
Thu, Jul 30, 2026
[Archive]
Volume 18, Issue 1 (2025)
J Med Edu Dev 2025, 18(1): 42-53 |
Back to browse issues page


Ethics code: IR.KUMS.REC.1401.453.
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Khodabakhsh E, Keramati A, Barry A, Rahmani Tanha R, Babazadeh M, Pourbairamian G et al . A comparative study of the implementation of the doughnut round teaching and the lecture method on self-regulation and motivation of medical students' academic progress: A semi-experimental study. J Med Edu Dev 2025; 18 (1) :42-53
URL: http://edujournal.zums.ac.ir/article-1-2265-en.html
URL: http://edujournal.zums.ac.ir/article-1-2265-en.html
Elmira Khodabakhsh1  , Ali Keramati2 , Azizeh Barry3 , Rastegar Rahmani Tanha4 , Maryam Babazadeh5 , Ghadir Pourbairamian6 , Ghobad Ramezani *7
, Ali Keramati2 , Azizeh Barry3 , Rastegar Rahmani Tanha4 , Maryam Babazadeh5 , Ghadir Pourbairamian6 , Ghobad Ramezani *7
, Ali Keramati2 , Azizeh Barry3 , Rastegar Rahmani Tanha4 , Maryam Babazadeh5 , Ghadir Pourbairamian6 , Ghobad Ramezani *7
1- Assistant Professor of General Surgery, Mazandaran University of Medical Sciences, Sari, Iran.
2- Department of Pediatrics, Medical School, Kermanshah University of Medical Sciences, Kermanshah, Iran.
3- Ph.D Student of Medical Education, Center for Educational Research in Medical Sciences(CERMS), Department of Medical Education, School of Medicine, Iran University of Medical Sciences, Tehran, Iran
4- Department of Neurosurgery, School of Medicine, Kermanshah University of Medical Sciences, Kermanshah, Iran
5- Department of Social Medicine, Faculty of Medicine, pecialist in Social Medicine and Preventive Medicine, Alborz University of Medical Sciences
6- Education Development Center, Ardabil University of Medical Sciences, Ardabil, Iran
7- Education Development Center, Kermanshah University of Medical Sciences, Kermanshah, Iran ,ramaznighobad@gmail.com
2- Department of Pediatrics, Medical School, Kermanshah University of Medical Sciences, Kermanshah, Iran.
3- Ph.D Student of Medical Education, Center for Educational Research in Medical Sciences(CERMS), Department of Medical Education, School of Medicine, Iran University of Medical Sciences, Tehran, Iran
4- Department of Neurosurgery, School of Medicine, Kermanshah University of Medical Sciences, Kermanshah, Iran
5- Department of Social Medicine, Faculty of Medicine, pecialist in Social Medicine and Preventive Medicine, Alborz University of Medical Sciences
6- Education Development Center, Ardabil University of Medical Sciences, Ardabil, Iran
7- Education Development Center, Kermanshah University of Medical Sciences, Kermanshah, Iran ,
Keywords: self-regulation, motivation, medical education, teaching methods, active learning, educational rounds, randomized controlled trial
Full-Text [PDF 899 kb]
(661 Downloads)
| Abstract (HTML) (3098 Views)
Full-Text: (565 Views)
Abstract
Background & Objective: In medical education, effective teaching/learning strategies are crucial, especially those that improve academic motivation and self-control. The aim of this study was to evaluate how the doughnut round teaching method versus the traditional lecture approach affected medical students’ motivation and self-regulation.
Materials & Methods: Forty medical students participated in this semi-experimental study. The participants were divided into two groups using the random allocation method through Excel software: The A group was doughnut (20 students), while the B group followed lecture methods (20 students). Both before and after the intervention, assessments were conducted using Hatter's academic motivation scale and Bouffard's self-regulation scale. ANCOVA, the independent t-test, the paired t-test, and the Kolmogorov-Smirnov test were among the statistics we employed for data analysis. Software called SPSS version 16 was used for all of our analyses.
Results: The treatment group demonstrated significant improvements in academic motivation (p < 0.001) and self-regulation (p < 0.001) in the post-test, while the control group showed no significant changes. The experimental group's pre-test and post-test scores significantly differed, indicating the effectiveness of the doughnut round teaching method in enhancing self-control and motivation.
Conclusion: The round doughnut round teaching technique significantly outperformed the standard lecture style in terms of students' academic motivation and self-regulation. This approach promotes independent study and active participation, which may improve academic performance in medical school.
Introduction
Students from various clinical disciplines in each hospital ward are considered part of the treatment staff and care team. Clinical education is a crucial phase of medical training that significantly influences students' professional development and allows them to apply their theoretical knowledge practically. One of the most visible forms of clinical training is the clinical round, which occurs alongside diagnostic, treatment, and patient care activities in teaching hospital wards [1, 2]. One of the key objectives of every medical school is to prepare students to become effective members of the medical staff and to develop skilled healthcare professionals for society. In this context, the role and significance of clinical education become even more significant. Proper clinical training allows students to gain valuable experiences essential for their future careers in medicine [3-5].One form of conducting rounds is the conference-based round, also known as an educational round. In this type of round, the professor and students engage in discussions and exchange opinions about the disease or specific conditions of a patient, culminating in a conference presentation on the topic. This form of training, along with clinical rounds, contributes to the professional development of students during their study and internship periods [6]. However, it has been noted that non-clinical rounds often do not follow a proper implementation framework, leading to various obstacles and challenges. Key issues include a lack of alignment between theoretical and practical components, overcrowding of students, and the stressful clinical environments in which these training rounds occur, such as crowded corridors and busy operating rooms [7-9].These deficiencies highlight the need for a revision of the current approach. Therefore, there is a growing interest in adopting new, active, and self-directed educational methods for non-clinical rounds. One such approach is the doughnut round teaching. The way this educational round is held is that starting one week before the round, the professor determines the sources for study with the students' consent, and then each student is asked to write the specified content. Study the week and design 10 questions with different taxonomies (easy, medium and difficult) and in different formats (short answer, multiple choices) and prepare their answers. Before holding the round, the relevant professor must have all the questions designed by Confirm the students with the correct answer. In the following, according to the schedule set in advance by the professor, which is usually one session, one hour per week, and the students appear in small groups and only the basic information of the relevant case is provided by the professor at the beginning of the session, then randomly one of the students asks another student his question and gives a score from 1 to 3 according to his satisfaction with his answer and then gives the correct answer as well. If a student answers correctly, they will choose the next participant. If the answer is incorrect, the first student will select the next person. This process will continue until the champion student, determined by the points earned, is established. The entire topic related to the case will be covered, and participants will learn about the subject through these questions, answers, and their interactions with each other [10].This training round, characterized by its structured format, serves as a self-directed learning approach. It offers numerous advantages, including the opportunity for structured discussions with multiple participants within a short time frame, enhancing the self-confidence of learners, improving communication skills, and boosting motivation to acquire knowledge. Additionally, this teaching method encourages active participation in the learning process and is recognized as an approach rooted in games and entertainment [11-13].On the other hand, the discussion of self-regulation and the motivation to progress in students is one of the most important recent topics in the field of medical education. Researchers do not consider self-regulation learning strategies as a fixed and unchanging trait, but consider it a skill that results in its development in the individual through personal experiences and the use of these strategies in practice [14]. Learners who use self-regulated learning strategies while achieving higher levels of self-efficacy and correct understanding of learning as a task value, will be able to improve their academic performance levels [15].Self-regulation can be considered a behavior that refers to the optimal use of various resources and increases learning. Motivational self-regulation refers to the active use of motivational strategies to increase learning. Learners with motivational self-regulation in all stages of learning consider themselves to be self-efficacious and independent. Cognitively and met cognitively, self-regulating people are people who use planning, organizing, self-learning, self-control, and self-evaluation in the learning process. Learning self-regulation during the acquisition of skills may justify the individual differences of people [16, 17]. Motivation is one of the common concepts in educational issues, and its role in academic progress has long been the focus of psychologists. Nowadays, creating motivation as a motivating factor in learners and directing their activities is more and more the attention of educational authorities. In educational theories, motivation is considered a basic concept. Psychologists and teachers consider motivation as one of the key concepts used to explain different levels of progress. This concept tells the difference in the amount of effort to do the homework [18]. According to the above documents and the new findings of psychology and education, the necessity of the present study is to use new and active methods and methods of teaching and training, especially in the field of clinical education. To educate medical students during the non-clinical rounds, the researchers plan to utilize a teaching method known as the doughnut round. They will then evaluate and compare the effectiveness of this method with traditional lectures in enhancing academic self-regulation and motivating student progress. The research hypotheses included the following:
1. The average academic self-regulation score of medical students before the intervention is different in the experimental and control groups.
