes
The data analysis and interpretation stage
We followed Elo and Kyngas [77] This framework for examining information is built upon three foundational pillars. The initial stage focuses on establishing a foundation, where information is gathered and a structure for categorization is defined.
The subsequent stage, concerned with systematic arrangement, involves a meticulous review and sorting of the data based on its alignment with pre-established classifications. The final and culminating stage is dedicated to presenting the outcomes, which articulates the findings to enable a deeper understanding of the identified patterns. Furthermore, the insights derived from this process can be significantly augmented by integrating a mixed-methods approach that incorporates both statistical and interpretive techniques. To ensure consistency, the concepts derived from each classification session were compared to measure the degree of agreement between the two coding processes. The process involved labeling similar codes across the two-time intervals as "agreement" and dissimilar codes as "disagreement." The frequency of agreements and disagreements was then used in a formula to calculate the reliability of the coding process over time. This study conducted coding and classification twice, with a 14-day interval between sessions. A total of 403 concepts were extracted, with agreement reached on 175 of them between the two coding sessions. The calculated reliability for this retest was 86%, which, since it exceeds the 60% threshold, confirms the reliability of the coding process [78].

The reporting and discussing of research findings
Finally, the findings were systematically documented and shared, ensuring a comprehensive and rigorous analysis process.
Results
As stated earlier, we used a standardized framework for quality assessment, which has been widely accepted in many studies, as a standard by which to measure the caliber of medical education. To ensure alignment with this framework, key concepts were extracted and then categorized according to their similarities and differences. Mission and objectives, organizational structure and management, faculty, students, teaching-learning processes, educational programs and curricula, academic and research facilities, and research activities are the eight primary dimensions that make up the framework. Within this framework, the integrated key concepts were taken into consideration as criteria. The departmental goals and missions are covered by the Mission and Objectives dimension. Academic departments' organizational setup, including policies, staffing levels, and services, is covered by the Organizational Structure and Management dimension. Academic counseling, consultation accessibility, and faculty-student interactions are all included in the Faculty Members dimension. The Students dimension covers student activities like participation in departmental planning, awareness of departmental goals, and knowledge of their rights and responsibilities.
Additionally, teaching and learning strategies, technology integration, and student assessment procedures are all included in the Instruction-Learning Processes dimension. The academic programs themselves, including their alignment with departmental missions and their design in accordance with curriculum planning principles, are covered by the Educational Programs and Curricula dimension. The infrastructure and resources that are available, including libraries, information systems, and technological services, are covered by the Educational and Research Facilities dimension. Lastly, academic work done by both students and faculty is included in the Research Activities dimension. The analysis's specific results are shown in Tables 3 and 4.
Table 3: Analysis of findings based on the standard framework for assessing the quality of medical education
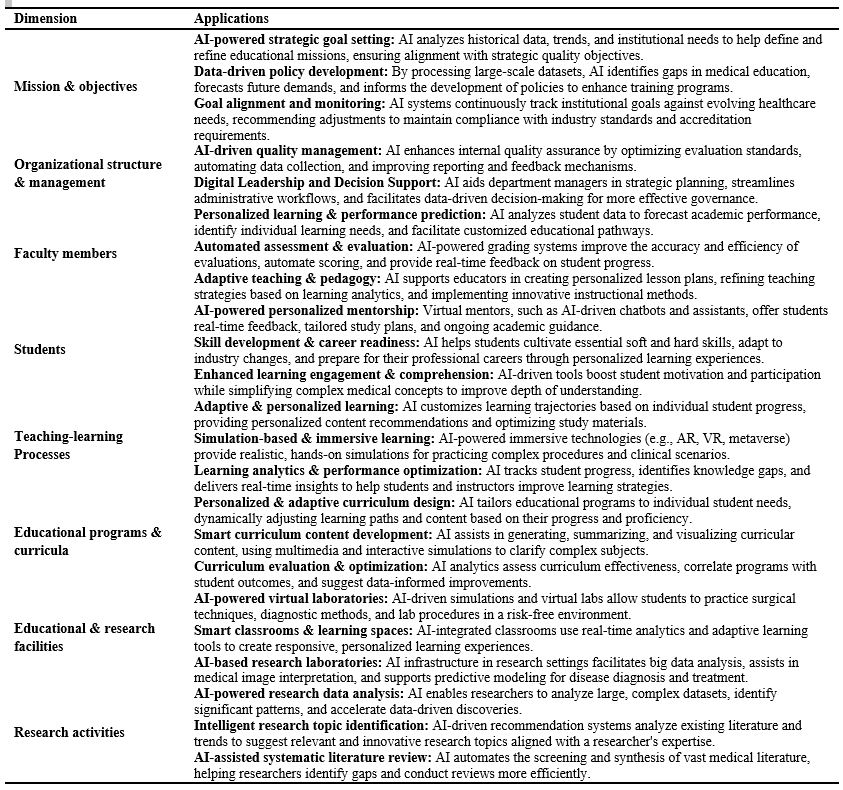
Table 4: Applications of Artificial Intelligence (AI) for enhancing quality in medical education
The frequency of references to different aspects of quality assessment in medical education, as indicated by the data in the table, stresses the significance and precedence of each aspect in related research. Teaching-learning processes (36 references) and faculty members (38 references) are given the highest priority, highlighting the critical roles that creative learning strategies, teaching approaches, and faculty engagement play in determining the quality of education. These results highlight the value of AI tools and cutting-edge technologies in improving the teaching and learning processes. 32 of the included studies made reference to the students dimension, and 34 references to organizational structure and management show that they actively take part in creating and carrying out successful educational initiatives. The development of data-driven strategies and effective resource management targeted at ongoing quality improvement in medical education are supported by highlighting these dimensions.
However, dimensions like Mission and Objectives and Research Activities—of which there are only eight—seem to be less closely looked at in the studies. The intricacy of assessing these aspects or a stronger emphasis on more realistic and concrete aspects could be the cause of this. Additionally, educational programs and curricula (21 times) and educational and research facilities (14 times) show how infrastructure and curriculum design quality directly affect the quality of the learning experience.
In order to guarantee a more uniform improvement in the quality of education, this frequency distribution pattern emphasizes the necessity of giving different aspects equal attention, with a special emphasis on the development of infrastructure and research initiatives. The frequency of each dimension is shown in the bar chart that follows (Figure 3).
In Table 4, examples of AI applications in enhancing the quality of medical education are presented, categorized according to each dimension of the framework.
Figure 3. Column chart of the dimensions of the framework used
Discussion
Higher education is predicted to experience even more significant changes as a result of artificial intelligence's revolution in educational systems [79]. Quality, which has always been central to academic thinking, is still a crucial tenet. Using standardized criteria that are frequently used in the medical field for rigorous evaluation, this study methodically investigated how AI can improve the caliber of medical education. In the second dimension, organizational management and structure, AI demonstrates extensive applications in strengthening university governance. Bhaskar et al. [88] highlights blockchain’s unique capacity to introduce efficiency and transparency, while Balayan et al. [89] shows AI’s utility in monitoring student enrollment and graduation. These tools support administrators in data-driven decision-making, process organization, and workflow optimization, ultimately enabling better utilization of resources [90]. AI also enhances human resource management through automation and optimization, reengineering recruitment, training, performance appraisal, career planning, and employee mobility [91, 92]. Universities can also forecast revenues and expenditures, improving the precision of budgets and association of allocation of resources with educational quality. AI therefore significantly enhances management and organizational systems, resulting in improved academic performance. These results are congruent with research [42, 44–48, 51, 53, 57–61, 64, 67, 68, 71, 74–76]. Empirical evidence exists for these results: Zabol University of Medical Sciences in Iran reported an adequate status in organizational structure [93], as did the University of Qom in Iran, which scored a mean of 2.11 and reflected positive assessment of educational quality [94]. These results indicate that there is a strong influence of effective governance, stable institutions, and institutional leadership on quality improvement. Further, AI automates routine tasks like admissions, whereby chatbots offer continuous support, decrease workload for staff, and increase efficiency [95–98]. In the third aspect, faculty members, AI has extensive applications to improve the quality of scholarly and teaching work. A significant contribution is reducing labor in grading, increasing efficiency and accuracy [98]. Professors utilizing AI technologies gain immensely in terms of providing extra examples, individualizing instruction, and improving materials [99]. Chan and Tsi [100] mention that AI tools improve teaching practice and provide instant feedback, hence instructional design increases. By analyzing students’ learning patterns, strengths, and weaknesses, AI enables individualized, data-driven instruction [101]. These findings are supported by extensive previous studies [39–70]. Empirical findings support these advantages: students of Yazd University of Medical Sciences indicated high levels of satisfaction with the punctuality of teachers and dedication of time [102], and Tehran University of Medical Sciences also reported positive results [103]. Conversely, in Tehran e-learning, the interaction between faculty and students was unsatisfactory (45% satisfaction) [104], and at Mashhad University, both interaction and feedback were unsatisfactory [105]. These conflicting results point towards variability in faculty communication and interaction, especially in online environments. AI allows faculty to save time for routine tasks such as attendance and grading, freeing time for course design [106]. Moreover, AI plans out lesson planning, syllabus creation, exams, tests, and rubrics [107]. Intensive technology such as image recognition and prediction systems increases assessment accuracy and effectiveness, decreasing test development, grading, and performance analysis [108].
In the fourth dimension—students—AI technologies are extensively used to significantly enhance the quality of learning. Chen et al. [109] summarize that chatbots are conversational interactive systems with the capacity to educate primary concepts and dispense instructional material. Similarly, Su et al. [110] demonstrate that AI allows one-on-one real-time support in e-learning, thereby enhancing the performance and participation of students. AI technologies simplify hard things, help students with disabilities, and promote inclusive learning [111]. According to Robert et al. [112], AI personalizes materials and feedback based on individual needs and learning styles, thereby creating adaptive learning environments. The collection of technologies as a whole improves learning through providing personalized experiences. There is proof that AI has very strong positive impact on quality and attainment of learning, in accordance with previous research studies [39, 41, 42, 45–72]. Empirical findings vary by institution: at Isfahan University of Medical Sciences, the student factor received a low score in comparison to other categories [113], while at Hamedan University, it received a high score [114]. These contradictory findings show how context-dependent student-related factors are, affected by learning environments, support services, and institution culture. Remarkably, student perceptions remain critical to complete assessments of education quality. AI systems provide tailored feedback, pinpoint weaknesses, and recommend targeted interventions for improvement [115]. In addition, algorithms for machine learning and neural networks promote autonomous learning by recognizing latent patterns in data and adapting continually from experience, facilitating dynamic and self-adjusting learning [116]. Apart from individuals, AI also assesses group performance, classroom relationships, and collective behavior, dealing with affective and social dimensions of learning. Through the promotion of teamwork, motivation, and communication, AI reinforces both individual and collective quality of learning [117].
