
Wed, Aug 5, 2026
[Archive]
Volume 18, Issue 1 (2025)
J Med Edu Dev 2025, 18(1): 65-75 |
Back to browse issues page


Ethics code: (No. 482, dated 04/02/2024)
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Babakurd F, Sharaf M, Dashash M. Identification of essential competencies for the pediatric dentistry curriculum at Damascus University: A Delphi study. J Med Edu Dev 2025; 18 (1) :65-75
URL: http://edujournal.zums.ac.ir/article-1-2256-en.html
URL: http://edujournal.zums.ac.ir/article-1-2256-en.html

1- Department of Pediatric Dentistry, Faculty of Dentistry, Damascus University, Syria.
2- Department of Professor, Pediatric Dentistry, Faculty of Dentistry, Damascus. ,mdashash@yahoo.com
2- Department of Professor, Pediatric Dentistry, Faculty of Dentistry, Damascus. ,
Keywords: pediatric dentistry, educational curricula, competency-based medical education, Delphi technique.
Full-Text [PDF 863 kb]
(871 Downloads)
| Abstract (HTML) (2138 Views)
Full-Text: (356 Views)
Abstract
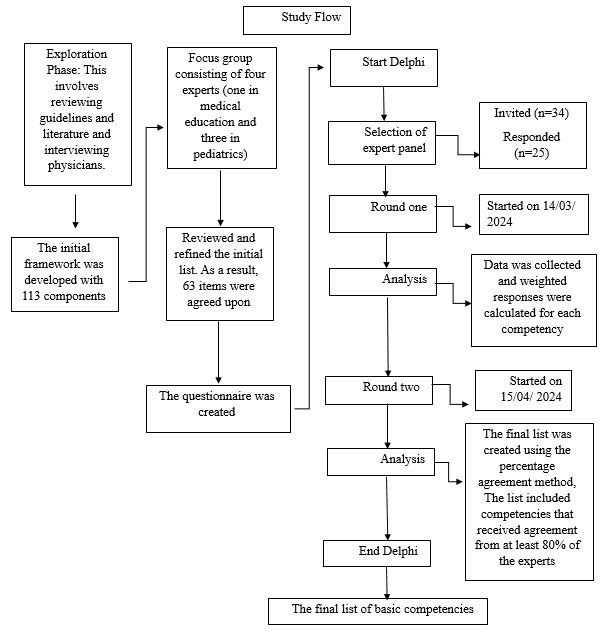
Figure. Flow chart of the study
Results
Of the 34 physicians invited to participate in the questionnaire, 25 expert physicians responded, resulting in a response rate of 73.5%. For details on the demographic characteristics of the participants, please refer to Table 1. During the focus group meetings, a preliminary list of 63 competencies was identified: 16 in the knowledge domain, 31 in the skills domain, and 16 in the attitude domain.
Table 1. Demographic characteristics of the participants
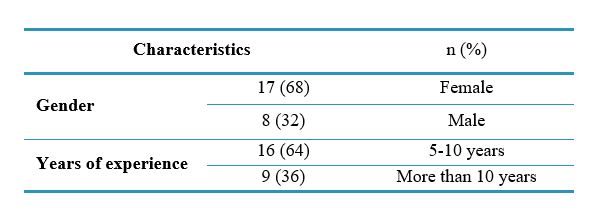
Abbreviations: n, number of participants; %, percentage.
In the first round of the Delphi process, three additional competencies were suggested, two of which were added to the knowledge domain and one to the skills domain. This brought the total to 66 competencies, distributed as follows: 18 in the knowledge domain, 32 in the skills domain, and 16 in the attitude domain.
Competencies with a weighted response of 2.5 or higher were considered during the first Delphi round. Four competencies (one from the knowledge domain and the others from the attitude domain) were excluded. This left 62 competencies for the second round, distributed as follows: 17 within the knowledge domain, 32 within the skills domain, and 13 within the attitude domain.
The second Delphi round evaluated the 62 competencies by 25 experts. The level of agreement responses ranged from neutral to agree to strongly agree, with a low standard deviation showing some homogeneity and agreement among the experts.
The last basic list was limited to the competencies rated on average higher than 4.21 (80%, being ‘strongly agree’) as valid competencies. Hence, 15 competencies (two from the knowledge domain, eleven from the skills domain, and two from the attitudes domain) that obtained an average rating of less than 4.21 were deleted (Appendix 1)
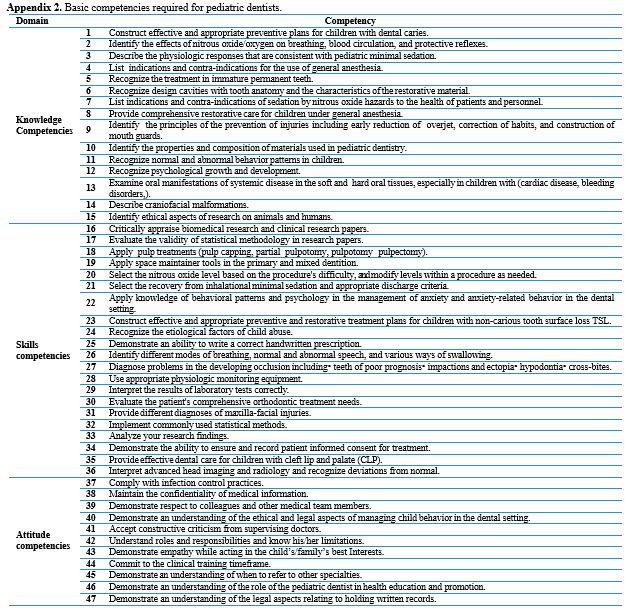
Appendix 2 presents the essential competencies assumed for postgraduate students of the Department of Pediatric Dentistry. The competencies were developed through the Delphi technique and consist of 47 items, 15 of which are on the cognitive dimension, 21 on the skills dimension, and 11 on the attitudinal dimension.