2. There is a difference in the average academic self-regulation score of medical students after the intervention in the experimental and control groups.
3. There is a difference between the mean score of medical students' academic achievement motivation before and after the intervention in the control group.
4. There is a difference between the mean scores of medical students' academic achievement motivation before and after the intervention in the experimental group.
5. The average score of self-regulation and academic achievement motivation of medical students in the experimental and a control group is different based on demographic characteristics.
Materials & Methods
Design and setting(s)
This semi-experimental study was conducted on 40 medical students (20 people in each group) at Kermanshah University of Medical Sciences. The current study is a semi-experimental study of pre-test and post-test types with random assignment to two control and experimental groups, in which the effect of the doughnut round teaching and lecture method was studied. Before the intervention, both groups responded to Bouffard's self-regulation scale and Hatter's motivation for academic progress. At the end of the intervention, both groups responded to the tool again.
Participants and sampling
The research population consisted of medical students enrolled at Kermanshah University of Medical Sciences for the 2023-24 academic year. The sample size for this study was determined using Cohen's table to specify sample sizes for experimental studies. Considering an effect size of 1, a test power of 0.80, and a significance level of 0.05, the minimum sample size required for each group was established as 17 individuals. In addition to Cohen's formula, according to Gall et al., translated by Nasr, the criterion for selecting 15 people for each group is also based on previous studies and experts' opinions, so a 15-person sample size is considered sufficient in semi-experimental studies. (Gall M, Borg W, Gall J. Nasr AR, translator [19].Considering an anticipated dropout rate of approximately 15%, a sample size of 20 students per group was deemed appropriate.
Figure 1. CONSORT flow diagram of the study
Figure 1 presents a CONSORT flow diagram showing the study process. The participants were divided into two groups using the random allocation method through Excel software: The A group consisted of doughnuts (20 students). In contrast, the B group followed lecture methods (20 students). The eligibility criteria required students to provide informed consent and to have passed the prerequisite credits (including basic science courses and clinical preparation). The exclusion criteria included lack of consent, failure to pass prerequisite credits, and missing more than two sessions.
Tools/Instruments
Bouffard's self-regulation scale is a 14-question questionnaire designed to measure self-regulation based on Bandura's social-cognitive theory. The questions of this questionnaire are on a 5-point Likert scale (completely agree 5, agree 4, have no opinion 3, disagree 2, and completely disagree 1) and measure two factors of cognitive strategies and metacognitive strategies of self-regulation. Questions 5, 13, and 14 are scored in a reverse way; the total scores of each person can be 14-60. A higher score in each component shows a person's tendency to use that component. The overall reliability coefficient of Bouffard's self-regulation scale was obtained based on Cronbach's alpha of 0.71. The reliability of the cognitive strategies subscale is 0.70, and the metacognitive subscale is 0.68. The reliability of the above test was reported as 0.63 in research conducted by Entezari et al. [20]. In addition, the reliability of the above test was reported as 0.67 and 0.69, respectively, in the study conducted by Zamani et al. [21] and Bagheri Kerachi and Razmjoo [22]. In addition, the reliability of Bouffard's self-regulation scale in research conducted by Ghazvineh et al. [23] has been obtained.
The factor analysis results showed that the correlation coefficient between the questions is appropriate, the value load related to the factors is acceptable, and its validity is also at the desired level. bagheri mousavi and Kadivar [4] also studied the validity and reliability of Boufard's self-regulation scale. The construct validity of this questionnaire has been reported to be optimal by using correlation coefficients and factor analysis of discriminating correlation coefficients between questionnaire questions. Cronbach's alpha coefficient to measure internal consistency was 0.08. Based on this, this questionnaire can predict the scores and actual scores of the subjects. In this study, five medical education specialists confirmed the face validity of the questionnaire, and Cronbach's alpha was calculated at 0.82.
Another questionnaire was the Hatter academic motivation scale. This scale measures people's academic motivation level in the two components: Intrinsic and external motivation. This questionnaire has 33 questions; the answer to each question is on a five-point Likert scale from never to always. Also, Harter's academic motivation questionnaire has validity, reliability, and scoring. The alpha reliability coefficient was 0.83 in the study of Zare et al. [25] and 0.86 in the study of Fallahi et al. [26] The validity of this tool has been proven in the above research. In this study, five medical education specialists confirmed the face validity of the questionnaire, and Cronbach's alpha was calculated as 0.79.
Data collection methods
Before implementing the intervention, a pre-test was conducted to assess the students' knowledge levels on specified topics. This pre-test was administered to all four groups one day before the first intervention. The pre-test tool consisted of a 20-item multiple-choice questionnaire developed specifically for this study. The questions were designed based on a structured blueprint derived from core educational topics, including fever without a source, poisoning with chemicals, gastroenteritis, and neonatal jaundice. Each question followed the standards of the Millman checklist to ensure relevance and thorough content coverage. The questions were initially drafted based on key topics within the clinical curriculum and refined with input from five clinical education specialists. This panel of experts reviewed each question for clarity, relevance, and alignment with the educational objectives to establish face and content validity. To assess the reliability of the test, Cronbach's alpha was calculated and yielded a coefficient of 0.78, indicating acceptable internal consistency. This suggests that the test provides a reliable measure of students' baseline knowledge in the specified topics. Each correct answer was assigned one point, with 20 points possible. This score provided a baseline index for each student's knowledge of the selected clinical topics.
In the intervention implementation stage, the training for the intervention group began one day after the pre-test. Over the first two days of each week, a one-hour session was held for group A and a separate one-hour session for group B. Before implementing the intervention, a pre-test was conducted to assess the students' knowledge levels on specified topics. This pre-test was administered to all four groups one day before the first intervention. A schedule was developed to present specialized topics, with study resources determined by the professor in agreement with the students. Each student was required to study the assigned content and prepare ten questions with varying difficulty levels (easy, medium, and hard) and in different formats (e.g., short answer, multiple choice), along with their correct answers. The professor reviewed and approved these questions before the round commenced.
Based on the pre-determined schedule, the professor presented the relevant case information to the group during the sessions. Students took turns answering questions, receiving scores between 1 and 3 based on their responses, with the correct answers provided by the professor. If a student answered correctly, they chose the next student to respond; if not, the first student selected the next participant. This process continued until a "champion" student was identified based on accumulated points. Throughout the session, the professor acted as an active listener, closely monitoring the students' responses to ensure all aspects of the case were addressed.
For the control groups (C and D), the same instances taught to the intervention groups using the "doughnut round" method were presented by the professor through lectures without requiring the students to study the material beforehand. These lectures were delivered two days weekly in a virtual format, accompanied by questions and answers. The intervention lasted for three months, totaling 12 weeks, during which 48 sessions were conducted—24 sessions for the intervention group and 24 sessions for the control group. Two weeks after the last post-test session, intervention and control were taken from all four groups with the same written test used in the pre-test.