In the fifth dimension, teaching–learning procedures, AI really adds quality to education by identifying students' learning habits and making customized recommendations for academic improvement. These technologies make classroom learning settings more flexible, responsive, and effective [118]. Passaic et al. [119] emphasize that augmented and virtual reality, learning games, and other AI offerings provide students with new and engaging experiences. Zhai et al. [120] confirm that AI automates testing and delivers timely feedback, boosting student performance, while Crawford et al. [121] show that tools such as ChatGPT foster interactive learning environments. Mislevy et al. [122] highlight the necessity of adaptive instruction, a central advantage of AI, enabling education tailored to students’ intellectual abilities. Collectively, these findings demonstrate AI’s broad utility in advancing teaching–learning quality, consistent with prior studies [38–75]. These claims are backed by Iranian university empirical data: 76% of the medical students at Isfahan University of Medical Sciences expressed satisfaction with the teaching process [123], and Guilan University was also satisfied [124]. The teaching process, however, indicated the highest variance between desired and experienced quality at Urmia University [125] and reflected institutional variations in teaching procedures. While some universities have well-coordinated student strategies, others struggle to align targeted quality goals with insights gained from experience. For digital natives, new interactive technologies significantly enhance motivation [126]. Virtual reality offers experience-derived learning environment that replicates real-world conditions [127]. AI also supports adaptive learning using data mining, intelligent tutoring, learning analytics, and real-time individualization. Gamification, another AI-supported technology, increases engagement by enabling real-time adaptation of game mechanics to students’ values, needs, and performance [128]. Augmented reality, particularly in anatomy and radiology, helps students better grasp complex concepts from the early years of study [129].
In the sixth dimension, curricula and training programs, AI-based personalization has arrived as a revolutionary method in medical education. Learning analytics determine students' areas of strength and weakness in order to create personalized learning paths that modify practice, study plans, content, and simulation-based evaluation to meet individual needs. The innovations improve professional preparedness for clinical settings, decrease burnout, and streamline efficiency. Curriculum visualization tools, such as diagrams, concept maps, and charts tracking progress, create unified perspectives on content, goals, and tests. These, along with AI, become dynamic, real-time updating relative to performance, alerting, and suggesting personalized routes of self-regulation. This is in line with previous studies [38–40, 43, 46, 48–50, 51, 53, 55–57, 59, 62, 64–68]. Besides, the convergence of AI and big data has also opened up new promises of large-scale learning analytics, promoting reform and enhancing curriculum quality [130]. AI-informed insights direct curriculum planning that aligns student needs with labor market and future health care demand requirements [131].
At the seventh dimension, research and education facilities, infrastructural development is one of the key drivers to the quality of education. Among the best applications of AI is the concept of smart campuses, which integrates intelligent systems such as ICT infrastructure, intelligent sensors, autonomous control, prophylactic care, and sustainability to deliver harmonized and efficient learning environments [132]. These campuses leverage high-performance cloud computing and Internet of Things (IoT) to facilitate collaboration, security, and adaptive services in higher education [133]. Upgrading software and hardware infrastructures enables innovation and uptake of modern learning technologies consistent with findings from earlier studies [38, 41, 48, 49, 52, 54, 56–58, 70–73]. Empirical evidence indicates differences, however: Behbahan University of Medical Sciences cited infrastructural shortages as a key factor in decreasing educational quality [134], as did Hamedan University, who also recorded poor performance here [135]. Yasouj University, however, assessed its equipment in the laboratory—an essential infrastructural component—very satisfactory [136]. Such variations are indicative of the difference in infrastructural provision, with direct consequence for perceived and actual educational quality. Artificial Intelligence-based Learning Management Systems (LMS) like Absorb LMS and Docebo enhance learning efficiency with intelligent content development, administrative automation, and personalized pathways [137]. The broader concept of smart campuses positions AI in the middle of creating adaptive, data-driven, and student-centered environments. AI delivers academic and administrative services more accurately and efficiently through predictive analytics and adaptive services [8]. In the eighth dimension—research activities—AI has significant potential to support and transform university research. Although still maturing, AI technologies, particularly no-code platforms, can transform research design and implementation [138]. AI software aids the researcher by rapidly reviewing and summarizing literature, generating short summaries, organizing references, and refining manuscript writing [139]. Tools such as ChatGPT provide personalized feedback, and thus scholars improve in writing, creating insights, and improving the quality of the work [140]. Specifically, ChatGPT helps clinical researchers in drafting literature reviews, abstracts, references, and even draft versions of the manuscript [141]. These benefits align in consistency with previous results [44, 49, 55, 60, 66, 69, 70, 72]. Evidence by Sabzevar University of Medical Sciences is also in support that research work was considered desirable in internal quality evaluations [142], calling for the integration of research productivity into instruction structures. By coming up with concepts, posing research questions, and identifying keywords, AI also aids in the development of research problems [143]. Furthermore, sophisticated language models enhance readability, fix grammatical mistakes, expand vocabulary, and fortify syntax, freeing up researchers to concentrate on analytical and experimental tasks. Additionally, these technologies facilitate more logical and fact-based communication by assisting non-native English speakers in overcoming language barriers [144]. Beyond writing, AI also enhances data gathering, examination, and inter-disciplinary coordination by acting as recommendation systems that suggest to researchers pertinent areas of research across a wide variety of subjects [145–147].
Conclusion
With the advent of AI, decision-makers and policymakers should maximize its potential to further enhance educational quality. These results need to be used continuously to develop interventions to improve educational quality with systems thinking and understanding. Quality is not a static state; it is an ever-changing and evolving entity. All organizational elements, from culture, a directional and so-called soft capability, through to governance and management frameworks, are involved and contributing to the quality movement. Without the involvement of all elements, significant improvements in educational quality are unrealistic. From a systems perspective, all components must work together—much like parts of a living entity—to enhance quality.
The purpose of this research was to gather, combine, and summarize the existing research in this subject using mixed methods research synthesis in order to obtain a general idea of the applications of AI to enhance educational quality.
Apart from methodological comprehensiveness and comprehensive coverage, this research is still exposed to some limitations.
The most important one is the use of only English-written peer-reviewed articles in the final selection. This language barrier may also lead to the exclusion of relevant studies that were published in other languages, particularly from non-English-speaking countries where AI application in medical education may be imminent but not well represented in international databases.
Furthermore, reliance on database-indexed literature may exclude thoughtful observations from grey literature, conference talks, or institutional reports not covered by mainstream systems.
Though Google Scholar was consulted to respond to this in part, it will not compensate for such potential omissions. These constraints suggest that the findings, while informative, may be English-dominant or Western-centric perception of the contribution of AI to medical education. The delimitation to this research is the exclusion of grey literature, i.e., unofficial and non-academic sources such as organizational documents, theses, conference papers, government documents, etc. that are not typically formally published or are not widely accessible.
Another limitation is the problem of updates; meta-syntheses tend to capture the prevailing situation at the time of research. The study needs to be updated frequently because of the rapid advancements in fields like artificial intelligence. It is noteworthy that future research should pay more attention to the operational aspects (faculty roles, teaching-learning processes) than the strategic ones (research and mission).
Ethical considerations
This study did not use primary data from either human or animal participants; rather, it is a mixed methods research synthesis of previously published research. Therefore, no institutional review board (IRB) code or ethical approval was needed. To maintain academic integrity, all included studies were openly accessible and properly referenced.
Artificial intelligence utilization for article writing
The authors would like to express their profound appreciation to the colleagues who helped with this study's quality assessment and consensus-building phases, offering an impartial check and assisting in the resolution of disagreements.
The research process was substantially enhanced by their insightful remarks and collaborative input. CahtGPT-4 used to improve the organization and clarity of expression prior to submission. The authors are solely responsible for the final content and have carefully reviewed, edited, and approved all outputs produced with the help of this tool.
Acknowledgment
We are deeply grateful to Dr. Chenxi Liu, a PhD candidate in Learning Technologies at Stanford University School of Medicine, for her helpful and perceptive criticism, which significantly improved the manuscript's overall quality, rigor, and clarity.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Author contributions
AK led the conceptualization and had the primary role in developing the manuscript.
FD was responsible for the collection and organization of references.
RK contributed to the structural review and refinement of the manuscript. RM conducted the final review and provided critical revisions.
Funding
No specific grant from a public, private, or nonprofit funding organization was obtained for this study.
Data availability statement
All data analyzed in this study are available in publicly accessible databases.
Background & Objective: Academic systems are among the many spheres of human life highly influenced by artificial intelligence (AI). The idea of quality in medical education is changing as a result of AI-driven developments, creating both opportunities and difficulties. The purpose of this study is to investigate how AI might be used to improve the quality of medical education.
Materials & Methods: Mixed methods research synthesis was the approach taken. Relevant studies published in Science Direct, Springer, ERIC, Emerald, Sage Journals, Wiley Online Library, PubMed, and Google Scholar between 2015 and 2025 were found using targeted search terms. Quality was assessed through the Mixed Methods Appraisal Tool (MMAT) and selection process followed Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The final review included 49 studies that met the criteria. A model with eight dimensions of the quality of medical education was employed to analyze the data.
Results: The results were grouped into eight categories: mission and goals, organizational structure and governance, faculty members, students, teaching and learning processes, curricula, facilities, and research activities. AI was found to have a positive effect on all areas, with the most focus on faculty members (38 citations) and teaching-learning processes (36 citations). It was found that these themes were very important for making education better. By comparison, mission and objectives, and research activities received little reference (8 references each), indicating strategic and research-focused AI integration lacunae.
Conclusion: AI has the most potential to change how medical education is taught by using new teaching tools, better lesson plans, and personalized learning. But the fact that research and planning dimensions don't cover everything shows how important it is to do research and make policies with clear, well-defined goals. Balanced implementation of AI in all dimensions of quality is needed to bring sustainable and comprehensive transformations in medical education. The current study offers significant implications to educators, policymakers, and researchers for guiding AI-supported education reforms in the future.