Discussion
This study focuses on the fundamental competencies that postgraduate students should possess to offer quality services to patients without compromising social accountability. The focus is most certainly on enhancing the quality of education and training, which requires developing an integrated course to fill the educational gaps [30].
A modified Delphi technique has been employed to increase the likelihood of reaching a consensus in competency identification in medical education. It comprises deliberate and progressive interactions of a specific group of specialists, and the consensus is reached through a set of systematic, interactive procedures whereby each participant can change their view and include new ones if needed [31].
This study constitutes the first attempt to define all necessary competencies for postgraduate students of pediatric dentistry curricula. The Delphi method was applied, and as a result, the panel of 25 experts agreed on 47 competencies arranged in three specific areas. These competencies will be the first step toward formulating a competencies-based program focusing on pediatric dentistry. The list incorporates important knowledge and competencies that cover general and behavior management concepts related to pediatric dentistry. It also touches upon general pediatrics and its sub-specialties, dealing with medically compromised and children with special needs, management of pain, oral medicine and surgery, techniques of sedation and general anesthesia, dental materials, interceptive orthodontics, pharmacology, epidemiology, prevention, restorative dentistry, dental trauma, research design, statistics, dental and maxillofacial radiology. Besides, the set includes the duties that the practitioners will perform. They must perform routine diagnostic and therapeutic measures, care for patients and their feelings and needs, and build trust. Dedication to self-evolution, patient safety and confidentiality, adherence to legal procedures, and obtaining informed consent are crucial aspects of a dentist's professional duty.
The optimal size of experts participating in Delphi studies varies and ranges from 5 to more than 1000 participants [32]. Loo emphasized that the purposeful selection of experts yields consensual data rather than large, randomly selected numbers [33].
A systematic review determined that most Delphi studies included ≥ 25 participants [32]. Only seven experts were included in the Delphi study by Dalkey and Helmer [34]. In comparison, this study included 25 pediatric dentistry experts with a response rate of 73.5%.
Answers were recorded using a five-point Likert scale, including a neutral point. Eliminating the neutral point may prompt respondents to adopt a clearer stance. However, its deletion results in a distortion in the responses toward negative responses, particularly in the case of ambivalent respondents [35].
This study employed two research methodologies. First, a focus group method was used to create an initial list of competencies. Second, the Delphi technique was used to restructure and develop a list of core competencies based on recommendations from previous studies [36].
The knowledge competency with the highest score was "construct effective and appropriate preventive plans for children with dental caries." This is crucial due to the significance of preventive strategies in halting caries development in children. Traditional pediatric dentistry residency program curricula have excessively emphasized restorative dentistry while neglecting early diagnosis and preventive management. This has contributed to a concerning increase in detected, missing, and filled teeth (DMFT) indicators in recent epidemiological studies conducted in Syria [37].
It is important to emphasize that preventive dentistry constitutes the most essential component of training in pediatric dentistry, as prevention is the foundation of the specialty. Previous studies have reported similar findings, highlighting that most universities in Brazil and Malaysia emphasize the knowledge and application of preventive materials in undergraduate dental education [38, 39]. The highest score regarding skill competencies was "critically appraise biomedical research and clinical research papers." Maintaining competency and continuing professional development are essential to providing up-to-date, high-quality patient care.
The postgraduate students will be able to confidently take responsibility for pediatric problems regarding evidence-based practice. They need to be equipped to research, select, analyze critically, and apply valid information based on evidence to sustain lifelong learning. Research studies in Chile and Latin America have supported the scientific basis that teaching and professional development involve research. These studies have also emphasized a need for more support, encouragement, and promotion of research culture within dental schools [40]. A study assessing the educational program given to postgraduate students in pediatric dentistry in Egypt revealed areas for improvement regarding scientific research. This was attributed to a need for more sufficient attention paid by faculty members to research and the lack of financial resources as significant obstacles to postgraduate research [41]. The data indicated that "compliance with infection control practices" was the most important attitude competency. This competency is crucial because infection control protects patients and healthcare workers, including pediatric dentists. Dentists work in an environment characterized by close contact with patients and the production of aerosols; therefore, the chances of infection transmission from an infected patient are very high. Thus, pediatric dentists should be informed and educated on the absolute adherence to infection control.
A recent review of emerging viral diseases in the new millennium concluded that infection control is as important in dental practice as understanding oral manifestations and diagnosing and managing viral infections [42]. Another important benefit of this study would be to aid the curriculum planners in making a
pediatric dentistry curriculum comprising a prioritized list of competencies established by experts.
There are several limitations of the Delphi survey. First, the repetitiveness of the survey set may easily cause a loss of interest in the participants over time, hence putting pressure on the study supervisors to keep the participants' motivation going after every round. Secondly, targeted postgraduate students participating in the study did not contribute to developing these competencies and thus may not be reflected in the identified competencies. Therefore, a comprehensive review of the pediatric dentistry curriculum is required to create appropriate structured curricular guidelines that answer the needs of learners and the community. These guidelines should standardize the content of undergraduate pediatric dentistry curricula in keeping with contemporary evidence-based dentistry, recommend the most effective educational methodology for delivering this content, and suggest the most appropriate assessment tools in light of the need to adopt a competency-based approach.
Conclusion
Forty-seven competencies have been identified that are expected to facilitate pediatric dentists' providing the highest quality patient health care. These competencies will also contribute to decision-makers developing more focused educational curricula that can dramatically enhance the evolution of competency-based education in pediatric dentistry.
Ethical considerations
This study got the Ethical Committee's approval, Damascus University, No. 482, on 04/02/2024, and it was mentioned in the introductory paragraph that this is an informed consent while filling out the electronic survey form.
Artificial intelligence utilization for article writing
Grammarly was used to correct grammar, punctuation, spelling, and paraphrasing in a critical review according to the ethical code.
Acknowledgment
The authors would like to thank all participating students and everyone who provided comments and suggestions that improved this study.