Data analysis
Data analysis used descriptive and inferential statistics to test the research hypotheses. Descriptive statistical indices, such as the mean and standard deviation, were used to describe the collected data. The Kolmogorov-Smirnov test (KS test) was conducted first to check the distribution of the data. Since the data were found to be normally distributed, independent, and paired t-tests, Analysis of Covariance (ANCOVA) was used to remove the effect of intervening variables using statistical methods to obtain the results more accurately. All statistical procedures were conducted using the SPSS-16 software. Random numbers between 0 and 40 were generated to determine groups, and participants were assigned to groups based on whether each number was odd or even. Odd numbers resulted in assignment to group A (control group), while even numbers assigned participants to group B (intervention group). This process continued until two groups of 20 participants were formed. To enhance the rigor of randomization, we used the Excel random allocation function to assign participants, ensuring an equal distribution in both the "doughnut round teaching" group (n = 20) and the "conventional lecture training" group (n = 20).
Blinding was carefully maintained throughout the study to reduce bias. The participants and the individuals responsible for data collection and analysis needed to be made aware of group assignments. Given the nature of the intervention, only the allocation codes (A for the intervention group and B for the control group) were recorded, and data collection forms did not reveal which intervention was associated with each code.
To further ensure unbiased allocation, an independent third party, who had no role in the study's execution or data analysis, performed the randomization. This individual's sole role was to handle the randomization process and assign codes based on the random number sequence. This prevented any direct influence from the research team on group assignments, ensuring the integrity of the blinding and randomization process.
Results
The data in Table 1 illustrates the age distribution of the research sample across the two groups, intervention and control. It indicates that most participants fall within the age range of 23 years. Furthermore, the independent t-test results reveal no statistically significant difference in the average age between the two groups, with values reported as t = 1.912 and p = 0.058. This suggests that age may not be a differentiating factor between this study's intervention and control groups. The data presented in Table 1 outlines the gender distribution of the research sample within the two groups. In the intervention group, 53% of participants were female and 47% were male. In contrast, 54% were female in the control group and 46% were male. The Chi-square test results indicate no statistically significant difference in gender composition between the two groups (χ²(1) = 0.426, p = 0.692).
Table1. Distribution of the statistical sample according to age, gender, residence status in two groups

Abbreviations: M, Mean; SD, standard deviation; F, Frequency; X2, Chi-square test; Sig, statistical significance.
Additionally, the table provides information on the residence status of the participants. It shows that 38% of students in the intervention group live in a dormitory, compared to 46% in the control group. Furthermore, 27% of students in the intervention group reside in a private house. In comparison, 23% of those in the control group do the same. This data contributes to understanding the demographic characteristics of the sample. In addition, 35% of them in the intervention group and 31% in the control group live in rented houses. The Chi-square test results indicated no statistically significant difference between the two groups regarding their state of residence, with a p-value of 0.587. Assessing the data for normal distribution is essential before conducting various statistical tests on the collected data. To accomplish this, the Kolmogorov-Smirnov test was performed on the main variables of the study to evaluate their distribution characteristics. This preliminary step is crucial for ensuring that the assumptions of subsequent statistical analyses are met. The results of this study are presented in Table 2. Based on the data presented in Table 2, the significance levels obtained for the research variables are more significant than 0.05. It shows that the data has a normal distribution, and parametric statistical tests can be used to check these data.
Table 2. Kolmogorov-Smirnov test
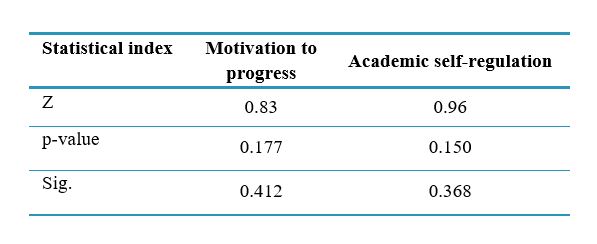
Abbreviations: p-value, probability value indicating the significance level of the correlation coefficient; Z, test statistic value; P, probability-value; Sig, statistical significance.
Table 3 demonstrates a significant difference between the average scores of both variables when comparing pre-test and post-test results among students in the two groups, with this difference being statistically significant (p < 0.0001). However, the two groups had no significant statistical difference in the pre-test scores, indicating that the mean scores were nearly identical before the intervention (p = 0.316 for the first variable and p = 0.602 for the second variable). This suggests that while the intervention had a notable impact on post-test scores, the groups started with similar baseline performances. Based on the results obtained from Levine's test, the obtained significance level (0.425) is greater than the critical value at the 0.95 level (0.05), so the prediction of the assumption of homogeneity of variance is confirmed. The results of covariance analysis show that there is a significant difference between the academic self-regulation of the intervention and control groups (p < 0.01) and F = 20.83. Its square equals 0.62; 62% of the educational self-regulation is related to implementing education through doughnut rounds. In other words, the education by doughnut round teaching method significantly affects medical students' academic self-regulation (Table 4). In addition, the results of covariance analysis in Table 5 show that there is a significant difference between the progress motivation of the intervention and control groups (p < 0.01) and F = 31.06. Its square equals 0.66; 66% of the progress motivation is related to implementing training through the doughnut round. In other words, teaching using the doughnut round method significantly affects the motivation level of medical students.
Table 3. Paired t-test to check the difference between the average scores in the pre- and post-test of students in two group

Note: Paired t-test was used to compare the mean scores of students before and after the intervention in both experimental and control groups.
Abbreviations: M, mean; SD, standard deviation; p-value, probability value indicating the significance level of the correlation coefficient; T, t-statistic value.
Table 4. The results of covariance analysis of two experimental and control groups in the level of academic self-regulation Note: Analysis of covariance (ANCOVA) was used to examine the difference in academic self-regulation between the experimental and control groups, adjusting for pre-test scores.
Note: Analysis of covariance (ANCOVA) was used to examine the difference in academic self-regulation between the experimental and control groups, adjusting for pre-test scores.
Abbreviations: F, analysis of variance test; Sig, statistical significance; p, probability-value; df, degrees of freedom.
Table 5. The results of covariance analysis of two experimental and control groups in the level of progress motivation

Note: Analysis of covariance (ANCOVA) was used to examine the difference in progress motivation between the experimental and control groups, adjusting for pre-test scores.
Abbreviations: F, analysis of variance test; Sig, statistical significance; p, probability-value; df, degrees of freedom.
Discussion
This study compared the effects of the traditional lecture and doughnut round teaching methods on medical student's academic motivation and self-regulation. Compared to the control group, the results showed a significant improvement in academic motivation and self-regulation in the doughnut round intervention group. There were statistically significant differences between the pre-test and post-test scores (p < 0.01), indicating that students in the doughnut round teaching group demonstrated higher engagement and improved learning outcomes. The control group was given lecture-based instruction and did not see these gains. This indicates how well the doughnut round teaching method promotes self-directed skills and active learning.
Doughnut round teaching is an increasingly popular self-directed learning technique that is being progressively added to medical curricula. Self-directed learners use various resources to learn independently or with little help from others. As this skill becomes more widely acknowledged as a required competency in their education, all students pursuing clinical fields should acquire it [10]. Evidence has shown that the self-directed learning approach has many advantages over direct training, such as lectures [11]. Studies [10-12] show that, in addition to being used in medicine, doughnut rounds have also been used as informal discussion sessions for curriculum development in other disciplines, such as nursing, and have recently become popular at Oxford University. It has achieved a lot, and so far, it has been used to teach undergraduate students various subjects such as surgery, anatomy, pediatrics, emergency, and medicine. Professors can implement it in various other subjects.