Introduction
Improving the quality of medical education has therefore become a priority for different stakeholders such as learners, teachers, patients, healthcare workers, regulatory agencies, and financiers [3]. To address this priority, quality in medical education has drawn significant scholarly attention as researchers seek to understand and maximize it amidst evolving health needs [4]. The quality of medical education is important beyond the academe since it is irrevocably entwined with the ability of health systems to deliver safe, effective, and equitable care. All stakeholders agree that without earnest dedication to the quality of medical education, quality improvements in healthcare delivery are not feasible [5]. High-quality medical education is characterized by well-structured educational systems, comprehensive curricula, qualified faculty, and enhanced teaching practices. Furthermore, medicine graduates need to attain a blend of soft skills, practical skills, and theory-based medical understanding [6]. However, "quality" is an aggregate and comparative term and is still challenging to define as there are multiple interpretations based on stakeholders' perceptions and standards [7]. Amidst rapidly evolving international trends shaping higher education today, quality has become increasingly critical. Universities are faced with complex issues with technological advancement accelerating, calling for adaptive interventions and revolutionary changes in their function as educators [8]. Artificial Intelligence (AI), a revolutionary technological innovation, also promises to enhance the quality of education in every discipline, including medical education. The application of AI—including intelligent tutoring systems, chatbots, adaptive learning platforms, automated grading, and learning analytics—enables individualized learning experiences, enhances teaching effectiveness, and streamlines academic administration [9-13]. In addition to its well-known applications in medical training, artificial intelligence is driving a wide range of innovations across the broader field of medicine. For instance, personalized medicine has been developed with the aim of providing drugs based on the individual characteristics of patients [14]. In addition to its well-known applications in medical training, artificial intelligence is driving a wide range of innovations across the broader field of medicine [15]. Yet another key focus area is the early diagnosis of various diseases, which results in improved prevention and reduced costs of treatment [16]. Also, advances in medical imaging have provided improved analysis of radiological data, thereby improving diagnostic efficiency [17]. In medical care, AI has proven to be an effective tool for patient monitoring and surveillance [18], while clinical decision-support systems have enhanced diagnostic and therapeutic processes [19].
Medical data management has also been streamlined through advanced algorithms, enabling the analysis of large-scale health datasets [20]. In addition, genome analysis and genetic medicine have opened new pathways for treatments based on patients’ genetic profiles [21]. Virtual medical consultations and AI-driven assistants have also played a substantial role in improving patient engagement and expanding access to healthcare services [22]. Finally, AI has contributed to optimizing therapeutic processes and improving the overall efficiency of healthcare systems [23]. Despite this potential, the integration of AI into education presents several challenges. Some of these are the danger of relying too much on AI tools, which could hurt academic standards, worries about student data privacy, and the possibility of biases being built into AI platforms through algorithms that reflect human biases [24, 25]. Therefore, AI should not be regarded as a universal remedy, but rather as a supportive instrument whose efficacy is contingent upon the establishment of suitable safeguards. Current studies underscore these dual facets of AI in education. Kabudi [26] identifies critical areas such as educator roles, support for special-needs students, racial and data bias in AI-based learning systems, and commercialization challenges. Flores-Viva and García-Peñalvo [27] emphasize ethical considerations in AI’s educational applications. Nkechi et al. [28] show how AI can help close the digital divide and overcome language barriers to make education more equal. Ajani et al. [29] talk about how AI can help with personalized learning, better teaching methods, and more efficient administration. They also talk about privacy and ethical issues. AlSagri and Sohail [30] argue that deeper understanding of AI capabilities can inform policies fostering equitable and sustainable education systems. This study employs a mixed methods research synthesis approach to address international research gaps regarding AI’s role in improving education quality, with a novel focus on medical education. The results give a broad, worldwide view of how AI could improve the quality of medical education. This study helps close the knowledge gap by giving educators, policymakers, and researchers who want to use AI to improve the quality of medical education useful information. This study adheres to the most prevalent framework for evaluating the intrinsic quality of university teaching [31–35]. There are eight principal dimensions in the conceptual model: Mission and Objectives, Organizational Structure and Management, Faculty Members and Students, Teaching-Learning Processes, Educational Programs and Curricula, Educational and Research Facilities, and Research Activities.
Materials & Methods
Design and setting(s)
Since both quantitative and qualitative studies, as well as those employing mixed-method research designs, are available for examining the applications of artificial intelligence in quality of medical education, we chose an integrated Mixed-Methods Research Synthesis (MMRS) design as the methodological framework for our review. A mixed-methods research synthesis is a form of systematic review that applies the principles of mixed-methods inquiry. In essence, such a study is expected not only to include two distinct strands—one qualitative and one quantitative—each with its own questions, data, analyses, and conclusions—but also to integrate, link, or connect these strands in a meaningful way [36]. Specifically, we adopted the MMRS framework developed by Heyvaert and colleagues [37]. A diagrammatic overview of this framework can be found in Figure 1. Considering the multidimensional complexity of artificial intelligence applications quality of medical education, it seems essential to employ a mixed-methods approach in the synthesis of the studies (Figure 1). Quantitative studies primarily seek to investigate the effectiveness of AI tools by measuring the performance improvement of learners, or system accuracy, while qualitative studies evaluate attitudes, experiences, and ethical and educational dilemmas with the implementation of this technology. A synthesis of these two types of data provides a richer understanding of the phenomenon. On one hand, quantitative data provide empirical and objective evidence about efficiency and outcomes; on the other hand, qualitative data primarily offer enhanced insights into the contexts, meanings, and processes associated with the use of AI in quality of medical education. In a methodological sense, a mixed synthesis approach is especially relevant for publishing the synthesis or results of qualitative and quantitative studies, as it allows for interpretation of these diverse findings within a unifying framework. In this manuscript, and as shown in Figure 1, data from the base qualitative and quantitative studies were first synthesized in their separate studies. In the last stage, through an integrative synthesis, similarities, differences, and complementarity across the two strands were assessed. The framework provides a six-stage process [37], and subsequent sections of this report describe the process we undertook for each of the particular six stages of this study.
Figure 1. Qualitative, quantitative, and mixed methods research synthesis
The problem identification and question formulation stage
The development of a review protocol and the literature search
The study protocol was crafted to facilitate mixed methods research synthesis MMRS framework regarding the utilization of AI in the enhancement of medical education quality. The creation of the protocol needed multiple steps: crafting the research question and study objectives; choosing a conceptual framework; setting up inclusion and exclusion criteria; devising the search strategy and resource retrieval techniques; delineating the screening and selection process for studies; choosing tools to evaluate study quality; deciding on the data analysis method; and validating and confirming the results. We did a systematic search of the literature for peer-reviewed articles that were published in English between 2015 and 2025. This decade was chosen to include the era of large progress in machine learning, deep learning, and natural language processing, which have become essential in revolutionizing educational assessment and improving quality. The electronic databases Science Direct, Springer, ERIC, Emerald, Sage Journals, Wiley Online Library, PubMed, and Google Scholar were all searched. With an emphasis on (O) Quality Improvement, the search strategy combined keywords associated with (I) Artificial Intelligence and (P) Medical Education in a Boolean query based on the PICO framework. For every database, the search string
was modified. Below is a representative example: An example of a search query is: ("artificial intelligence" OR AI OR "machine learning" OR chatbot*). AND ("clinical training" OR "medical student*" OR "medical education") AND ("learning outcome*" OR "educational quality" OR "quality improvement")
The following standards served as a guide for choosing the study: Criteria for inclusion: publications from 2015–2025 that are peer-reviewed in English, specifically address AI applications in medical education, and use either mixed-methods, quantitative, or qualitative research.
Exclusion criteria include: studies done outside of the designated time frame; editorials, opinion pieces, and non-peer-reviewed literature; and articles that do not focus on improving educational quality.
Look at the selection procedure: As shown in Figure 2, the PRISMA guidelines were followed during the study selection process. 187 records were found in the first database search. 77 studies were excluded after the titles and abstracts of these records were screened and duplicates were removed. After abstract review, 43 of the 110 remaining studies were eliminated. Following a full-text evaluation of the 67 studies that were found, 18 articles that did not fit the inclusion criteria were eliminated.
The MMAT (Mixed Methods Appraisal Tool, 2018 version) was adopted to assess the quality of the methodological approach of all the studies included in this synthesis. Each study was reviewed based on five criteria followed by a score of between zero to five. The criteria cut-off was defined to be any study that scored three or above, which is demonstrative of a compromise between quality and feasibility. Lower scores indicate methodological concerns with confidence and an increased risk of bias which may affect confidence in the findings from this synthesis.
As such a score of three or above is the minimum standard of quality and validity to avoid studies that demonstrate methodological concerns from being included in the synthesis. The MMAT scores for studies included in this synthesis are shown in Table 1.
Figure 2. PRISMA flowchart for screening the articles
Table 1. Bibliography of the selected articles
The selection of an appropriate design and method
The third phase of this investigation selected the mixed content analysis approach as the primary analytical lens in order to determine the appropriate synthesis design and method.
The goal of the research is to achieve an in-depth understanding of the uses of artificial intelligence in medical education through the integration of quantitative and qualitative evidence, and as such, content analysis offers a mechanism by which to provide shared meaning units to represent the diverse findings of primary studies, and identify categories and themes from the units.
Further, within this methodological approach, data from quantitative studies have also been transformed into classizable units of meaning via content-based extraction and description—for example, by identifying indicators, variables, statistical findings or evidence statements—that can also be analyzed alongside qualitative findings. This methodological approach design has constituted a synthesis that is grounded in meaning and content as opposed to data type, thus generating a coherent and multi-faceted account of applications of artificial intelligence in the quality of medical education.
The data extraction and evaluation stage
The articles' texts were read several times to help readers become fully immersed in the content before the data was extracted.
Key sections of the articles were documented in a structured format using Microsoft Word. For identifying key concepts—those conveying the most significant meanings—the paragraph was utilized as the unit of analysis, from which the most critical concepts were extracted.
Throughout the analysis process, memos were employed extensively.
During the initial reading of the texts, researchers made notes on key points, trends, or potential connections.