Conflict of interest statement
The authors confirm that they have no conflicting financial interests or personal relationships that could bias the work reported in this paper.
Author contributions
FB and MS collected the focus group data and employed the Delphi technique. MD oversaw the study's design and execution. FB and MD contributed to data analysis, interpretation, and manuscript drafting and reviewed the manuscript before submission. All authors have reviewed and approved the final manuscript.
Funding
Damascus University, Syria, supports this study.
Data availability statement
Data are available upon reasonable request. They are stored as de-identified participant data, which are available upon request to babakrdfarah@gmail.com.
Background & Objective: Global education is focusing on the significance of developing competency-based curricula nowadays. This study aims to establish a comprehensive set of essential competencies in pediatric dentistry designated for the curriculum at Damascus University to ensure that the graduates are equipped with the knowledge, skills, and professional attitudes to deliver effective pediatric dental care.
Materials & Methods: This qualitative exploratory study used Delphi techniques to build a consensus among experts on the core competencies of the pediatric dentistry curriculum at Damascus University in 2024. This study used two sequential qualitative methods: a focus group and the Delphi technique. A focus group was conducted with one medical education expert and three specialists in pediatric dentistry to develop an initial list of competencies. This list was assessed using a two-round Delphi technique utilized for this purpose. 25 participated in the process, and out of the 34 experts invited, Competencies that garnered at least 80% agreement among the experts were included in the final list. The analysis included descriptive statistics such as mean and standard deviation.
Results: The study identified 47 core competencies, of which 15 were related to knowledge: facts and concepts in pediatric dentistry; 21 were related to skills: abilities to perform an activity or a task; and 11 were related to attitudes: feelings or opinions that guide behavior.Conclusion: The application of theoretical knowledge acquired in various aspects of clinical education is hampered by diverse challenges. These challenges manifest at different levels, encompassing management, policy, infrastructure, and human and material resources. Prioritizing identified issues and implementing corrective actions based on existing capacities is the initial step in overcoming these challenges.
Conclusion: Identifying a comprehensive framework of essential competencies for the pediatric dentistry curriculum at Damascus University has been successfully established. This framework is good because it aligns differently with global education trends. Still, it aims to improve the dental care provided by future practitioners. The results will be an asset to the curriculum developers and educators in pediatric dentistry to ensure that graduates are better equipped to provide quality care to their young patients.
Introduction
Materials & Methods: This qualitative exploratory study used Delphi techniques to build a consensus among experts on the core competencies of the pediatric dentistry curriculum at Damascus University in 2024. This study used two sequential qualitative methods: a focus group and the Delphi technique. A focus group was conducted with one medical education expert and three specialists in pediatric dentistry to develop an initial list of competencies. This list was assessed using a two-round Delphi technique utilized for this purpose. 25 participated in the process, and out of the 34 experts invited, Competencies that garnered at least 80% agreement among the experts were included in the final list. The analysis included descriptive statistics such as mean and standard deviation.
Results: The study identified 47 core competencies, of which 15 were related to knowledge: facts and concepts in pediatric dentistry; 21 were related to skills: abilities to perform an activity or a task; and 11 were related to attitudes: feelings or opinions that guide behavior.Conclusion: The application of theoretical knowledge acquired in various aspects of clinical education is hampered by diverse challenges. These challenges manifest at different levels, encompassing management, policy, infrastructure, and human and material resources. Prioritizing identified issues and implementing corrective actions based on existing capacities is the initial step in overcoming these challenges.
Conclusion: Identifying a comprehensive framework of essential competencies for the pediatric dentistry curriculum at Damascus University has been successfully established. This framework is good because it aligns differently with global education trends. Still, it aims to improve the dental care provided by future practitioners. The results will be an asset to the curriculum developers and educators in pediatric dentistry to ensure that graduates are better equipped to provide quality care to their young patients.
Introduction
Competency-Based Medical Education (CBME) is an outcome-oriented approach focused on designing, implementing, and evaluating educational programs [1]. Its first aim is to identify the skills, knowledge, and professional attitudes that learners should be able to practice independently [2]. Knowledge entails acquiring, retaining, and effectively utilizing information, requiring mental effort and the capacity to grasp concepts while distinguishing between right and wrong. While skill aims to represent the practical application of knowledge and established rules, leading to actions guided by specific ethical principles, an example of that is balancing expected benefits with potential risks. Attitude refers to predispositions that shape how responding to a particular situation differs individually, including interpreting events, organizing opinions into coherent structures (such as values), and articulating ethical actions [3]. These competencies are defined according to the needs of patients, the community, and the health care system [4]. The advantages of CBME include developing competent clinicians who can work through problem-based learning, communicate effectively, and think critically [5]. As we all know, for graduates, competency-based education was first adopted by the University of Puerto Rico, one of the dental schools. Then, the American Association of Dental Schools took the leadership role in organizing the execution of this educational model in various specialties [6]. More recently, the National Dental Examining Board of Canada has designed a competency standard that is considered sufficient for certificate awards to dental graduates [7].
Pediatric dentistry, also known as pedodontists, is a specialty that provides both primary and comprehensive preventive and therapeutic dental care for children from birth through adolescence, including those with special needs [8]. This specialty incorporates, in addition to the distinct techniques specifically designed to address children's unique requirements, a variety of skills and procedures that are common to other dental disciplines [9]. Consequently, what is vital in pediatric dentistry is focusing on evidence-based interventions—whether preventive, diagnostic, or -therapeutic [10]. The current curriculum covers essential topics in pediatric dentistry, including behavior management techniques, preventive and restorative treatments, trauma care, and preventive and interventional orthodontics. On the contrary, it lacks modernization, depth, and timely updates on the latest advancements in these areas [11]. However, what is regrettable is that there is currently no standardized curriculum for pediatric dentistry, resulting in substantial variation in educational context across different regions. Many factors influence this disparity, including regional societal and capacity [12]. Recently, there has been a movement towards establishing universally accepted competencies and defining quality standards in education on every continent. These efforts to cover curricula are expected to promote the exchange of experiences and enhance communication and collaboration among professionals worldwide [13].