The self-regulation strategy is one of the most important internal factors contributing to academic progress. It facilitates learning and helps students manage their behavior by enabling them to respond to the stimuli they create themselves. For this reason, it has always been the focus of education specialists and the main subject of a significant part of the research conducted in the country. An investigation by Zhang and colleagues was named " Supported Self-Directed Learning of Clinical Anatomy: A Pilot Study of Doughnut Rounds." In this study, 17 first-year medical students used the doughnut round method to learn the clinical anatomy of the lower limb in small groups over six weeks (one-hour sessions). Lastly, there was a 77% increase in the students' self-confidence and an 87% increase in their lower anatomy learning rate. According to this study, using the doughnut round has
enhanced students' understanding of the lower anatomy topic. It can be applied to any number of students. A topic should be applied in different fields of medicine [10].
Bulstrode et al. [13] conducted a randomized controlled trial comparing traditional lectures and the doughnut round method of teaching medical students about trauma and orthopedics. Their study aimed to assess which teaching methods better facilitated knowledge transfer among medical students. One hundred six students from Oxford university participated in the trial, and they were randomly divided into two groups: one receiving traditional lectures and the other undergoing the doughnut round method. The researchers administered a pre-test, followed by three post-tests conducted at different intervals: one at the end of the 4th week, another at the end of the 10th week, and the last at the end of the 17th week. The average scores from both teaching methods were compared across these three-time points. The results indicated that the doughnut round method yielded average scores of 41.0 in the 4th week, 36.3 in the 10th week, and 38.7 in the 17th week. In comparison, the lecture method achieved averages of 40.1 in the 4th week, 37.3 in the 10th week, and 38.1 in the 17th week. No significant differences between the two methods were observed at these three stages. This study concluded that the doughnut round method was less effective than the lecture method for teaching trauma concepts, contrasting our findings.
The key findings of our study, which indicate significant improvements in self-regulation and academic motivation using the doughnut round method, are directly compared to similar results from the studies conducted by Zhang et al. [10]. Furthermore, the distinctions found in the study by Bulstrode et al., [13] that contrasted the lecture and doughnut round approaches to teaching trauma concepts have been thoroughly examined. The type of instruction, indicating that the doughnut round teaching approach works best in subjects that call for greater self-control and active engagement, explains these variations.
Another research project used the doughnut rounds method at a university to promote active learning in a large class setting. It proved that this interactive approach raised students' confidence in their subject matter and enhanced engagement. According to feedback, students enjoyed the format more than traditional lectures, which support the idea that group learning can greatly impact knowledge retention and academic achievement [27]. The results of these studies are consistent with the present study's findings and show the positive effect of implementing the doughnut round teaching.
The active engagement of students in the doughnut round teaching method has led to improved learning of the course material. As a result, they have obtained more academic self-regulation scores in the knowledge assessment test. At the same time, the learners who participate in the lecture method sometimes forget the material due to relying on their memory. Hence, the probability of remembering that material during the test is low. This result confirms that implementing the doughnut round method compared to the lecture method has a tremendous effect on increasing the motivation and understanding of learners. In other words, the doughnut round teaching method encourages more serious participation and higher levels of engagement from learners. This creates a more conducive environment for understanding relationships, ultimately leading to more stable learning outcomes for them [19-20]. Therefore, they can have a deeper understanding of educational materials by better using their power of reasoning and judgment in the context of the topics raised in the class.
According to Sohrabi et al., teaching operating room nursing students—especially those in their senior year—through the virtual doughnut round method is more effective than traditional lectures [28]. In a study Ratelle JT et al concluded that doughnut rounds have been used successfully in marine science classes to encourage student participation. Compared to traditional teaching methods, the results show that students felt more engaged and could better connect theoretical concepts with real-world applications [29]. In a study, Bulstrode et al. [30] hinted at how doughnut rounds affect medical students' clinical reasoning abilities and their self-assurance when using these abilities in practical situations. The authors discovered that students' confidence and teamwork had considerably increased. In a study, Elbasateeny et al. [31] found that various creative teaching techniques, such as doughnut rounds, improve medical trainees' teamwork and communication. According to the results, these rounds promote a more cooperative learning atmosphere.
Our findings align with earlier research, showing that the doughnut round teaching approach significantly improves student motivation, self-control, and engagement. Ratelle JT et al [29], for example, showed how the doughnut round method enhances student engagement and connection to the subject matter by encouraging active learning in marine science education. Similarly, Bulstrode et al. [30] discovered that medical students expressed greater confidence and enhanced clinical reasoning abilities after introducing doughnut rounds. Elbasateeny et al. [31-32] also emphasized how this creative strategy encourages trainee cooperation and communication, which supports the doughnut round method's efficacy in educational settings. Together, these studies support the doughnut round teaching method's beneficial effects on student learning outcomes, consistent with the notable gains we found in our research.
The doughnut round-based teaching approach facilitates learning, fosters deep learning, and boosts student participation and self-regulation abilities. This method should be used more in the education of learners in various fields of medical sciences.
One of the main limitations of this study was the relatively small sample size, which may restrict the generalizability of the results to larger populations. Also, more than three months of intervention implementation (three months) may be required to fully evaluate the long-term effects of the doughnut round method on self-regulation and achievement motivation. Other limitations include using self-report questionnaires to assess motivational and self-regulatory variables, which may have been affected by subjective factors or response bias. Also, this study was conducted in a specific educational environment, and its results may need to be more generalizable to other universities or academic fields.
Several integrated steps are recommended to implement the doughnut round teaching method effectively in medical education. Training workshops can be conducted to familiarize faculty members with key tactics, like time management during rounds and fostering an interactive environment, so they can successfully incorporate this method into their instruction. Designating particular interactive learning spaces in educational institutions can also enhance the collaborative nature of this approach by motivating students to engage with the material and actively participate.
Examining a hybrid teaching model that incorporates aspects of doughnut rounds with traditional lectures could improve student engagement and accommodate a variety of learning styles, especially considering the benefits of combining traditional and interactive techniques. Lastly, longitudinal studies that monitor students' self-regulation, academic motivation, and clinical competencies over time offer essential insights into the efficacy of this approach and validate its role in comprehensive medical training to assess its long-term benefits.
Conclusion
The results of this study indicated a statistically significant difference in academic self-regulation and motivation to progress between the pre-test and post-test scores in the intervention group. However, this difference was not significant in the control or speech group. The importance of incorporating new teaching methods in medical education has been increasingly recognized in recent years. Doughnut-round teaching has proven to be an effective educational intervention for medical students in various educational settings. Innovative teaching methods, such as doughnut-round teaching, can significantly enhance students' academic performance.
Ethical considerations
Ethical considerations in conducting research involve several essential practices, including obtaining approval from the university's ethics committee, securing informed consent from participants, ensuring anonymity for those involved, providing participants with necessary explanations and objectives of the study, and allowing individuals the right to withdraw from the study at any time. This study received approval from the Ethics Committee of Kermanshah University of Medical Sciences (IR.KUMS.REC.1401.490), and written informed consent was obtained from each participant. It is important to note that this study focused on educational strategies and new teaching methods rather than a clinical study—research code number 4020013.
Artificial intelligence utilization for article writing
The authors confirm that no artificial intelligence tools were used to create or draft this article. However, AI-based tools were selectively employed for minor editing tasks to enhance clarity and coherence, including suggestions in sections such as recommendations. All core content, analysis, and original contributions result from the authors' independent work and expertise.
Acknowledgment
The authors of this research wish to express their gratitude to the participants for their hard work and dedicated cooperation during the study.
Conflict of interest statement
The authors declare no conflicts of interest.
Author contributions
E.K., G.R., A.K., and R.R.T., who conducted data collection and computerization while E.K. analyzed the data, conceptualized this study. Simultaneously, R.R.T., G.R., and M.B. managed data treatment and interpretation. A.B. and G.P. drafted the manuscript, with E.K., G.R., and A.K. supervising and critically revising the article, contributing significant content. A.K. also performed language revisions on the manuscript. All authors have read and approved the final version of the article.