The notes included preliminary impressions of the focal issues of the articles, key ideas related to the research issue, and emerging ideas or issues worth investigating.
During coding, memos aided the recording of the rationale for why the codes were chosen, meaning-making, and interconnection, thus promoting conversation among the researchers.
In later data organization and extraction, memos proved helpful to aid the research team to compile suitable codes to create categories and overall themes. Examples of how to extract codes are shown in Table 2.
Table 2. Examples of how to extract codes
The data analysis and interpretation stage
We followed Elo and Kyngas [77] This framework for examining information is built upon three foundational pillars. The initial stage focuses on establishing a foundation, where information is gathered and a structure for categorization is defined.
The subsequent stage, concerned with systematic arrangement, involves a meticulous review and sorting of the data based on its alignment with pre-established classifications. The final and culminating stage is dedicated to presenting the outcomes, which articulates the findings to enable a deeper understanding of the identified patterns. Furthermore, the insights derived from this process can be significantly augmented by integrating a mixed-methods approach that incorporates both statistical and interpretive techniques. To ensure consistency, the concepts derived from each classification session were compared to measure the degree of agreement between the two coding processes. The process involved labeling similar codes across the two-time intervals as "agreement" and dissimilar codes as "disagreement." The frequency of agreements and disagreements was then used in a formula to calculate the reliability of the coding process over time. This study conducted coding and classification twice, with a 14-day interval between sessions. A total of 403 concepts were extracted, with agreement reached on 175 of them between the two coding sessions. The calculated reliability for this retest was 86%, which, since it exceeds the 60% threshold, confirms the reliability of the coding process [78].
The reporting and discussing of research findings
Finally, the findings were systematically documented and shared, ensuring a comprehensive and rigorous analysis process.
Results
As stated earlier, we used a standardized framework for quality assessment, which has been widely accepted in many studies, as a standard by which to measure the caliber of medical education. To ensure alignment with this framework, key concepts were extracted and then categorized according to their similarities and differences. Mission and objectives, organizational structure and management, faculty, students, teaching-learning processes, educational programs and curricula, academic and research facilities, and research activities are the eight primary dimensions that make up the framework. Within this framework, the integrated key concepts were taken into consideration as criteria. The departmental goals and missions are covered by the Mission and Objectives dimension. Academic departments' organizational setup, including policies, staffing levels, and services, is covered by the Organizational Structure and Management dimension. Academic counseling, consultation accessibility, and faculty-student interactions are all included in the Faculty Members dimension. The Students dimension covers student activities like participation in departmental planning, awareness of departmental goals, and knowledge of their rights and responsibilities.
Additionally, teaching and learning strategies, technology integration, and student assessment procedures are all included in the Instruction-Learning Processes dimension. The academic programs themselves, including their alignment with departmental missions and their design in accordance with curriculum planning principles, are covered by the Educational Programs and Curricula dimension. The infrastructure and resources that are available, including libraries, information systems, and technological services, are covered by the Educational and Research Facilities dimension. Lastly, academic work done by both students and faculty is included in the Research Activities dimension. The analysis's specific results are shown in Tables 3 and 4.
Table 3: Analysis of findings based on the standard framework for assessing the quality of medical education
Table 4: Applications of Artificial Intelligence (AI) for enhancing quality in medical education
The frequency of references to different aspects of quality assessment in medical education, as indicated by the data in the table, stresses the significance and precedence of each aspect in related research. Teaching-learning processes (36 references) and faculty members (38 references) are given the highest priority, highlighting the critical roles that creative learning strategies, teaching approaches, and faculty engagement play in determining the quality of education. These results highlight the value of AI tools and cutting-edge technologies in improving the teaching and learning processes. 32 of the included studies made reference to the students dimension, and 34 references to organizational structure and management show that they actively take part in creating and carrying out successful educational initiatives. The development of data-driven strategies and effective resource management targeted at ongoing quality improvement in medical education are supported by highlighting these dimensions.
However, dimensions like Mission and Objectives and Research Activities—of which there are only eight—seem to be less closely looked at in the studies. The intricacy of assessing these aspects or a stronger emphasis on more realistic and concrete aspects could be the cause of this. Additionally, educational programs and curricula (21 times) and educational and research facilities (14 times) show how infrastructure and curriculum design quality directly affect the quality of the learning experience.
In order to guarantee a more uniform improvement in the quality of education, this frequency distribution pattern emphasizes the necessity of giving different aspects equal attention, with a special emphasis on the development of infrastructure and research initiatives. The frequency of each dimension is shown in the bar chart that follows (Figure 3).
In Table 4, examples of AI applications in enhancing the quality of medical education are presented, categorized according to each dimension of the framework.
Figure 3. Column chart of the dimensions of the framework used
Discussion
Higher education is predicted to experience even more significant changes as a result of artificial intelligence's revolution in educational systems [79]. Quality, which has always been central to academic thinking, is still a crucial tenet. Using standardized criteria that are frequently used in the medical field for rigorous evaluation, this study methodically investigated how AI can improve the caliber of medical education. In the second dimension, organizational management and structure, AI demonstrates extensive applications in strengthening university governance. Bhaskar et al. [88] highlights blockchain’s unique capacity to introduce efficiency and transparency, while Balayan et al. [89] shows AI’s utility in monitoring student enrollment and graduation. These tools support administrators in data-driven decision-making, process organization, and workflow optimization, ultimately enabling better utilization of resources [90]. AI also enhances human resource management through automation and optimization, reengineering recruitment, training, performance appraisal, career planning, and employee mobility [91, 92]. Universities can also forecast revenues and expenditures, improving the precision of budgets and association of allocation of resources with educational quality. AI therefore significantly enhances management and organizational systems, resulting in improved academic performance. These results are congruent with research [42, 44–48, 51, 53, 57–61, 64, 67, 68, 71, 74–76]. Empirical evidence exists for these results: Zabol University of Medical Sciences in Iran reported an adequate status in organizational structure [93], as did the University of Qom in Iran, which scored a mean of 2.11 and reflected positive assessment of educational quality [94]. These results indicate that there is a strong influence of effective governance, stable institutions, and institutional leadership on quality improvement. Further, AI automates routine tasks like admissions, whereby chatbots offer continuous support, decrease workload for staff, and increase efficiency [95–98]. In the third aspect, faculty members, AI has extensive applications to improve the quality of scholarly and teaching work. A significant contribution is reducing labor in grading, increasing efficiency and accuracy [98]. Professors utilizing AI technologies gain immensely in terms of providing extra examples, individualizing instruction, and improving materials [99]. Chan and Tsi [100] mention that AI tools improve teaching practice and provide instant feedback, hence instructional design increases. By analyzing students’ learning patterns, strengths, and weaknesses, AI enables individualized, data-driven instruction [101]. These findings are supported by extensive previous studies [39–70]. Empirical findings support these advantages: students of Yazd University of Medical Sciences indicated high levels of satisfaction with the punctuality of teachers and dedication of time [102], and Tehran University of Medical Sciences also reported positive results [103]. Conversely, in Tehran e-learning, the interaction between faculty and students was unsatisfactory (45% satisfaction) [104], and at Mashhad University, both interaction and feedback were unsatisfactory [105]. These conflicting results point towards variability in faculty communication and interaction, especially in online environments. AI allows faculty to save time for routine tasks such as attendance and grading, freeing time for course design [106]. Moreover, AI plans out lesson planning, syllabus creation, exams, tests, and rubrics [107]. Intensive technology such as image recognition and prediction systems increases assessment accuracy and effectiveness, decreasing test development, grading, and performance analysis [108].
In the fourth dimension—students—AI technologies are extensively used to significantly enhance the quality of learning. Chen et al. [109] summarize that chatbots are conversational interactive systems with the capacity to educate primary concepts and dispense instructional material. Similarly, Su et al. [110] demonstrate that AI allows one-on-one real-time support in e-learning, thereby enhancing the performance and participation of students. AI technologies simplify hard things, help students with disabilities, and promote inclusive learning [111]. According to Robert et al. [112], AI personalizes materials and feedback based on individual needs and learning styles, thereby creating adaptive learning environments. The collection of technologies as a whole improves learning through providing personalized experiences. There is proof that AI has very strong positive impact on quality and attainment of learning, in accordance with previous research studies [39, 41, 42, 45–72]. Empirical findings vary by institution: at Isfahan University of Medical Sciences, the student factor received a low score in comparison to other categories [113], while at Hamedan University, it received a high score [114]. These contradictory findings show how context-dependent student-related factors are, affected by learning environments, support services, and institution culture. Remarkably, student perceptions remain critical to complete assessments of education quality. AI systems provide tailored feedback, pinpoint weaknesses, and recommend targeted interventions for improvement [115]. In addition, algorithms for machine learning and neural networks promote autonomous learning by recognizing latent patterns in data and adapting continually from experience, facilitating dynamic and self-adjusting learning [116]. Apart from individuals, AI also assesses group performance, classroom relationships, and collective behavior, dealing with affective and social dimensions of learning. Through the promotion of teamwork, motivation, and communication, AI reinforces both individual and collective quality of learning [117].
In the fifth dimension, teaching–learning procedures, AI really adds quality to education by identifying students' learning habits and making customized recommendations for academic improvement. These technologies make classroom learning settings more flexible, responsive, and effective [118]. Passaic et al. [119] emphasize that augmented and virtual reality, learning games, and other AI offerings provide students with new and engaging experiences. Zhai et al. [120] confirm that AI automates testing and delivers timely feedback, boosting student performance, while Crawford et al. [121] show that tools such as ChatGPT foster interactive learning environments. Mislevy et al. [122] highlight the necessity of adaptive instruction, a central advantage of AI, enabling education tailored to students’ intellectual abilities. Collectively, these findings demonstrate AI’s broad utility in advancing teaching–learning quality, consistent with prior studies [38–75]. These claims are backed by Iranian university empirical data: 76% of the medical students at Isfahan University of Medical Sciences expressed satisfaction with the teaching process [123], and Guilan University was also satisfied [124]. The teaching process, however, indicated the highest variance between desired and experienced quality at Urmia University [125] and reflected institutional variations in teaching procedures. While some universities have well-coordinated student strategies, others struggle to align targeted quality goals with insights gained from experience. For digital natives, new interactive technologies significantly enhance motivation [126]. Virtual reality offers experience-derived learning environment that replicates real-world conditions [127]. AI also supports adaptive learning using data mining, intelligent tutoring, learning analytics, and real-time individualization. Gamification, another AI-supported technology, increases engagement by enabling real-time adaptation of game mechanics to students’ values, needs, and performance [128]. Augmented reality, particularly in anatomy and radiology, helps students better grasp complex concepts from the early years of study [129].