The aim is to focus and structure educational programs, and this paper argues for developing a global competency-based curriculum in pediatric dentistry. It asserts that adopting a CBME framework can achieve such an outcome. This approach effectively fosters the necessary skills, knowledge, and attitudes among learners [14, 15]. Establishing the CBME framework is crucial to identifying the competencies required to perform the job [16]. Various techniques, including expert panels and critical assessments, have been employed to determine the competencies, learner surveys, and task analysis [17]. The Delphi technique is more precisely a systematic method developed to collect expert opinions on topics that may not come under existing knowledge and concepts by consensus [18]. This method makes it easier for a group of experts engaging in structured, repetitive discussions to derive collective judgments, often more insightful than individual opinions [19]. While traditional surveys typically determine 'what is' the Delphi method focuses on "what should be" [20]. The advantages of the Delphi technique are reliability, diversity of expert opinions, and the capacity to be conducted remotely without face-to-face interaction [21]. This method allows experts to communicate anonymously and easily to exchange information, encouraging independent thought. We can enhance the validity of the content by engaging experts in multiple review rounds.
Moreover, for objectivity's sake, the technique upholds anonymity and confidentiality to avoid the influence of dominant individuals, group pressures, and groupthink. This anonymity encourages the free and frank expression of opinion, and repeating review rounds allows participants to reconsider their ideas, further enhancing the robustness of findings [22]. The Delphi technique has been used extensively in health to reach consensus and determine competencies in medical specialties [23-26]. This study aims to establish a complete umbrella set of essential competencies in pediatric dentistry, adapted for the curriculum at Damascus University, to enable graduates to possess the knowledge, skills, and professional attitudes necessary for effective pediatric dental care.
Materials & Methods
Design and setting(s)
This is a qualitative exploratory study with Delphi elements to build expert consensus on the core competencies of the pediatric dentistry curriculum at Damascus University in 2024. Two sequential qualitative methods, focus group and Delphi technique, were used.
The current research has been approved by the Scientific Research Ethics Committee of Damascus University, No. 482, dated 04/02/2024. Written informed consent was sought from the survey participants and attached to the front page of the e-questionnaire.
This study was carried out according to the recommendations of Delphi Studies (CREDES) [27].
Participants and sampling
The principal researchers, F.B. and M.S., prepared an initial list of 113 items through a comprehensive review of the medical literature and global competencies [28] and interviews with members of the Syrian Association of Pediatric Dentistry, the Dental Association, and professors of pediatric dentistry at public and private universities who are physicians. Acknowledging that the Delphi Technique has been approved over time, it is qualitative as it gathers subjective opinions and insights from experts; traditional coding might not be directly involved. This technique has been employed by designing a list of suggested competencies and gathering expert opinions to achieve consensus. The supervisor, an M.D., an expert in medical education, reviewed and refined the initial list, made the necessary changes, adjusted the wording of some competencies, and added or removed items to ensure clarity and comprehension. Following this, a focus group of four experts (one in medical education and three in pediatrics) reviewed the initial list and made necessary modifications. As a result, 63 items were agreed upon, documented, and categorized into knowledge, skills, and attitudes.
Tools/Instruments
The questionnaire was designed on Google Forms, an online survey platform. It was composed of 6 sections. Section 1 was an introduction explaining the purpose of the study and the policy protecting the privacy and confidentiality of the participants' data. Each fully completed questionnaire was assigned an identification code to keep it anonymous, considered one of the major aspects of Delphi surveys. Besides, an implied agreement is clearly stated.Section 2 gathered information on demographics: gender and years of practice. Sections 3, 4, and 5 identified the core knowledge, skills, and attitudes competencies. Section 6 had a free text field where the respondent could suggest a new competency not listed in the preliminary list.
Data collection methods
Delphi expert panel
According to Dalkey, Delphi experts are individuals with knowledge and skills in a specific field who meet four requirements: knowledge and experience of the issue, ability and willingness to participate, sufficient time to participate in the Delphi, and effective communication skills [29]. In line with these criteria, 34 experts were invited to participate, comprising faculty members from public and private universities and directors of training and specialization programs within the Department of Pediatric Dentistry of the Syrian Society of Pediatric Dentistry. Each expert had a minimum of 5 years of experience. Out of those invited, 25 experts responded, resulting in a response rate of 73.5%.
Delphi protocol-first round
During the first round, experts were asked to rate the importance of each competency on a five-point Likert scale (1 for "strongly disagree" to 5 for "strongly agree"). They were also encouraged to comment on any competencies they felt should be changed or added. The first-round survey deadline was two weeks, and reminders were sent to those who still needed to respond on the seventh day.
Delphi data analysis-first round
The competencies were reviewed based on expert feedback in the first round. Additional competencies suggested in the free-text comments were included in the second round. Data was collected, and weighted responses were calculated for each competency.
Delphi protocol-second round:
The second round consisted of a list sent to all experts to re-evaluate the importance of each competency since this list included all competencies. Their corresponding weighted responses were created, adding the new competencies suggested during the first round. Thus, the updated version was sent to them on a five-point Likert scale, considering their colleagues' responses from the first Delphi round. The second survey deadline was two weeks, and a reminder was sent on the seventh day. The first round occurred on 14/03/2024, and the second on 15/04/2024.
Delphi data analysis-second round
The agreement below was extracted using a common approach: the percentage agreement method, which establishes consensus in the Delphi technique. This method only lists competencies where at least 80% of experts agree.
Data analysis
Data analysis was done using the IBM SPSS statistical package, with descriptive statistics such as the mean of responses on the Likert scale used to determine the direction of the response and the standard deviation used to gauge the homogeneity of the responses. See Figure 1 for the study flow chart.