Funding
Kermanshah University of Medical Sciences provided the funding for this research.
Data availability statement
The datasets used and analyzed during the current study are available from the Corresponding author on reasonable request.
Background & Objective: In medical education, effective teaching/learning strategies are crucial, especially those that improve academic motivation and self-control. The aim of this study was to evaluate how the doughnut round teaching method versus the traditional lecture approach affected medical students’ motivation and self-regulation.
Materials & Methods: Forty medical students participated in this semi-experimental study. The participants were divided into two groups using the random allocation method through Excel software: The A group was doughnut (20 students), while the B group followed lecture methods (20 students). Both before and after the intervention, assessments were conducted using Hatter's academic motivation scale and Bouffard's self-regulation scale. ANCOVA, the independent t-test, the paired t-test, and the Kolmogorov-Smirnov test were among the statistics we employed for data analysis. Software called SPSS version 16 was used for all of our analyses.
Results: The treatment group demonstrated significant improvements in academic motivation (p < 0.001) and self-regulation (p < 0.001) in the post-test, while the control group showed no significant changes. The experimental group's pre-test and post-test scores significantly differed, indicating the effectiveness of the doughnut round teaching method in enhancing self-control and motivation.
Conclusion: The round doughnut round teaching technique significantly outperformed the standard lecture style in terms of students' academic motivation and self-regulation. This approach promotes independent study and active participation, which may improve academic performance in medical school.
Introduction
1. The average academic self-regulation score of medical students before the intervention is different in the experimental and control groups.
2. There is a difference in the average academic self-regulation score of medical students after the intervention in the experimental and control groups.
3. There is a difference between the mean score of medical students' academic achievement motivation before and after the intervention in the control group.
4. There is a difference between the mean scores of medical students' academic achievement motivation before and after the intervention in the experimental group.
5. The average score of self-regulation and academic achievement motivation of medical students in the experimental and a control group is different based on demographic characteristics.
Materials & Methods
Design and setting(s)
This semi-experimental study was conducted on 40 medical students (20 people in each group) at Kermanshah University of Medical Sciences. The current study is a semi-experimental study of pre-test and post-test types with random assignment to two control and experimental groups, in which the effect of the doughnut round teaching and lecture method was studied. Before the intervention, both groups responded to Bouffard's self-regulation scale and Hatter's motivation for academic progress. At the end of the intervention, both groups responded to the tool again.
Participants and sampling
The research population consisted of medical students enrolled at Kermanshah University of Medical Sciences for the 2023-24 academic year. The sample size for this study was determined using Cohen's table to specify sample sizes for experimental studies. Considering an effect size of 1, a test power of 0.80, and a significance level of 0.05, the minimum sample size required for each group was established as 17 individuals. In addition to Cohen's formula, according to Gall et al., translated by Nasr, the criterion for selecting 15 people for each group is also based on previous studies and experts' opinions, so a 15-person sample size is considered sufficient in semi-experimental studies. (Gall M, Borg W, Gall J. Nasr AR, translator [19].Considering an anticipated dropout rate of approximately 15%, a sample size of 20 students per group was deemed appropriate.
Figure 1. CONSORT flow diagram of the study
Figure 1 presents a CONSORT flow diagram showing the study process. The participants were divided into two groups using the random allocation method through Excel software: The A group consisted of doughnuts (20 students). In contrast, the B group followed lecture methods (20 students). The eligibility criteria required students to provide informed consent and to have passed the prerequisite credits (including basic science courses and clinical preparation). The exclusion criteria included lack of consent, failure to pass prerequisite credits, and missing more than two sessions.
Tools/Instruments
Bouffard's self-regulation scale is a 14-question questionnaire designed to measure self-regulation based on Bandura's social-cognitive theory. The questions of this questionnaire are on a 5-point Likert scale (completely agree 5, agree 4, have no opinion 3, disagree 2, and completely disagree 1) and measure two factors of cognitive strategies and metacognitive strategies of self-regulation. Questions 5, 13, and 14 are scored in a reverse way; the total scores of each person can be 14-60. A higher score in each component shows a person's tendency to use that component. The overall reliability coefficient of Bouffard's self-regulation scale was obtained based on Cronbach's alpha of 0.71. The reliability of the cognitive strategies subscale is 0.70, and the metacognitive subscale is 0.68. The reliability of the above test was reported as 0.63 in research conducted by Entezari et al. [20]. In addition, the reliability of the above test was reported as 0.67 and 0.69, respectively, in the study conducted by Zamani et al. [21] and Bagheri Kerachi and Razmjoo [22]. In addition, the reliability of Bouffard's self-regulation scale in research conducted by Ghazvineh et al. [23] has been obtained.
The factor analysis results showed that the correlation coefficient between the questions is appropriate, the value load related to the factors is acceptable, and its validity is also at the desired level. bagheri mousavi and Kadivar [4] also studied the validity and reliability of Boufard's self-regulation scale. The construct validity of this questionnaire has been reported to be optimal by using correlation coefficients and factor analysis of discriminating correlation coefficients between questionnaire questions. Cronbach's alpha coefficient to measure internal consistency was 0.08. Based on this, this questionnaire can predict the scores and actual scores of the subjects. In this study, five medical education specialists confirmed the face validity of the questionnaire, and Cronbach's alpha was calculated at 0.82.
Another questionnaire was the Hatter academic motivation scale. This scale measures people's academic motivation level in the two components: Intrinsic and external motivation. This questionnaire has 33 questions; the answer to each question is on a five-point Likert scale from never to always. Also, Harter's academic motivation questionnaire has validity, reliability, and scoring. The alpha reliability coefficient was 0.83 in the study of Zare et al. [25] and 0.86 in the study of Fallahi et al. [26] The validity of this tool has been proven in the above research. In this study, five medical education specialists confirmed the face validity of the questionnaire, and Cronbach's alpha was calculated as 0.79.
Data collection methods
Before implementing the intervention, a pre-test was conducted to assess the students' knowledge levels on specified topics. This pre-test was administered to all four groups one day before the first intervention. The pre-test tool consisted of a 20-item multiple-choice questionnaire developed specifically for this study. The questions were designed based on a structured blueprint derived from core educational topics, including fever without a source, poisoning with chemicals, gastroenteritis, and neonatal jaundice. Each question followed the standards of the Millman checklist to ensure relevance and thorough content coverage. The questions were initially drafted based on key topics within the clinical curriculum and refined with input from five clinical education specialists. This panel of experts reviewed each question for clarity, relevance, and alignment with the educational objectives to establish face and content validity. To assess the reliability of the test, Cronbach's alpha was calculated and yielded a coefficient of 0.78, indicating acceptable internal consistency. This suggests that the test provides a reliable measure of students' baseline knowledge in the specified topics. Each correct answer was assigned one point, with 20 points possible. This score provided a baseline index for each student's knowledge of the selected clinical topics.
In the intervention implementation stage, the training for the intervention group began one day after the pre-test. Over the first two days of each week, a one-hour session was held for group A and a separate one-hour session for group B. Before implementing the intervention, a pre-test was conducted to assess the students' knowledge levels on specified topics. This pre-test was administered to all four groups one day before the first intervention. A schedule was developed to present specialized topics, with study resources determined by the professor in agreement with the students. Each student was required to study the assigned content and prepare ten questions with varying difficulty levels (easy, medium, and hard) and in different formats (e.g., short answer, multiple choice), along with their correct answers. The professor reviewed and approved these questions before the round commenced.
Based on the pre-determined schedule, the professor presented the relevant case information to the group during the sessions. Students took turns answering questions, receiving scores between 1 and 3 based on their responses, with the correct answers provided by the professor. If a student answered correctly, they chose the next student to respond; if not, the first student selected the next participant. This process continued until a "champion" student was identified based on accumulated points. Throughout the session, the professor acted as an active listener, closely monitoring the students' responses to ensure all aspects of the case were addressed.