In the sixth dimension, curricula and training programs, AI-based personalization has arrived as a revolutionary method in medical education. Learning analytics determine students' areas of strength and weakness in order to create personalized learning paths that modify practice, study plans, content, and simulation-based evaluation to meet individual needs. The innovations improve professional preparedness for clinical settings, decrease burnout, and streamline efficiency. Curriculum visualization tools, such as diagrams, concept maps, and charts tracking progress, create unified perspectives on content, goals, and tests. These, along with AI, become dynamic, real-time updating relative to performance, alerting, and suggesting personalized routes of self-regulation. This is in line with previous studies [38–40, 43, 46, 48–50, 51, 53, 55–57, 59, 62, 64–68]. Besides, the convergence of AI and big data has also opened up new promises of large-scale learning analytics, promoting reform and enhancing curriculum quality [130]. AI-informed insights direct curriculum planning that aligns student needs with labor market and future health care demand requirements [131].
At the seventh dimension, research and education facilities, infrastructural development is one of the key drivers to the quality of education. Among the best applications of AI is the concept of smart campuses, which integrates intelligent systems such as ICT infrastructure, intelligent sensors, autonomous control, prophylactic care, and sustainability to deliver harmonized and efficient learning environments [132]. These campuses leverage high-performance cloud computing and Internet of Things (IoT) to facilitate collaboration, security, and adaptive services in higher education [133]. Upgrading software and hardware infrastructures enables innovation and uptake of modern learning technologies consistent with findings from earlier studies [38, 41, 48, 49, 52, 54, 56–58, 70–73]. Empirical evidence indicates differences, however: Behbahan University of Medical Sciences cited infrastructural shortages as a key factor in decreasing educational quality [134], as did Hamedan University, who also recorded poor performance here [135]. Yasouj University, however, assessed its equipment in the laboratory—an essential infrastructural component—very satisfactory [136]. Such variations are indicative of the difference in infrastructural provision, with direct consequence for perceived and actual educational quality. Artificial Intelligence-based Learning Management Systems (LMS) like Absorb LMS and Docebo enhance learning efficiency with intelligent content development, administrative automation, and personalized pathways [137]. The broader concept of smart campuses positions AI in the middle of creating adaptive, data-driven, and student-centered environments. AI delivers academic and administrative services more accurately and efficiently through predictive analytics and adaptive services [8]. In the eighth dimension—research activities—AI has significant potential to support and transform university research. Although still maturing, AI technologies, particularly no-code platforms, can transform research design and implementation [138]. AI software aids the researcher by rapidly reviewing and summarizing literature, generating short summaries, organizing references, and refining manuscript writing [139]. Tools such as ChatGPT provide personalized feedback, and thus scholars improve in writing, creating insights, and improving the quality of the work [140]. Specifically, ChatGPT helps clinical researchers in drafting literature reviews, abstracts, references, and even draft versions of the manuscript [141]. These benefits align in consistency with previous results [44, 49, 55, 60, 66, 69, 70, 72]. Evidence by Sabzevar University of Medical Sciences is also in support that research work was considered desirable in internal quality evaluations [142], calling for the integration of research productivity into instruction structures. By coming up with concepts, posing research questions, and identifying keywords, AI also aids in the development of research problems [143]. Furthermore, sophisticated language models enhance readability, fix grammatical mistakes, expand vocabulary, and fortify syntax, freeing up researchers to concentrate on analytical and experimental tasks. Additionally, these technologies facilitate more logical and fact-based communication by assisting non-native English speakers in overcoming language barriers [144]. Beyond writing, AI also enhances data gathering, examination, and inter-disciplinary coordination by acting as recommendation systems that suggest to researchers pertinent areas of research across a wide variety of subjects [145–147].
Conclusion
With the advent of AI, decision-makers and policymakers should maximize its potential to further enhance educational quality. These results need to be used continuously to develop interventions to improve educational quality with systems thinking and understanding. Quality is not a static state; it is an ever-changing and evolving entity. All organizational elements, from culture, a directional and so-called soft capability, through to governance and management frameworks, are involved and contributing to the quality movement. Without the involvement of all elements, significant improvements in educational quality are unrealistic. From a systems perspective, all components must work together—much like parts of a living entity—to enhance quality.
The purpose of this research was to gather, combine, and summarize the existing research in this subject using mixed methods research synthesis in order to obtain a general idea of the applications of AI to enhance educational quality.
Apart from methodological comprehensiveness and comprehensive coverage, this research is still exposed to some limitations.
The most important one is the use of only English-written peer-reviewed articles in the final selection. This language barrier may also lead to the exclusion of relevant studies that were published in other languages, particularly from non-English-speaking countries where AI application in medical education may be imminent but not well represented in international databases.
Furthermore, reliance on database-indexed literature may exclude thoughtful observations from grey literature, conference talks, or institutional reports not covered by mainstream systems.
Though Google Scholar was consulted to respond to this in part, it will not compensate for such potential omissions. These constraints suggest that the findings, while informative, may be English-dominant or Western-centric perception of the contribution of AI to medical education. The delimitation to this research is the exclusion of grey literature, i.e., unofficial and non-academic sources such as organizational documents, theses, conference papers, government documents, etc. that are not typically formally published or are not widely accessible.
Another limitation is the problem of updates; meta-syntheses tend to capture the prevailing situation at the time of research. The study needs to be updated frequently because of the rapid advancements in fields like artificial intelligence. It is noteworthy that future research should pay more attention to the operational aspects (faculty roles, teaching-learning processes) than the strategic ones (research and mission).
Ethical considerations
This study did not use primary data from either human or animal participants; rather, it is a mixed methods research synthesis of previously published research. Therefore, no institutional review board (IRB) code or ethical approval was needed. To maintain academic integrity, all included studies were openly accessible and properly referenced.
Artificial intelligence utilization for article writing
The authors would like to express their profound appreciation to the colleagues who helped with this study's quality assessment and consensus-building phases, offering an impartial check and assisting in the resolution of disagreements.
The research process was substantially enhanced by their insightful remarks and collaborative input. CahtGPT-4 used to improve the organization and clarity of expression prior to submission. The authors are solely responsible for the final content and have carefully reviewed, edited, and approved all outputs produced with the help of this tool.
Acknowledgment
We are deeply grateful to Dr. Chenxi Liu, a PhD candidate in Learning Technologies at Stanford University School of Medicine, for her helpful and perceptive criticism, which significantly improved the manuscript's overall quality, rigor, and clarity.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Author contributions
AK led the conceptualization and had the primary role in developing the manuscript.
FD was responsible for the collection and organization of references.
RK contributed to the structural review and refinement of the manuscript. RM conducted the final review and provided critical revisions.
Funding
No specific grant from a public, private, or nonprofit funding organization was obtained for this study.
Data availability statement
All data analyzed in this study are available in publicly accessible databases.
Article Type : Review |
Subject:
Medical Education
Received: 2025/05/13 | Accepted: 2025/10/26 | Published: 2025/11/19
Received: 2025/05/13 | Accepted: 2025/10/26 | Published: 2025/11/19
References
1. Khazaei Z, Ramezanzadeh K, Moodi M, Moradi M. Quality of clinical education from the viewpoints of students and interns in Birjand University of Medical Sciences. Future Med Educ J. 2012;2(1):22-6.
2. Gaikwad J, Bande V, Nikam L, Ghorpade M. Evaluation of quality of medical education services by students' perception based on SERVQUAL model: a cross-sectional study in Maharashtra, India. Int J Acad Med Pharm. 2022;4(4):590-5.
3. Jamieson S. State of the science: Quality improvement of medical curricula-How should we approach it?. Med Educ. 2023;57(1):49-56. [DOI:10.1111/medu.14912] [PMID] []
4. Hu X, Li J, Wang X, Guo K, Liu H, Yu Q, et al. Medical education challenges in Mainland China: an analysis of the application of problem-based learning. Med Teach. 2024;46(7):913-28.
5. Joshi MA. Quality assurance in medical education. Indian J Pharmacol. 2012;44(3):285-7. [DOI:10.4103/0253-7613.96295] [PMID] []
6. AlThukair D, Rattray J. What makes a high-quality medical education and graduate? The Saudi Arabia labor market's perspective. In: Halabi JK, Bissattini V, Massoud L, editors. Quality Assurance in Higher Education in the Middle East: Practices and Perspectives. Emerald Publishing Limited; 2023. p. 67-83. [DOI:10.1108/S2055-364120230000054004]
7. Keykha A, Ezati M, Khodayari Z. Identification of the barriers and factors affecting the quality of higher education in Allameh Tabataba'i university from the viewpoints of faculty members. Qual High Educ. 2022;28(3):326-44. [DOI:10.1080/13538322.2021.1968107]
8. Keykha A. Extraction and classification of smart university components to provide a conceptual framework: a meta-synthesis study. J Sci Tech Inf Manage. 2023;8(4):75-112.
9. Cooper G. Examining science education in ChatGPT: an exploratory study of generative artificial intelligence. J Sci Educ Technol. 2023;32(3):444-52. [DOI:10.1007/s10956-023-10039-y]
10. Tashtoush MA, Wardat Y, Aloufi F, Taani O. The effectiveness of teaching method based on the components of concept-rich instruction approach in students achievement on linear algebra course and their attitudes towards mathematics. J High Educ Theory Pract. 2022;22(7):41-57. [DOI:10.33423/jhetp.v22i7.5269]
11. Keykha A, Fazlali B, Behravesh S, Farahmandpour Z. Integrating artificial intelligence in medical education: a meta-synthesis of potentials and pitfalls of ChatGPT. J Adv Med Educ Prof. 2024;12(3):125-136.
12. Keykha A, Mohammadi H, Darabi F, Hosseini SS. Identifying the applications of artificial intelligence in the assessment of medical students. Strides Dev Med Educ. 2024;21(1):e140287.