Pediatric dentistry, also known as pedodontists, is a specialty that provides both primary and comprehensive preventive and therapeutic dental care for children from birth through adolescence, including those with special needs [8]. This specialty incorporates, in addition to the distinct techniques specifically designed to address children's unique requirements, a variety of skills and procedures that are common to other dental disciplines [9]. Consequently, what is vital in pediatric dentistry is focusing on evidence-based interventions—whether preventive, diagnostic, or -therapeutic [10]. The current curriculum covers essential topics in pediatric dentistry, including behavior management techniques, preventive and restorative treatments, trauma care, and preventive and interventional orthodontics. On the contrary, it lacks modernization, depth, and timely updates on the latest advancements in these areas [11]. However, what is regrettable is that there is currently no standardized curriculum for pediatric dentistry, resulting in substantial variation in educational context across different regions. Many factors influence this disparity, including regional societal and capacity [12]. Recently, there has been a movement towards establishing universally accepted competencies and defining quality standards in education on every continent. These efforts to cover curricula are expected to promote the exchange of experiences and enhance communication and collaboration among professionals worldwide [13].
The aim is to focus and structure educational programs, and this paper argues for developing a global competency-based curriculum in pediatric dentistry. It asserts that adopting a CBME framework can achieve such an outcome. This approach effectively fosters the necessary skills, knowledge, and attitudes among learners [14, 15]. Establishing the CBME framework is crucial to identifying the competencies required to perform the job [16]. Various techniques, including expert panels and critical assessments, have been employed to determine the competencies, learner surveys, and task analysis [17]. The Delphi technique is more precisely a systematic method developed to collect expert opinions on topics that may not come under existing knowledge and concepts by consensus [18]. This method makes it easier for a group of experts engaging in structured, repetitive discussions to derive collective judgments, often more insightful than individual opinions [19]. While traditional surveys typically determine 'what is' the Delphi method focuses on "what should be" [20]. The advantages of the Delphi technique are reliability, diversity of expert opinions, and the capacity to be conducted remotely without face-to-face interaction [21]. This method allows experts to communicate anonymously and easily to exchange information, encouraging independent thought. We can enhance the validity of the content by engaging experts in multiple review rounds.
Moreover, for objectivity's sake, the technique upholds anonymity and confidentiality to avoid the influence of dominant individuals, group pressures, and groupthink. This anonymity encourages the free and frank expression of opinion, and repeating review rounds allows participants to reconsider their ideas, further enhancing the robustness of findings [22]. The Delphi technique has been used extensively in health to reach consensus and determine competencies in medical specialties [23-26]. This study aims to establish a complete umbrella set of essential competencies in pediatric dentistry, adapted for the curriculum at Damascus University, to enable graduates to possess the knowledge, skills, and professional attitudes necessary for effective pediatric dental care.
Materials & Methods
Design and setting(s)
This is a qualitative exploratory study with Delphi elements to build expert consensus on the core competencies of the pediatric dentistry curriculum at Damascus University in 2024. Two sequential qualitative methods, focus group and Delphi technique, were used.
The current research has been approved by the Scientific Research Ethics Committee of Damascus University, No. 482, dated 04/02/2024. Written informed consent was sought from the survey participants and attached to the front page of the e-questionnaire.
This study was carried out according to the recommendations of Delphi Studies (CREDES) [27].
Participants and sampling
The principal researchers, F.B. and M.S., prepared an initial list of 113 items through a comprehensive review of the medical literature and global competencies [28] and interviews with members of the Syrian Association of Pediatric Dentistry, the Dental Association, and professors of pediatric dentistry at public and private universities who are physicians. Acknowledging that the Delphi Technique has been approved over time, it is qualitative as it gathers subjective opinions and insights from experts; traditional coding might not be directly involved. This technique has been employed by designing a list of suggested competencies and gathering expert opinions to achieve consensus. The supervisor, an M.D., an expert in medical education, reviewed and refined the initial list, made the necessary changes, adjusted the wording of some competencies, and added or removed items to ensure clarity and comprehension. Following this, a focus group of four experts (one in medical education and three in pediatrics) reviewed the initial list and made necessary modifications. As a result, 63 items were agreed upon, documented, and categorized into knowledge, skills, and attitudes.
Tools/Instruments
The questionnaire was designed on Google Forms, an online survey platform. It was composed of 6 sections. Section 1 was an introduction explaining the purpose of the study and the policy protecting the privacy and confidentiality of the participants' data. Each fully completed questionnaire was assigned an identification code to keep it anonymous, considered one of the major aspects of Delphi surveys. Besides, an implied agreement is clearly stated.Section 2 gathered information on demographics: gender and years of practice. Sections 3, 4, and 5 identified the core knowledge, skills, and attitudes competencies. Section 6 had a free text field where the respondent could suggest a new competency not listed in the preliminary list.
Data collection methods
Delphi expert panel
According to Dalkey, Delphi experts are individuals with knowledge and skills in a specific field who meet four requirements: knowledge and experience of the issue, ability and willingness to participate, sufficient time to participate in the Delphi, and effective communication skills [29]. In line with these criteria, 34 experts were invited to participate, comprising faculty members from public and private universities and directors of training and specialization programs within the Department of Pediatric Dentistry of the Syrian Society of Pediatric Dentistry. Each expert had a minimum of 5 years of experience. Out of those invited, 25 experts responded, resulting in a response rate of 73.5%.
Delphi protocol-first round
During the first round, experts were asked to rate the importance of each competency on a five-point Likert scale (1 for "strongly disagree" to 5 for "strongly agree"). They were also encouraged to comment on any competencies they felt should be changed or added. The first-round survey deadline was two weeks, and reminders were sent to those who still needed to respond on the seventh day.
Delphi data analysis-first round
The competencies were reviewed based on expert feedback in the first round. Additional competencies suggested in the free-text comments were included in the second round. Data was collected, and weighted responses were calculated for each competency.