For the control groups (C and D), the same instances taught to the intervention groups using the "doughnut round" method were presented by the professor through lectures without requiring the students to study the material beforehand. These lectures were delivered two days weekly in a virtual format, accompanied by questions and answers. The intervention lasted for three months, totaling 12 weeks, during which 48 sessions were conducted—24 sessions for the intervention group and 24 sessions for the control group. Two weeks after the last post-test session, intervention and control were taken from all four groups with the same written test used in the pre-test.
Data analysis
Data analysis used descriptive and inferential statistics to test the research hypotheses. Descriptive statistical indices, such as the mean and standard deviation, were used to describe the collected data. The Kolmogorov-Smirnov test (KS test) was conducted first to check the distribution of the data. Since the data were found to be normally distributed, independent, and paired t-tests, Analysis of Covariance (ANCOVA) was used to remove the effect of intervening variables using statistical methods to obtain the results more accurately. All statistical procedures were conducted using the SPSS-16 software. Random numbers between 0 and 40 were generated to determine groups, and participants were assigned to groups based on whether each number was odd or even. Odd numbers resulted in assignment to group A (control group), while even numbers assigned participants to group B (intervention group). This process continued until two groups of 20 participants were formed. To enhance the rigor of randomization, we used the Excel random allocation function to assign participants, ensuring an equal distribution in both the "doughnut round teaching" group (n = 20) and the "conventional lecture training" group (n = 20).
Blinding was carefully maintained throughout the study to reduce bias. The participants and the individuals responsible for data collection and analysis needed to be made aware of group assignments. Given the nature of the intervention, only the allocation codes (A for the intervention group and B for the control group) were recorded, and data collection forms did not reveal which intervention was associated with each code.
To further ensure unbiased allocation, an independent third party, who had no role in the study's execution or data analysis, performed the randomization. This individual's sole role was to handle the randomization process and assign codes based on the random number sequence. This prevented any direct influence from the research team on group assignments, ensuring the integrity of the blinding and randomization process.
Results
The data in Table 1 illustrates the age distribution of the research sample across the two groups, intervention and control. It indicates that most participants fall within the age range of 23 years. Furthermore, the independent t-test results reveal no statistically significant difference in the average age between the two groups, with values reported as t = 1.912 and p = 0.058. This suggests that age may not be a differentiating factor between this study's intervention and control groups. The data presented in Table 1 outlines the gender distribution of the research sample within the two groups. In the intervention group, 53% of participants were female and 47% were male. In contrast, 54% were female in the control group and 46% were male. The Chi-square test results indicate no statistically significant difference in gender composition between the two groups (χ²(1) = 0.426, p = 0.692).
Table1. Distribution of the statistical sample according to age, gender, residence status in two groups
Abbreviations: M, Mean; SD, standard deviation; F, Frequency; X2, Chi-square test; Sig, statistical significance.
Additionally, the table provides information on the residence status of the participants. It shows that 38% of students in the intervention group live in a dormitory, compared to 46% in the control group. Furthermore, 27% of students in the intervention group reside in a private house. In comparison, 23% of those in the control group do the same. This data contributes to understanding the demographic characteristics of the sample. In addition, 35% of them in the intervention group and 31% in the control group live in rented houses. The Chi-square test results indicated no statistically significant difference between the two groups regarding their state of residence, with a p-value of 0.587. Assessing the data for normal distribution is essential before conducting various statistical tests on the collected data. To accomplish this, the Kolmogorov-Smirnov test was performed on the main variables of the study to evaluate their distribution characteristics. This preliminary step is crucial for ensuring that the assumptions of subsequent statistical analyses are met. The results of this study are presented in Table 2. Based on the data presented in Table 2, the significance levels obtained for the research variables are more significant than 0.05. It shows that the data has a normal distribution, and parametric statistical tests can be used to check these data.
Table 2. Kolmogorov-Smirnov test
Abbreviations: p-value, probability value indicating the significance level of the correlation coefficient; Z, test statistic value; P, probability-value; Sig, statistical significance.
Table 3 demonstrates a significant difference between the average scores of both variables when comparing pre-test and post-test results among students in the two groups, with this difference being statistically significant (p < 0.0001). However, the two groups had no significant statistical difference in the pre-test scores, indicating that the mean scores were nearly identical before the intervention (p = 0.316 for the first variable and p = 0.602 for the second variable). This suggests that while the intervention had a notable impact on post-test scores, the groups started with similar baseline performances. Based on the results obtained from Levine's test, the obtained significance level (0.425) is greater than the critical value at the 0.95 level (0.05), so the prediction of the assumption of homogeneity of variance is confirmed. The results of covariance analysis show that there is a significant difference between the academic self-regulation of the intervention and control groups (p < 0.01) and F = 20.83. Its square equals 0.62; 62% of the educational self-regulation is related to implementing education through doughnut rounds. In other words, the education by doughnut round teaching method significantly affects medical students' academic self-regulation (Table 4). In addition, the results of covariance analysis in Table 5 show that there is a significant difference between the progress motivation of the intervention and control groups (p < 0.01) and F = 31.06. Its square equals 0.66; 66% of the progress motivation is related to implementing training through the doughnut round. In other words, teaching using the doughnut round method significantly affects the motivation level of medical students.
Table 3. Paired t-test to check the difference between the average scores in the pre- and post-test of students in two group
Note: Paired t-test was used to compare the mean scores of students before and after the intervention in both experimental and control groups.
Abbreviations: M, mean; SD, standard deviation; p-value, probability value indicating the significance level of the correlation coefficient; T, t-statistic value.
Table 4. The results of covariance analysis of two experimental and control groups in the level of academic self-regulation
Abbreviations: F, analysis of variance test; Sig, statistical significance; p, probability-value; df, degrees of freedom.
Table 5. The results of covariance analysis of two experimental and control groups in the level of progress motivation
Note: Analysis of covariance (ANCOVA) was used to examine the difference in progress motivation between the experimental and control groups, adjusting for pre-test scores.
Abbreviations: F, analysis of variance test; Sig, statistical significance; p, probability-value; df, degrees of freedom.
Discussion
This study compared the effects of the traditional lecture and doughnut round teaching methods on medical student's academic motivation and self-regulation. Compared to the control group, the results showed a significant improvement in academic motivation and self-regulation in the doughnut round intervention group. There were statistically significant differences between the pre-test and post-test scores (p < 0.01), indicating that students in the doughnut round teaching group demonstrated higher engagement and improved learning outcomes. The control group was given lecture-based instruction and did not see these gains. This indicates how well the doughnut round teaching method promotes self-directed skills and active learning.
Doughnut round teaching is an increasingly popular self-directed learning technique that is being progressively added to medical curricula. Self-directed learners use various resources to learn independently or with little help from others. As this skill becomes more widely acknowledged as a required competency in their education, all students pursuing clinical fields should acquire it [10]. Evidence has shown that the self-directed learning approach has many advantages over direct training, such as lectures [11]. Studies [10-12] show that, in addition to being used in medicine, doughnut rounds have also been used as informal discussion sessions for curriculum development in other disciplines, such as nursing, and have recently become popular at Oxford University. It has achieved a lot, and so far, it has been used to teach undergraduate students various subjects such as surgery, anatomy, pediatrics, emergency, and medicine. Professors can implement it in various other subjects.
The self-regulation strategy is one of the most important internal factors contributing to academic progress. It facilitates learning and helps students manage their behavior by enabling them to respond to the stimuli they create themselves. For this reason, it has always been the focus of education specialists and the main subject of a significant part of the research conducted in the country. An investigation by Zhang and colleagues was named " Supported Self-Directed Learning of Clinical Anatomy: A Pilot Study of Doughnut Rounds." In this study, 17 first-year medical students used the doughnut round method to learn the clinical anatomy of the lower limb in small groups over six weeks (one-hour sessions). Lastly, there was a 77% increase in the students' self-confidence and an 87% increase in their lower anatomy learning rate. According to this study, using the doughnut round has
enhanced students' understanding of the lower anatomy topic. It can be applied to any number of students. A topic should be applied in different fields of medicine [10].