13. Keykha A, Imanipour M, Shahrokhi J, Amiri M. The advantages and challenges of electronic exams: a qualitative research based on Shannon entropy technique. J Adv Med Educ Prof. 2025;13(1):1-10.
14. Ratiner K, Ciocan D, Abdeen SK, Elinav E. Utilization of the microbiome in personalized medicine. Nat Rev Microbiol. 2024;22(5):291-308. [DOI:10.1038/s41579-023-00998-9] [PMID]
15. Varghese C, Harrison EM, O'Grady G, Topol EJ. Artificial intelligence in surgery. Nat Med. 2024;30(5):1257-68. [DOI:10.1038/s41591-024-02970-3] [PMID]
16. Rabie AH, Saleh AI. Diseases diagnosis based on artificial intelligence and ensemble classification. Artif Intell Med. 2024;148:102753. [DOI:10.1016/j.artmed.2023.102753] [PMID]
17. Obuchowicz R, Strzelecki M, Piórkowski A. Clinical applications of artificial intelligence in medical imaging and image processing-a review. Cancers. 2024;16(10):1870. [DOI:10.3390/cancers16101870] [PMID] []
18. Shaik T, Tao X, Higgins N, Li L, Gururajan R, Zhou X, et al. Remote patient monitoring using artificial intelligence: current state, applications, and challenges. Wiley Interdiscip Rev Data Min Knowl Discov. 2023;13(2):e1485. [DOI:10.1002/widm.1485]
19. Ouanes K, Farhah N. Effectiveness of artificial intelligence (AI) in clinical decision support systems and care delivery. J Med Syst. 2024;48(1):74. [DOI:10.1007/s10916-024-02098-4] [PMID]
20. Musik S, Sasin-Kurowska J, Panczyk M. Bridging the past and future of clinical data management: the transformative impact of artificial intelligence. Open Access J Clin Trials. 2024;16:15-33. [DOI:10.2147/OAJCT.S509921]
21. Nagarajan R, Wang C, Walton D, Walton N. Artificial intelligence applications in genomics. Adv Mol Pathol. 2023;6:145-54. [DOI:10.1016/j.yamp.2024.08.001]
22. Thompson AE, Shaw T, Nott S, Wilson A, Saurman E. Patient and carer experiences of hospital‐based hybrid virtual medical care: a qualitative study. Med J Aust. 2024;221(11). [DOI:10.5694/mja2.52520]
23. Mirza M, Jabeen H, Fatima A. Artificial intelligence in digital therapeutics for optimized healthcare. J Pharma Insights Res. 2025;3(2):346-57. [DOI:10.69613/g5mbda64]
24. Hargreaves S. 'Words are flowing out like endless rain into a paper cup': ChatGPT & law school assessments. Leg Educ Rev. 2023;33:69. [DOI:10.53300/001c.83297]
25. Arrieta AB, Díaz-Rodríguez N, Del Ser J, Bennetot A, Tabik S, Barbado A, et al. Explainable Artificial Intelligence (XAI): Concepts, taxonomies, opportunities and challenges toward responsible AI. Inf Fusion. 2020;58:82-115. [DOI:10.1016/j.inffus.2019.12.012]
26. Kabudi TM. Artificial intelligence for quality education: successes and challenges for AI in meeting SDG4. In: Mikalef P, Pappas IO, Grønli TM, Krogstie J, editors. Responsible AI and Analytics for an Ethical and Inclusive Digitized Society. Cham: Springer International Publishing; 2022. p. 347-62. (Lecture Notes in Computer Science; vol. 13464).
27. Flores-Viva JM, García-Peñalvo FJ. Reflections on the ethics, potential, and challenges of artificial intelligence in the framework of quality education (SDG4). Comunicar. 2023;31(74):35-44. [DOI:10.3916/C74-2023-03]
28. Nkechi AA, Ojo AO, Eneh OA. Impact of artificial intelligence in achieving quality education. In: Mthembu NZ, editor. Artificial Intelligence and Education: Shaping the Future of Learning. Springer; 2024. p. 73-92.
29. Ajani OA, Gamede B, Matiyenga TC. Leveraging artificial intelligence to enhance teaching and learning in higher education: promoting quality education and critical engagement. J Pedagogical Sociol Psychol. 2024;7(1):54-69. [DOI:10.33902/JPSP.202528400]
30. AlSagri HS, Sohail SS. Evaluating the role of artificial intelligence in sustainable development goals with an emphasis on "quality education". Discov Sustain. 2024;5(1):118. [DOI:10.1007/s43621-024-00682-9]
31. Yarmohammadian MH, Kalbasi A. Internal evaluation of departments in the school of management and medical informatics, Isfahan University of Medical Science. Iran J Med Educ. 2006;6(1):125-34.
32. Sadeghimahalli F, Amuei F, Dabbaghi S. An assessment of internal evaluations in departments of basic sciences in Mazandaran University of Medical Sciences 2015. Dev Strateg Med Educ. 2016;3(2):63-74.
33. Parsa Yekta Z, Salmaani Barough N, Monjamed Z, Farzianpour F, Eshraghian M. Internal evaluation in Faculty of Nursing and Midwifery, Tehran University of Medical Sciences. Hayat. 2005;11(1-2):71-8.
34. Saravani S, Esmaeli N, Rezaeikeikhaei K, Rezaei Kahkhae L, Esmaeli Z. Internal evaluation of social medicine department of Zabol University of Medical Sciences. mededj. 2022;10(1):31-44.
35. Sadeghimahalli F, Sadeghimahalli N, Khaleghzadeh-Ahangar H, Amuei F, Mahmodi E. Study of the education and research quality in basic sciences through internal evaluation in two consecutive educational years in MUMS. Res Med Edu. 2019;11(1):20-8. [DOI:10.29252/rme.11.1.20]
36. Tashakkori A, Creswell JW. The new era of mixed methods. J Mix Methods Res. 2007;1(1):3-7. [DOI:10.1177/2345678906293042]
37. Heyvaert M, Maes B, Onghena P. Mixed methods research synthesis: definition, framework, and potential. Qual Quant. 2013;47(2):659-76. [DOI:10.1007/s11135-011-9538-6]
38. Merliana NP, Tantri NN. Improving the quality of Hindu education in the era of society 5.0 through digital culture. In: International Proceeding on Religion, Culture, Law, Education, and Hindu Studies. 2022. p. 203-16.
39. Somasundaram MJ, Junaid KM, Mangadu S. Artificial intelligence (AI) enabled intelligent quality management system (IQMS) for personalized learning path. Procedia Comput Sci. 2020;172:438-42. [DOI:10.1016/j.procs.2020.05.096]
40. Ibrahim SM. The effects of implementing artificial intelligence systems on enhancing educational services' quality from the perspective of employees at Alzaiem Alazhari University-Sudan. Kurdish Stud. 2024;12(2):1453-67.
41. Sahari S. Exploring the role of AI in advancing quality education in higher institutions for sustainable development. Int J Humanit Soc Sci Stud. 2024;10(3):185-95.
42. Muminov DM. Development of artificial intelligence and its impact on educational quality in public schools. Ment Enlight Sci Methodol J. 2024;5(5):169-74.
43. a EP, Arruda DP. Artificial intelligence for SDG 4 of the 2030 agenda: transforming education to achieve quality, equality, and inclusion. Sustain Econ. 2024;2(2):34-50. [DOI:10.62617/se.v2i2.34]
44. Buaton R, Muhammad Z, Dilham A. Optimization of higher education internal quality audits based on artificial intelligence. J Artif Intell Eng Appl. 2022;1(2):158-61. [DOI:10.59934/jaiea.v1i2.83]
45. Judijanto L, Aswamedhika A, Aksan I, Mustofa I. Student sentiment analysis: implementation of artificial intelligence in improving teaching quality. J Soc Sci Util Technol. 2023;1(4):227-38. [DOI:10.70177/jssut.v1i4.664]
46. Sayfullayeva N. The role of artificial intelligence in improving the quality of student learning process. Sci Innov. 2024;3(B6):195-203.
47. Abdullayev J. Harnessing technologies for enhancing the quality of higher education. Educ Res Univ Sci. 2023;2(3):1261-5.
48. Nugroho AD, Anwar K. Implementation of artificial intelligence in increasing the quality of learning. In: Proceeding of International Conference on Education, Society and Humanity; 2023 May 30; Vol. 1, No. 1. p. 302-6.
49. Shikokoti H, Mutegi R. Influence of artificial intelligence on the quality of education in higher learning: a case study of Faculty of Education, University of Nairobi, Kenya. J Educ Pract. 2024;15:97-114. [DOI:10.2139/ssrn.5014109]
50. Lei Q. Modern educational technology theory and university quality education. In: 7th International Conference on Management, Education, Information and Control (MEICI 2017); 2017 Oct. Atlantis Press; 2017. p. 287-91. [DOI:10.2991/meici-17.2017.58]
51. Chemlal Y, Azouazi M. Implementing quality assurance practices in teaching machine learning in higher education. Math Model Comput. 2023;10(3):660-7. [DOI:10.23939/mmc2023.03.660]
52. Wang T. The high-quality development path of education from the perspective of digitization. Educ Rev USA. 2023;7(9):1339-43. [DOI:10.26855/er.2023.09.019]
53. Chekirine D, Zoubida S. Artificial intelligence's impact on higher education quality. J Sci Knowl Horiz. 2024;4(1):606-23. [DOI:10.34118/jskp.v4i01.3889]
54. Hafiiak A, Yastreba S, Nosach O, Borodina E. Information technology as a component of improving the training quality future specialists in higher education institutions. Syst Control Navig Commun. 2019;2(54):60-4. [DOI:10.26906/SUNZ.2019.2.060]
55. Peñalvo FJ, Alier M, Pereira J, Casany MJ. Safe, transparent, and ethical artificial intelligence: keys to quality sustainable education (SDG4). IJERI. 2024;(22):1-21. [DOI:10.46661/ijeri.11036]
56. Li M, Su Y. Evaluation of online teaching quality of basic education based on artificial intelligence. Int J Emerg Technol Learn. 2020;15(16):147-61. [DOI:10.3991/ijet.v15i16.15937]
57. Yang Z. Digital transformation to advance high-quality development of higher education. J Educ Technol Dev Exch. 2022;15(2):15-23. [DOI:10.18785/jetde.1502.02]
58. Hussain MI, Shamim M, Ravi Sankar AV, Kumar M, Samanta K, Sakhare DT. The effect of the artificial intelligence on learning quality & practices in higher education. J Posit Sch Psychol. 2022;6(6):1002-9.