Delphi protocol-second round:
The second round consisted of a list sent to all experts to re-evaluate the importance of each competency since this list included all competencies. Their corresponding weighted responses were created, adding the new competencies suggested during the first round. Thus, the updated version was sent to them on a five-point Likert scale, considering their colleagues' responses from the first Delphi round. The second survey deadline was two weeks, and a reminder was sent on the seventh day. The first round occurred on 14/03/2024, and the second on 15/04/2024.
Delphi data analysis-second round
The agreement below was extracted using a common approach: the percentage agreement method, which establishes consensus in the Delphi technique. This method only lists competencies where at least 80% of experts agree.
Data analysis
Data analysis was done using the IBM SPSS statistical package, with descriptive statistics such as the mean of responses on the Likert scale used to determine the direction of the response and the standard deviation used to gauge the homogeneity of the responses. See Figure 1 for the study flow chart.
Figure. Flow chart of the study
Results
Of the 34 physicians invited to participate in the questionnaire, 25 expert physicians responded, resulting in a response rate of 73.5%. For details on the demographic characteristics of the participants, please refer to Table 1. During the focus group meetings, a preliminary list of 63 competencies was identified: 16 in the knowledge domain, 31 in the skills domain, and 16 in the attitude domain.
Table 1. Demographic characteristics of the participants
Abbreviations: n, number of participants; %, percentage.
In the first round of the Delphi process, three additional competencies were suggested, two of which were added to the knowledge domain and one to the skills domain. This brought the total to 66 competencies, distributed as follows: 18 in the knowledge domain, 32 in the skills domain, and 16 in the attitude domain.
Competencies with a weighted response of 2.5 or higher were considered during the first Delphi round. Four competencies (one from the knowledge domain and the others from the attitude domain) were excluded. This left 62 competencies for the second round, distributed as follows: 17 within the knowledge domain, 32 within the skills domain, and 13 within the attitude domain.
The second Delphi round evaluated the 62 competencies by 25 experts. The level of agreement responses ranged from neutral to agree to strongly agree, with a low standard deviation showing some homogeneity and agreement among the experts.
The last basic list was limited to the competencies rated on average higher than 4.21 (80%, being ‘strongly agree’) as valid competencies. Hence, 15 competencies (two from the knowledge domain, eleven from the skills domain, and two from the attitudes domain) that obtained an average rating of less than 4.21 were deleted (Appendix 1)
Appendix 2 presents the essential competencies assumed for postgraduate students of the Department of Pediatric Dentistry. The competencies were developed through the Delphi technique and consist of 47 items, 15 of which are on the cognitive dimension, 21 on the skills dimension, and 11 on the attitudinal dimension.
Discussion
This study focuses on the fundamental competencies that postgraduate students should possess to offer quality services to patients without compromising social accountability. The focus is most certainly on enhancing the quality of education and training, which requires developing an integrated course to fill the educational gaps [30].
A modified Delphi technique has been employed to increase the likelihood of reaching a consensus in competency identification in medical education. It comprises deliberate and progressive interactions of a specific group of specialists, and the consensus is reached through a set of systematic, interactive procedures whereby each participant can change their view and include new ones if needed [31].
This study constitutes the first attempt to define all necessary competencies for postgraduate students of pediatric dentistry curricula. The Delphi method was applied, and as a result, the panel of 25 experts agreed on 47 competencies arranged in three specific areas. These competencies will be the first step toward formulating a competencies-based program focusing on pediatric dentistry. The list incorporates important knowledge and competencies that cover general and behavior management concepts related to pediatric dentistry. It also touches upon general pediatrics and its sub-specialties, dealing with medically compromised and children with special needs, management of pain, oral medicine and surgery, techniques of sedation and general anesthesia, dental materials, interceptive orthodontics, pharmacology, epidemiology, prevention, restorative dentistry, dental trauma, research design, statistics, dental and maxillofacial radiology. Besides, the set includes the duties that the practitioners will perform. They must perform routine diagnostic and therapeutic measures, care for patients and their feelings and needs, and build trust. Dedication to self-evolution, patient safety and confidentiality, adherence to legal procedures, and obtaining informed consent are crucial aspects of a dentist's professional duty.
The optimal size of experts participating in Delphi studies varies and ranges from 5 to more than 1000 participants [32]. Loo emphasized that the purposeful selection of experts yields consensual data rather than large, randomly selected numbers [33].
A systematic review determined that most Delphi studies included ≥ 25 participants [32]. Only seven experts were included in the Delphi study by Dalkey and Helmer [34]. In comparison, this study included 25 pediatric dentistry experts with a response rate of 73.5%.
Answers were recorded using a five-point Likert scale, including a neutral point. Eliminating the neutral point may prompt respondents to adopt a clearer stance. However, its deletion results in a distortion in the responses toward negative responses, particularly in the case of ambivalent respondents [35].
This study employed two research methodologies. First, a focus group method was used to create an initial list of competencies. Second, the Delphi technique was used to restructure and develop a list of core competencies based on recommendations from previous studies [36].
The knowledge competency with the highest score was "construct effective and appropriate preventive plans for children with dental caries." This is crucial due to the significance of preventive strategies in halting caries development in children. Traditional pediatric dentistry residency program curricula have excessively emphasized restorative dentistry while neglecting early diagnosis and preventive management. This has contributed to a concerning increase in detected, missing, and filled teeth (DMFT) indicators in recent epidemiological studies conducted in Syria [37].
It is important to emphasize that preventive dentistry constitutes the most essential component of training in pediatric dentistry, as prevention is the foundation of the specialty. Previous studies have reported similar findings, highlighting that most universities in Brazil and Malaysia emphasize the knowledge and application of preventive materials in undergraduate dental education [38, 39]. The highest score regarding skill competencies was "critically appraise biomedical research and clinical research papers." Maintaining competency and continuing professional development are essential to providing up-to-date, high-quality patient care.