Bulstrode et al. [13] conducted a randomized controlled trial comparing traditional lectures and the doughnut round method of teaching medical students about trauma and orthopedics. Their study aimed to assess which teaching methods better facilitated knowledge transfer among medical students. One hundred six students from Oxford university participated in the trial, and they were randomly divided into two groups: one receiving traditional lectures and the other undergoing the doughnut round method. The researchers administered a pre-test, followed by three post-tests conducted at different intervals: one at the end of the 4th week, another at the end of the 10th week, and the last at the end of the 17th week. The average scores from both teaching methods were compared across these three-time points. The results indicated that the doughnut round method yielded average scores of 41.0 in the 4th week, 36.3 in the 10th week, and 38.7 in the 17th week. In comparison, the lecture method achieved averages of 40.1 in the 4th week, 37.3 in the 10th week, and 38.1 in the 17th week. No significant differences between the two methods were observed at these three stages. This study concluded that the doughnut round method was less effective than the lecture method for teaching trauma concepts, contrasting our findings.
The key findings of our study, which indicate significant improvements in self-regulation and academic motivation using the doughnut round method, are directly compared to similar results from the studies conducted by Zhang et al. [10]. Furthermore, the distinctions found in the study by Bulstrode et al., [13] that contrasted the lecture and doughnut round approaches to teaching trauma concepts have been thoroughly examined. The type of instruction, indicating that the doughnut round teaching approach works best in subjects that call for greater self-control and active engagement, explains these variations.
Another research project used the doughnut rounds method at a university to promote active learning in a large class setting. It proved that this interactive approach raised students' confidence in their subject matter and enhanced engagement. According to feedback, students enjoyed the format more than traditional lectures, which support the idea that group learning can greatly impact knowledge retention and academic achievement [27]. The results of these studies are consistent with the present study's findings and show the positive effect of implementing the doughnut round teaching.
The active engagement of students in the doughnut round teaching method has led to improved learning of the course material. As a result, they have obtained more academic self-regulation scores in the knowledge assessment test. At the same time, the learners who participate in the lecture method sometimes forget the material due to relying on their memory. Hence, the probability of remembering that material during the test is low. This result confirms that implementing the doughnut round method compared to the lecture method has a tremendous effect on increasing the motivation and understanding of learners. In other words, the doughnut round teaching method encourages more serious participation and higher levels of engagement from learners. This creates a more conducive environment for understanding relationships, ultimately leading to more stable learning outcomes for them [19-20]. Therefore, they can have a deeper understanding of educational materials by better using their power of reasoning and judgment in the context of the topics raised in the class.
According to Sohrabi et al., teaching operating room nursing students—especially those in their senior year—through the virtual doughnut round method is more effective than traditional lectures [28]. In a study Ratelle JT et al concluded that doughnut rounds have been used successfully in marine science classes to encourage student participation. Compared to traditional teaching methods, the results show that students felt more engaged and could better connect theoretical concepts with real-world applications [29]. In a study, Bulstrode et al. [30] hinted at how doughnut rounds affect medical students' clinical reasoning abilities and their self-assurance when using these abilities in practical situations. The authors discovered that students' confidence and teamwork had considerably increased. In a study, Elbasateeny et al. [31] found that various creative teaching techniques, such as doughnut rounds, improve medical trainees' teamwork and communication. According to the results, these rounds promote a more cooperative learning atmosphere.
Our findings align with earlier research, showing that the doughnut round teaching approach significantly improves student motivation, self-control, and engagement. Ratelle JT et al [29], for example, showed how the doughnut round method enhances student engagement and connection to the subject matter by encouraging active learning in marine science education. Similarly, Bulstrode et al. [30] discovered that medical students expressed greater confidence and enhanced clinical reasoning abilities after introducing doughnut rounds. Elbasateeny et al. [31-32] also emphasized how this creative strategy encourages trainee cooperation and communication, which supports the doughnut round method's efficacy in educational settings. Together, these studies support the doughnut round teaching method's beneficial effects on student learning outcomes, consistent with the notable gains we found in our research.
The doughnut round-based teaching approach facilitates learning, fosters deep learning, and boosts student participation and self-regulation abilities. This method should be used more in the education of learners in various fields of medical sciences.
One of the main limitations of this study was the relatively small sample size, which may restrict the generalizability of the results to larger populations. Also, more than three months of intervention implementation (three months) may be required to fully evaluate the long-term effects of the doughnut round method on self-regulation and achievement motivation. Other limitations include using self-report questionnaires to assess motivational and self-regulatory variables, which may have been affected by subjective factors or response bias. Also, this study was conducted in a specific educational environment, and its results may need to be more generalizable to other universities or academic fields.
Several integrated steps are recommended to implement the doughnut round teaching method effectively in medical education. Training workshops can be conducted to familiarize faculty members with key tactics, like time management during rounds and fostering an interactive environment, so they can successfully incorporate this method into their instruction. Designating particular interactive learning spaces in educational institutions can also enhance the collaborative nature of this approach by motivating students to engage with the material and actively participate.
Examining a hybrid teaching model that incorporates aspects of doughnut rounds with traditional lectures could improve student engagement and accommodate a variety of learning styles, especially considering the benefits of combining traditional and interactive techniques. Lastly, longitudinal studies that monitor students' self-regulation, academic motivation, and clinical competencies over time offer essential insights into the efficacy of this approach and validate its role in comprehensive medical training to assess its long-term benefits.
Conclusion
The results of this study indicated a statistically significant difference in academic self-regulation and motivation to progress between the pre-test and post-test scores in the intervention group. However, this difference was not significant in the control or speech group. The importance of incorporating new teaching methods in medical education has been increasingly recognized in recent years. Doughnut-round teaching has proven to be an effective educational intervention for medical students in various educational settings. Innovative teaching methods, such as doughnut-round teaching, can significantly enhance students' academic performance.
Ethical considerations
Ethical considerations in conducting research involve several essential practices, including obtaining approval from the university's ethics committee, securing informed consent from participants, ensuring anonymity for those involved, providing participants with necessary explanations and objectives of the study, and allowing individuals the right to withdraw from the study at any time. This study received approval from the Ethics Committee of Kermanshah University of Medical Sciences (IR.KUMS.REC.1401.490), and written informed consent was obtained from each participant. It is important to note that this study focused on educational strategies and new teaching methods rather than a clinical study—research code number 4020013.
Artificial intelligence utilization for article writing
The authors confirm that no artificial intelligence tools were used to create or draft this article. However, AI-based tools were selectively employed for minor editing tasks to enhance clarity and coherence, including suggestions in sections such as recommendations. All core content, analysis, and original contributions result from the authors' independent work and expertise.
Acknowledgment
The authors of this research wish to express their gratitude to the participants for their hard work and dedicated cooperation during the study.
Conflict of interest statement
The authors declare no conflicts of interest.
Author contributions
E.K., G.R., A.K., and R.R.T., who conducted data collection and computerization while E.K. analyzed the data, conceptualized this study. Simultaneously, R.R.T., G.R., and M.B. managed data treatment and interpretation. A.B. and G.P. drafted the manuscript, with E.K., G.R., and A.K. supervising and critically revising the article, contributing significant content. A.K. also performed language revisions on the manuscript. All authors have read and approved the final version of the article.
Funding
Kermanshah University of Medical Sciences provided the funding for this research.
Data availability statement
The datasets used and analyzed during the current study are available from the Corresponding author on reasonable request.