59. Flores-Viva JM, García-Peñalvo FJ. Reflections on the ethics, potential, and challenges of artificial intelligence in the framework of quality education (SDG4). Comunicar. 2023;31(74):35-44. [DOI:10.3916/C74-2023-03]
60. Perminova L, Vasylyuk-Zaitseva S, Shapka I, Savastru N. The role of artificial intelligence in improving the quality of education and research. Futurity Educ. 2023;3(4):46-59. [DOI:10.57125/FED.2023.12.25.03]
61. Yuan L, Xiaofei Z, Yiyu Q. Evaluation model of art internal auxiliary teaching quality based on artificial intelligence under the influence of COVID-19. J Intell Fuzzy Syst. 2020;39(6):8713-21. [DOI:10.3233/JIFS-189267]
62. Patil V. The potential of AI in enhancing education access and quality. Int J Sci Res Eng Trends. 2024;10(1):160-9. [DOI:10.61137/ijsret.vol.10.issue1.133]
63. Ajani OA, Gamede B, Matiyenga TC. Leveraging artificial intelligence to enhance teaching and learning in higher education: promoting quality education and critical engagement. J Pedagog Sociol Psychol. 2024;7(1):54-69. [DOI:10.33902/JPSP.202528400]
64. Lv F. Research on evaluation of teaching quality of marxist theory in massive open online course based on artificial intelligent. In: Journal of Physics: Conference Series; 2021 May 1; Vol. 1915, No. 2. IOP Publishing; 2021. p. 022050. [DOI:10.1088/1742-6596/1915/2/022050]
65. Yugandhar K, Rao YR. Artificial intelligence in classroom management: improving instructional quality of English class with AI tools. Educ Adm Theory Pract. 2024;30(4):2666-72.
66. Li F, Wang C. Artificial intelligence and edge computing for teaching quality evaluation based on 5G-enabled wireless communication technology. J Cloud Comput. 2023;12(1):45. [DOI:10.1186/s13677-023-00418-6]
67. Altinay Z, Altinay F, Sharma RC, Dagli G, Shadiev R, Yikici B, et al. Capacity building for student teachers in learning, teaching artificial intelligence for quality of education. Societies. 2024;14(8):148. [DOI:10.3390/soc14080148]
68. Rane N. Enhancing the quality of teaching and learning through ChatGPT and similar large language models: challenges, future prospects, and ethical considerations in education. 2023 Sep 15. [DOI:10.2139/ssrn.4599104]
69. Utkirov A. Artificial intelligence impact on higher education quality and efficiency. Eurasian J Acad Res. 2024;4(9):52-8. [DOI:10.47390/SPR1342V4I9Y2024N52]
70. Verma A, Kumar Y, Kohli R. Study of AI techniques in quality educations: challenges and recent progress. SN Comput Sci. 2021;2(4):238. [DOI:10.1007/s42979-021-00635-3]
71. Rodríguez-Abitia G, Martínez-Pérez S, Ramirez-Montoya MS, Lopez-Caudana E. Digital gap in universities and challenges for quality education: a diagnostic study in Mexico and Spain. Sustainability. 2020;12(21):9069. [DOI:10.3390/su12219069]
72. Nedungadi P, Tang KY, Raman R. The transformative power of generative artificial intelligence for achieving the sustainable development goal of quality education. Sustainability. 2024;16(22):9779. [DOI:10.3390/su16229779]
73. Rahayu ST. Analyzing of using educational technology to improve the quality and equity of learning outcomes at Politeknik Maritim Negeri. J Iqra. 2023;8(1):100-16. Ahmed S. The role of artificial intelligence applications in enhancing the quality of online higher education. Int J Financ Adm Econ Sci. 2024;3(2):10-28. [DOI:10.25217/ji.v8i1.3238]
74. Ahmad S, Ahmed A, Bhutta SM, Ansari AN. Transforming teaching learning with chatbots in higher education: quest, opportunities and challenges for quality enhancement. In: The Evolution of Artificial Intelligence in Higher Education. Emerald Publishing Limited; 2024. p. 111-27. [DOI:10.1108/978-1-83549-486-820241007]
75. Nie J. Research on improving education quality and efficiency through artificial intelligence and big data analysis. J Artif Intell Pract. 2023;6(8):35-40. [DOI:10.23977/jaip.2023.060806]
76. Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs. 2008;62(1):107-15. [DOI:10.1111/j.1365-2648.2007.04569.x] [PMID]
77. Keykha A, Ezati M, Salehi M. Entrepreneur university model design: qualitative approach (case study: University of Tehran). Iran J Eng Educ. 2019;21(83):69-90.
78. Keykha A, Shafiee M, Mahdi R. Digital developments and perspectives of future higher education in the horizon of 1410. J Ind Univ. 2023;14(3):9-24.
79. Supriyanto EE, Saputra J. Big data and artificial intelligence in policy making: a mini-review approach. Int J Adv Soc Sci Humanit. 2022;1(2):58-65. [DOI:10.56225/ijassh.v1i2.40]
80. Biloslavo R, Edgar D, Aydin E, Bulut C. Artificial intelligence (AI) and strategic planning process within VUCA environments: a research agenda and guidelines. Manag Decis. 2024;62(13):1-31. [DOI:10.1108/MD-10-2023-1944]
81. Seyf HM, Amin BM, Yazdiha M, Nabavi M, Faranoush M. Internal evaluation as a means of promoting the quality of education in the department of pediatrics of Semnan University of Medical Sciences. J Med Educ Dev. 2012;5(9):65-73.
82. Mirzaei A, Sadeghifar J, Mousavi SM, Khodayari R. Internal evaluation in selected educational departments of faculty of medicine in Ilam University of Medical Sciences (a short report). J Rafsanjan Univ Med Sci. 2013;12(7):583-90.
83. Shakhi K, Hossinpour D, Maharloo HR, Zahiri M, Haghighi Zadeh MH. Students' views about the educational quality of health services management department in AJUMS. Educ Dev Judishapur. 2013;4(3):83-9.
84. Sadeghimahalli F, Sadeghimahalli N, Khaleghzadeh-Ahangar H, Amuei F, Mahmodi E. Study of the education and research quality in basic sciences through internal evaluation in two consecutive educational years in MUMS. Res Med Edu. 2019;11(1):20-8. [DOI:10.29252/rme.11.1.20]
85. Olan F, Arakpogun EO, Suklan J, Nakpodia F, Damij N, Jayawickrama U. Artificial intelligence and knowledge sharing: contributing factors to organizational performance. J Bus Res. 2022;145:605-15. [DOI:10.1016/j.jbusres.2022.03.008]
86. Al Nabhani F, Hamzah MB, Abuhassna H. The role of artificial intelligence in personalizing educational content: enhancing the learning experience and developing the teacher's role in an integrated educational environment. Contemp Educ Technol. 2025;17(2):ep525. [DOI:10.30935/cedtech/16089]
87. Bhaskar P, Tiwari CK, Joshi A. Blockchain in education management: present and future applications. Interact Technol Smart Educ. 2020;18(1):1-17. [DOI:10.1108/ITSE-07-2020-0102]
88. Balayan A, Connor C, LaFave J. The evolution of graduate enrollment management. Strateg Enroll Manag Q. 2022;9(4):35-46.
89. Berente N, Gu B, Recker J, Santhanam R. Managing artificial intelligence. MIS Q. 2021;45(3):1433-50. [DOI:10.25300/MISQ/2021/16274]
90. Nankervis A, Connell J, Cameron R, Montague A, Prikshat V. 'Are we there yet?' Australian HR professionals and the Fourth Industrial Revolution. Asia Pac J Hum Resour. 2021;59(1):3-19. [DOI:10.1111/1744-7941.12245]
91. Palos-Sánchez PR, Baena-Luna P, Badicu A, Infante-Moro JC. Artificial intelligence and human resources management: a bibliometric analysis. Appl Artif Intell. 2022;36(1):2145631. [DOI:10.1080/08839514.2022.2145631]
92. Saravani S, Esmaeli N, Rezaeikeikhaei K, Rezaei Kahkhae L, Esmaeli Z. Internal evaluation of social medicine department of Zabol University of Medical Sciences. mededj. 2022;10(1):31-44.
93. Rahimifard H, Koohpaie A, Arast Y, Behnamipour S, Mahdinia M. Internal evaluation of department of occupational health of Qom University of Medical Sciences in academic year 2010-2011. Qom Univ Med Sci J. 2013;7(S1):86-91.
94. Ahmad SF, Alam MM, Rahmat MK, Mubarik MS, Hyder SI. Academic and administrative role of artificial intelligence in education. Sustainability. 2022;14(3):1101. [DOI:10.3390/su14031101]
95. Goksel N, Bozkurt A. Artificial intelligence in education: current insights and future perspectives. In: Sisman-Ugur S, Kurubacak G, editors. Handbook of Research on Learning in the Age of Transhumanism. IGI Global; 2019. p. 224-36. [DOI:10.4018/978-1-5225-8431-5.ch014]
96. Cui L, Huang S, Wei F, Tan C, Duan C, Zhou M. Superagent: a customer service chatbot for e-commerce websites. In: *Proceedings of the 55th Annual Meeting of the Association for Computational Linguistics-System Demonstrations*; 2017 Jul; Vancouver, Canada. Association for Computational Linguistics; 2017. p. 97-102. [DOI:10.18653/v1/P17-4017]
97. Kumar R. Faculty members' use of artificial intelligence to grade student papers: a case of implications. Int J Educ Integr. 2023;19(1):9. [DOI:10.1007/s40979-023-00130-7]
98. Wang X, Li L, Tan SC, Yang L, Lei J. Preparing for AI-enhanced education: conceptualizing and empirically examining teachers' AI readiness. Comput Human Behav. 2023;146:107798. [DOI:10.1016/j.chb.2023.107798]
99. Chan CKY, Tsi LH. The AI revolution in education: will AI replace or assist teachers in higher education? arXiv. 2023.
100. Vera F. Integration of artificial intelligence technology in higher education: exploring faculty members' experience. Transformar. 2023;4(3):17-22.