The postgraduate students will be able to confidently take responsibility for pediatric problems regarding evidence-based practice. They need to be equipped to research, select, analyze critically, and apply valid information based on evidence to sustain lifelong learning. Research studies in Chile and Latin America have supported the scientific basis that teaching and professional development involve research. These studies have also emphasized a need for more support, encouragement, and promotion of research culture within dental schools [40]. A study assessing the educational program given to postgraduate students in pediatric dentistry in Egypt revealed areas for improvement regarding scientific research. This was attributed to a need for more sufficient attention paid by faculty members to research and the lack of financial resources as significant obstacles to postgraduate research [41]. The data indicated that "compliance with infection control practices" was the most important attitude competency. This competency is crucial because infection control protects patients and healthcare workers, including pediatric dentists. Dentists work in an environment characterized by close contact with patients and the production of aerosols; therefore, the chances of infection transmission from an infected patient are very high. Thus, pediatric dentists should be informed and educated on the absolute adherence to infection control.
A recent review of emerging viral diseases in the new millennium concluded that infection control is as important in dental practice as understanding oral manifestations and diagnosing and managing viral infections [42]. Another important benefit of this study would be to aid the curriculum planners in making a
pediatric dentistry curriculum comprising a prioritized list of competencies established by experts.
There are several limitations of the Delphi survey. First, the repetitiveness of the survey set may easily cause a loss of interest in the participants over time, hence putting pressure on the study supervisors to keep the participants' motivation going after every round. Secondly, targeted postgraduate students participating in the study did not contribute to developing these competencies and thus may not be reflected in the identified competencies. Therefore, a comprehensive review of the pediatric dentistry curriculum is required to create appropriate structured curricular guidelines that answer the needs of learners and the community. These guidelines should standardize the content of undergraduate pediatric dentistry curricula in keeping with contemporary evidence-based dentistry, recommend the most effective educational methodology for delivering this content, and suggest the most appropriate assessment tools in light of the need to adopt a competency-based approach.
Conclusion
Forty-seven competencies have been identified that are expected to facilitate pediatric dentists' providing the highest quality patient health care. These competencies will also contribute to decision-makers developing more focused educational curricula that can dramatically enhance the evolution of competency-based education in pediatric dentistry.
Ethical considerations
This study got the Ethical Committee's approval, Damascus University, No. 482, on 04/02/2024, and it was mentioned in the introductory paragraph that this is an informed consent while filling out the electronic survey form.
Artificial intelligence utilization for article writing
Grammarly was used to correct grammar, punctuation, spelling, and paraphrasing in a critical review according to the ethical code.
Acknowledgment
The authors would like to thank all participating students and everyone who provided comments and suggestions that improved this study.
Conflict of interest statement
The authors confirm that they have no conflicting financial interests or personal relationships that could bias the work reported in this paper.
Author contributions
FB and MS collected the focus group data and employed the Delphi technique. MD oversaw the study's design and execution. FB and MD contributed to data analysis, interpretation, and manuscript drafting and reviewed the manuscript before submission. All authors have reviewed and approved the final manuscript.
Funding
Damascus University, Syria, supports this study.
Data availability statement
Data are available upon reasonable request. They are stored as de-identified participant data, which are available upon request to babakrdfarah@gmail.com.
Article Type : Orginal Research |
Subject:
Medical Education
Received: 2024/08/23 | Accepted: 2025/02/5 | Published: 2025/04/14
Received: 2024/08/23 | Accepted: 2025/02/5 | Published: 2025/04/14
References
1. Reyes Alardo LV, Palmer LB, Beach A, García‐Godoy F. Perceptions of dental students, dental faculty, practicing dentists and industry dental professionals on the acquisition of dental competencies and clinical skills in the Dominican Republic. European Journal of Dental Education. 2023;27(4):974-984. [DOI]
2. Khanna R, Lele G, Anandakrishna L, et al. Development of a competency-based curriculum for undergraduate education in pediatric dentistry: a systematic approach. Medical Journal Armed Forces India. 2021;77(1):22-30. [DOI]
3. Badran IG. Knowledge, attitude and practice the three pillars of excellence and wisdom: a place in the medical profession. EMHJ-Eastern Mediterranean Health Journal. [Online]. Available from: [Accessed: 1995]. [DOI]
4. Boateng SD, Ankrah DA, Manteaw, SA. Competence-based education: reflections on the context of teaching agriculture in Ghana’s pre-tertiary schools. Cogent Education. 2023;10(1):220-7793. [DOI]
5. Dashash, M. Identifying and assessing competencies for an entry level graduate in the faculty of dentistry, Damascus university: approaches, lessons learned and evidence provided. International Journal of Current Medical and Pharmaceutical Research. [Online]. Available from: [Accessed: Aug. 6, 2016]. [DOI]
6. Neumann LM, Nix JA. Trends in dental specialty education and practice, 1990‐99. Journal of Dental Education. [Online]. Available from: [Accessed: Dec. 1, 2002]. [DOI]
7. Boyd MA, Gerrow JD, Chambers DW, Henderson B J. Competencies for dental licensure in Canada. Journal of Dental Education. [Online]. Available from: [Accessed: Oct. 1, 2006]. [DOI]