Article Type : Orginal Research |
Subject:
Medical Education
Received: 2024/08/31 | Accepted: 2025/02/5 | Published: 2025/04/14
Received: 2024/08/31 | Accepted: 2025/02/5 | Published: 2025/04/14
References
1. Sharif MR, Azadchahr MJ, Jafari M, Khademian Z. Quality assessment of clinical rounds at Kashan university of medical sciences based on clinical education standards. Development Strategies in Medical Education. 2021;8(4):11-20. [Online]. Available from: [Accessed: Mar. 22, 2021] [Article]
2. Gregory D, Guse L, Davidson D, Davis P, Russell CK. What clinical learning contracts reveal about nursing education and patient safety. Canadian Nurse. 2009;105(8). [Online]. Available from: [Accessed: Feb. 10, 2009] [Article]
3. Wilson G. Redesigning OR orientation. AORN Journal. 2012;95(4):453-6. [Article]
4. Kim KH. Clinical competence among senior nursing students after their preceptorship experiences. Journal of Professional Nursing. 2007;23(6):369-75 []
5. Ter Brugge, B.P., Fegg, L.S. & Wijnen-Meijer, M. Preparing medical students for their educational task as physicians: important, desirable and unexplored territory. BMC Med Educ 24, 391 (2024) [Article]
6. Angelopoulou P, Panagopoulou E. Non-clinical rounds in hospital settings: a scoping review. Journal of Health Organization and Management. 2019;33(5):605-16 [Article]
7. Dolcourt JL, Zuckerman G, Warner K. Learners' decisions for attending pediatric grand rounds: a qualitative and quantitative study. BMC Medical Education. 2006;6(1):1-8. [Online]. Available from: [Accessed: Jun. 17, 2006] [Article]
8. Rajasoorya C. Clinical ward rounds-challenges and opportunities. Annals of the Academy of Medicine of Singapore. 2016;45(4):152-6. [Online]. Available from: [Accessed: Apr. 4, 2016] [Article]
9. Sarikaya O, Civaner M, Kalaca S. The anxieties of medical students related to clinical training. International Journal of Clinical Practice. 2006;60(11):1414-8 [Article]
10. Zhang Y, Zerafa Simler MA, Stabile I. Supported self-directed learning of clinical anatomy: a pilot study of doughnut rounds. European Journal of Anatomy. 2017;21(4):319-24. [Online]. Available from: [Accessed: Mar. 14, 2017] [Article]
11. Ratelle JT, Gallagher CN, Sawatsky AP, et al. The Effect of Bedside Rounds on Learning Outcomes in Medical Education: A Systematic Review. Academic Medicine. 2022 Jun 1;97(6):923-930 [Article]
12. Fleiszer D, Fleiszer T, Russell R. Doughnut rounds: a self-directed learning approach to teaching critical care in surgery. Medical Teacher. 2009;19(3):190-3 [Article]
13. Bulstrode C, Gallagher FA, Pilling EL, Furniss D, Proctor RD. A randomised controlled trial comparing two methods of teaching medical students trauma and orthopaedics: traditional lectures versus the "donut round". Surgeon. 2003 Apr;1(2):76-80. [Article]
14. Wang H, Sun Y, Zhao X, et al. Enhancing academic engagement through students' perceptions of teacher expectations: the mediating role of intentional self-regulation in middle school. Frontiers Psychology. 2024 Oct 24; 15:1456334. [Article]
15. Opdenakker MC. Developments in early adolescents' self-regulation: The importance of teachers' supportive vs. undermining behavior. Front Psychol. 2022 Nov 23;13:1021904 [Article]
16. Ballouk R, Mansour V, Dalziel B, et al. Medical students' self-regulation of learning in a blended learning environment: a systematic scoping review. Medical Education. 2022 Dec;27(1):2029336 [Article]
17. Rezaei B. Quality of clinical education (a case study in the viewpoints of nursing and midwifery students in Islamic Azad university, Falavarjan branch). Education Strategies in Medical Sciences. 2016;9(2):106-17. [Online]. Available from: [Accessed: Mar. 9, 2016] [Article]
18. Shi Y, Gao H, Yan Y, Li X, Ping W, Yang H, Du Y. Career choice motivation and professionalism in medical students in China: a gender-stratified analysis. BMJ Open. 2024 Jun 10;14(6):e083073 [Article]
19. Gall M, Borg W, Gall J. Quantitative and qualitative research methods in educational sciences and psychology. Translated by Ahmad Reza Nasr, et al. 2016;1398(11). [Online]. Available from: [Accessed: Mar. 15, 2016] [Article]
20. Entezami N, Ahghar G, Shabani H. The effect of self-regulated learning on conflict resolution styles in guidance school students. New Educational Approaches. 2017;12(1):110-29 [Article]
21. Zamani BE, Saeedi Z, Abedi A. Effectiveness and sustainability of impact of using multimedia on studentsâ self-regulation and academic achievement in mathematics at high school first grade. New Educational Approaches. 2011;6(2):1-22. [Online]. Available from: [Accessed: May. 14, 2011] [Article]
22. Bagheri Kerachi A, Razmjoo MM. Comparing self-regulation in students interested in different styles of computer games. Sociology of Education. 2020;5(2):48-55 [Article]
23. Ghazvineh J, Jadidi H, Taghvaeinia A, Morovvati Z. The effect of emotional intelligence, self-regulation and assertiveness on academic satisfaction with mediation of perceived social support in students of the second high school. Journal of Research in Educational Systems. 2022;16(59):49-62 [Article]
24. Bagheri mousavi M.S, kadivar P, & Habibzadeh A. Explain The Structural Relationship Between Teachers Emotions and Classroom Management Mediated by Self-Efficacy Professors of Farhangian University. Research in Teaching, (2022).10(1),130-107 [Article]
25. Zare H, Rajabzadeh S, Moghadami N. The prediction of self-regulation strategies from thinking control components. Horizon of Medical Education Development. 2016;7(2):14-20 [Article]
26. Fallahi V, Mikaeli N, Atadokht A, Ahmadi S. The role of self-regulation and alienation in predict educational achievement motivation of students. Shenakht Journal of Psychology and Psychiatry. 2019;6(5):72-82 [Article]
27. Saha, Satyajit & Roy, Hironmoy. 'Students Perception on 'Doughnut Roughnut rounds in Self Eirected Learning of Anatomy. (2021).v8.I,12,pp:2227-8179 [Article]
28. Sohrabi Z, Rasouli D, Nouri Khaneghah Z, Ramezanpour E, Nosrati S, Zhianifard A. Comparing the effect of virtual doughnut educational rounds and online lecture methods on the learning and satisfaction of operating room nursing students; a self-directed learning method. Health Education and Health Promotion. 2024;12(1):85-9 [Article]
29. Ratelle JT, Gallagher CN, Sawatsky AP, et al. The Effect of Bedside Rounds on Learning Outcomes in Medical Education: A Systematic Review. Academic Medicine. 2022 Jun 1;97(6):923-930 [Article]
30. Bulstrode C, Gallagher FA, Pilling EL, Furniss D, Proctor RD. A randomised controlled trial comparing two methods of teaching medical students trauma and orthopaedics: traditional lectures versus the “donut round”. The Surgeon. 2003;1(2):76-80 [Article]
31. Elbasateeny SS, Yassin MA, Mokhtar MM, et al. Prognostic implications of MALAT1 and BACH1 expression and their correlation with CTCs and Mo‐MDSCs in triple negative breast cancer and surgical management options. International Journal of Breast Cancer. 2022; 2022(1):8096764 [Article]
32. Soltani Arabshahi K, sorabi Z, Keshavarzi M H, Ramezani G. Investigation of the Relationship between Self-determined Motivation and Work Engagement of Faculty Members of Iran University of Medical Sciences. Journal of Medical Education Development 2019; 12 (33):16-25 [Article]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