101. Mirmohammadi SJ, Mehrparvar AH, Bahaloo M, Davari MH. Satisfaction of Shahid Sadoughi University of Medical Sciences' alumni about the quality of medical education. J Med Educ Dev. 2013;8(2):10-18.
102. Dashti N, Einollahi N, Zare Bavani M, Abbasi S. Internal evaluation of medical laboratory sciences department of allied health sciences school, Tehran University of Medical Sciences (2010). Payavard Salamat. 2012;6(2):131-42.
103. Afandideh N, Hakimzadeh R. Qualification of e-learning; medical education courses of Tehran University of Medical Sciences. Educ Strateg Med Sci. 2014;7(4):235-42.
104. Nobakht M, Gholami H, Emadzadeh A, Momeni RA. A survey on the quality of master of medical education e-learning course at Mashhad University of Medical Sciences. J Med Educ Dev. 2015;10(25):60-71.
105. Selwyn N, Gallo Cordoba B. Australian public understandings of artificial intelligence. AI Soc. 2022;37(4):1645-62. [DOI:10.1007/s00146-021-01268-z]
106. Whalen J, Mouza C. ChatGPT: challenges, opportunities, and implications for teacher education. Contemp Issues Technol Teach Educ. 2023;23(1):1-23.
107. Huang J, Saleh S, Liu Y. A review on artificial intelligence in education. Acad J Interdiscip Stud. 2021;10(3):209. [DOI:10.36941/ajis-2021-0077]
108. Chen Y, Jensen S, Albert LJ, Gupta S, Lee T. Artificial intelligence (AI) student assistants in the classroom: designing chatbots to support student success. Inf Syst Front. 2023;25(1):161-82. [DOI:10.1007/s10796-022-10291-4]
109. Su KD. Implementation of innovative artificial intelligence cognitions with problem-based learning guided tasks to enhance students' performance in science. J Balt Sci Educ. 2022;21(2):245-57. [DOI:10.33225/jbse/22.21.245]
110. Lyerly E. Utilizing ChatGPT to help students with disabilities. Disabil Compl High Educ. 2023;28(9):2-7. [DOI:10.1002/dhe.31479]
111. Robert A, Potter K, Frank L. The impact of artificial intelligence on students' learning experience. J Educ Technol Innov. 2024;2(2):71-6.
112. Yarmohammadian MH, Kalbasi A. Internal evaluation of departments in the school of management and medical informatics, Isfahan University of Medical Science. Iran J Med Educ. 2006;6(1):125-34.
113. Aghababaie S, Riazi H, Artimani T, Shobeiri F. Internal evaluation of mother and child & midwifery departments of Hamadan University of Medical Sciences. Avicenna J Nurs Midwifery Care. 2012;20(1):39-49.
114. Xiao M, Yi H. Building an efficient artificial intelligence model for personalized training in colleges and universities. Comput Appl Eng Educ. 2021;29(2):350-8. [DOI:10.1002/cae.22235]
115. Bryndin E. Self-learning AI in educational research and other fields. Res Intell Manuf Assembly. 2024;3(1):129-37. [DOI:10.25082/RIMA.2024.01.005]
116. Tan SC, Lee AV, Lee M. A systematic review of artificial intelligence techniques for collaborative learning over the past two decades. Comput Educ Artif Intell. 2022;3:100097. [DOI:10.1016/j.caeai.2022.100097]
117. Ambarita N, Nurrahmatullah MF. Impacts of artificial intelligence on student learning: a systematic literature review. J Varidika. 2024;36(1):13-30. [DOI:10.23917/varidika.v36i1.4730]
118. Pisica AI, Edu T, Zaharia RM, Zaharia R. Implementing artificial intelligence in higher education: pros and cons from the perspectives of academics. Societies. 2023;13(5):118. [DOI:10.3390/soc13050118]
119. Zhai X, Haudek KC, Shi L, Nehm RH, Urban-Lurain M. From substitution to redefinition: a framework of machine learning-based science assessment. J Res Sci Teach. 2020;57(9):1430-59. [DOI:10.1002/tea.21658]
120. Crawford J, Cowling M, Allen KA. Leadership is needed for ethical ChatGPT: character, assessment, and learning using artificial intelligence (AI). J Univ Teach Learn Pract. 2023;20(3):02. [DOI:10.53761/1.20.3.02]
121. Mislevy RJ, Yan D, Gobert J, Sao Pedro M. Automated scoring in intelligent tutoring systems. In: Drasgow F, editor. Handbook of Automated Scoring. Chapman and Hall/CRC; 2020. p. 403-22. [DOI:10.1201/9781351264808-22]
122. Masoomi B, Dastgiri M. Evaluation of medical students' opinion about quality of education in medical emergency ward in Isfahan University of Medical Sciences. J Isfahan Med Sch. 2011;28(121):1617-27.
123. Khoshrang H, Salari A, Dadgaran I, Moaddab F, Rouhi-Balasii L, Pourkazemi I. Quality of education provided at the clinical skills lab from medical students' viewpoints in Guilan University of Medical Sciences. Res Med Educ. 2016;8(2):77-83. [DOI:10.18869/acadpub.rme.8.2.77]
124. Chabook FA, Keyhan J, Hassani M, Sameri M, Feyzi A. Evaluating the quality of higher education from the perspective of students: a case study of Urmia University of Medical Sciences. Res Teach. 2023;11(1):22-39.
125. Lin XP, Li BB, Yao ZN, Yang Z, Zhang M. The impact of virtual reality on student engagement in the classroom-a critical review of the literature. Front Psychol. 2024;15:1360574. [DOI:10.3389/fpsyg.2024.1360574] [PMID] []
126. Tsivitanidou OE, Georgiou Y, Ioannou A. A learning experience in inquiry-based physics with immersive virtual reality: student perceptions and an interaction effect between conceptual gains and attitudinal profiles. J Sci Educ Technol. 2021;30(6):841-61. [DOI:10.1007/s10956-021-09924-1]
127. Suresh Babu S, Dhakshina Moorthy A. Application of artificial intelligence in adaptation of gamification in education: a literature review. Comput Appl Eng Educ. 2024;32(1):e22683. [DOI:10.1002/cae.22683]
128. Ahuja AS, Polascik BW, Doddapaneni D, Byrnes ES, Sridhar J. The digital metaverse: applications in artificial intelligence, medical education, and integrative health. Integr Med Res. 2023;12(1):100917. [DOI:10.1016/j.imr.2022.100917] [PMID] []
129. Williamson B. The hidden architecture of higher education: building a big data infrastructure for the 'smarter university'. Int J Educ Technol High Educ. 2018;15(1):12. [DOI:10.1186/s41239-018-0094-1]
130. Ejjami R. The future of learning: AI-based curriculum development. Int J Multidiscip Res. 2024;6(4):1-31. [DOI:10.36948/ijfmr.2024.v06i04.24441]
131. Kwok LF. A vision for the development of i-campus. Smart Learn Environ. 2015;2:1-2. [DOI:10.1186/s40561-015-0009-8]
132. Xiao J. Digital transformation in higher education: critiquing the five-year development plans (2016-2020) of 75 Chinese universities. Distance Educ. 2019;40(4):515-33. [DOI:10.1080/01587919.2019.1680272]
133. Arabzadeh T, Dastpaki F, Shojaei A, Ashafeli A, Faramarzinia Z. Evaluating the quality of clinical education from outlook of operating room technology students of Behbahan University of Medical Sciences in the Covid-19 pandemic. Educ Dev Judishapur. 2024;15(4):370-83.
134. Bazazi N, Houshmand B. Medical students' viewpoints about the quality of education in outpatient clinics in Hamedan University of Medical Sciences in 2007. Iran J Med Educ. 2011;11(2):124-33.
135. Raygan AR, Mahamed F, Rezaee S, Jamshidi A, Fararouyee M, Karimzadeh K, et al. Internal evaluation of educational groups of health school of Yasouj University of Medical Sciences in 2009. Res Med Educ. 2011;3(2):43-51.
136. Wang S, Wang F, Zhu Z, Wang J, Tran T, Du Z. Artificial intelligence in education: a systematic literature review. Expert Syst Appl. 2024;252:124167. [DOI:10.1016/j.eswa.2024.124167]
137. Calo R. Artificial intelligence policy: a primer and roadmap. UC Davis Law Rev. 2017;51:399-435. [DOI:10.2139/ssrn.3015350]
138. Švab I, Klemenc-Ketiš Z, Zupanič S. New challenges in scientific publications: referencing, artificial intelligence and ChatGPT. Slov J Public Health. 2023;62(3):109-12. [DOI:10.2478/sjph-2023-0015] [PMID] []
139. Tai AM, Meyer M, Varidel M, Prodan A, Vogel M, Iorfino F, et al. Exploring the potential and limitations of ChatGPT for academic peer-reviewed writing: addressing linguistic injustice and ethical concerns. J Acad Lang Learn. 2023;17(1):T16-30.
140. Fatani B. ChatGPT for future medical and dental research. Cureus. 2023;15(4):e37285. [DOI:10.7759/cureus.37285]
141. Tovfighiyan T, Shojaee S, Rahnamaye Rahsepar SF. Internal evaluation of nursing department of Sabzevar University of Medical Sciences. J Sabzevar Univ Med Sci. 2013;20(5):791-800.
142. Cribben I, Zeinali Y. The benefits and limitations of ChatGPT in business education and research: a focus on management science, operations management and data analytics. SSRN [Preprint]. 2023 [cited 2025 Aug 14]. Available from: [DOI:10.2139/ssrn.4404276]
143. Rahman MM, Watanobe Y. ChatGPT for education and research: opportunities, threats, and strategies. Appl Sci. 2023;13(9):5783. [DOI:10.3390/app13095783]
144. Keykha A, Behravesh S, Ghaemi F. ChatGPT and medical research: a meta-synthesis of opportunities and challenges. J Adv Med Educ Prof. 2024;12(3):135-46.
145. Jafari F, Keykha A, Taheriankalati A, Taghavi Monfared AV. The role of AI in shaping medical education: insights from an umbrella review of review studies. J Adv Med Educ Prof. 2025;13(4):270-93.
146. Keykha A, Mohammadi F, Taghavi Monfared A, Taheriankalati A. Unblocking innovation: a meta-synthesis of blockchain applications in medical education, research, and healthcare. Strides Dev Med Educ. 2025;22(1):e148521.
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