8. Casamassimo PS, Townsend JA. The importance of pediatric dentistry. In Pediatric Dentistry 2019;4(2):2-7. [DOI]
9. Shah S. Paediatric dentistry-novel evolvement. Annals of Medicine and Surgery. 2018;25(1):21–29. [DOI]
10. Poulsen S, Koch G, Espelid I, Haubek D. Pediatric oral health and pediatric dentistry: the perspectives. pediatric dentistry: a clinical approach. [Online]. Available from: [Accessed: Apr. 26, 2016]. [DOI]
11. Kayyal M, Dashash M. The participatory approach in the reform of academic curricula–case study of the faculty of dentistry at Damascus university–Syria. Towards an Arab Higher Education Space: International Challenges and Societal Responsibilities. [Online]. Available from: [Accessed: Feb. 25, 2010]. [DOI]
12. Rashwan N, Mahmoud MR. Application of competency-based education in dentistry. International Journal of Dental Sciences and Research. 2021;9(2):23-26 [DOI]
13. Maart RD, Adam, RZ, Frantz JM. Strategies to implement competencies as it relates to a competency framework in a dental undergraduate curriculum: a systematic review. European Journal of Dental Education. 2023;27(3):746-755. [DOI]
14. Dashash M. Community-oriented medical education: bringing perspectives to curriculum planners in Damascus university. Education for Health. 2013;26(2):130-132. [DOI]
15. Dashash M, Youssef M. Dental education in Damascus university: a critical analysis and a suggested road map for accreditation. Edulearn10 proceedings. [Online]. Available from: [Accessed: Jul. 7, 2010]. [DOI]
16. Leung WC. Competency based medical training. British Medical Journal. 2002;325(7366):693. [DOI]
17. Thirawat J. Survey of opinions on competencies standard in dentistry for new dental graduates. Chulalongkorn University Dental Journal. 2007;30(3):287-302. [DOI]
18. Barrios M, Guilera G, Nuño L, Gómez-Benito J. Consensus in the Delphi method: what makes a decision change? Technological Forecasting and Social Change. 2021;163(3):120484. [DOI]
19. Olsen AA, Wolcott MD, Haines ST, Janke KK, McLaughlin JE. How to use the Delphi method to aid in decision making and build consensus in pharmacy education. Currents in Pharmacy Teaching and Learning. 2021;13(10):13761385 [DOI]
20. Abdel-Basset M, Mohamed M, Sangaiah, AK. Neutrosophic AHP-Delphi group decision making model based on trapezoidal neutrosophic numbers. Journal of Ambient Intelligence and Humanized Computing. 2018;9(1):1427-1443. [DOI]
21. Goodarzi Z, Abbasi E, Farhadian H. Achieving consensus deal with methodological issues in the Delphi technique. International Journal of Agricultural Management and Development. [Online]. Available from: [Accessed: Feb. 25, 2017]. [DOI]
22. Avella JR. Delphi panels: research design, procedures, advantages, and challenges. International Journal of Doctoral Studies. 2016;11(1):305-321. [DOI]
23. Guan LI, Gao P, Liu S, et al. Development of a global health bachelor curriculum in China: a Delphi study. British Medical Journal. 2019;9(1):e023893. [DOI]
24. Dashash M, Almasri B, Takaleh E, Abou Halawah A, Sahyouni A. Educational perspective for the identification of essential competencies required for approaching patients with covid-19. Eastern Mediterranean Health Journal. 2020;26(9):1011-1017 [DOI]
25. Zoukar I, Dashash M. Using a modified delphi method for identifying competencies in a Syrian undergraduate neonatology curriculum. Maternal and Child Health Journal. 2023;27(11):1921-1929. [DOI]
26. Shaheen M, Al-Nerabieah Z, Dashash M. A framework for the identification of competencies required from Syrian pulmonologists during covid-19 pandemic. Pneumologia. 2024;71(4):181-187. [DOI]
27. Jünger S, Payne SA, Brine J, Radbruch L, Brearley SG. Guidance on conducting and reporting Delphi studies (CREDES) in palliative care: recommendations based on a methodological systematic review. Palliative Medicine. 2017;31(8):684-706. [DOI]
28. Shah S. Paediatric dentistry-novel evolvement. Annals of Medicine and Surgery. 2018;25(1): 21-29. [DOI]
29. Ab Latif R, Dahlan A, Mulud Z A, Nor ZM. The Delphi technique as a method to obtain consensus in health care education research. Education in Medicine Journal. 2017; 9(3):89-102. [DOI]
30. Agouropoulos A, Seymen F, Kupietzky A, Bönecker M. Global overview on current paediatric dentistry teaching: a survey of national member societies of the IAPD. International Journal of Paediatric Dentistry. 2024;34(1):58-65 [DOI]
31. McElroy L, Robinson L, Battle C, et al. Use of a modified Delphi process to develop research priorities in major trauma. European Journal of Trauma and Emergency Surgery. 2022;48(2):1453–1461. [DOI]
32. Diamond IR, Grant RC, Feldman BM, et al. Defining consensus: a systematic review recommends methodologic criteria for reporting of Delphi studies. Journal of Clinical Epidemiology. 2014; 67(4):401-409. [DOI]
33. Loo R. The Delphi method: a powerful tool for strategic management. Policing: An International Journal of Police Strategies & Management. 2002;25(4):762-769 [DOI]
34. O’Mahony D, O’Sullivan D, Byrne S, O’Connor MN, Ryan C, Gallagher P. STOPP/START criteria for potentially inappropriate prescribing in older people: version 2. Age and Ageing. 2014;44(2):213-218. [DOI]
35. Drumm, S, Bradley C, Moriarty F. ‘More of an art than a science’? The development, design and mechanics of the Delphi technique. Research in Social and Administrative Pharmacy. 2022;18(1):2230–2236. [DOI]
36. Khiami A, Dashash M. Identification of the role of oral health educators in elementary schools during covid-19 pandemic: a competency framework. BMC Research Notes. 2022;15(1):1-8. [DOI]
37. Ballouk MA, Dashash M. Caries prevalence and dental health of 8–12 year-old children in Damascus city in Syria during the Syrian crisis; a cross-sectional epidemiological oral health survey. BMC Oral Health. 2019;19(1):1-6. [DOI]
38. Da Costa VS, Wanderley MT, Haddad AE, et al. Currículo de odontopediatria nos cursos brasileiros de graduação em Odontologia. Revista Da ABENO. 2020;20(2):93-101. [DOI]
39. Lin GS, ChinYJ, Chong RS, et al. Expert consensus on relevant topics for undergraduate paediatric dental curriculum using the fuzzy Delphi method: a new direction for Malaysian dental education. BMC Oral Health. 2023;23(1):452. [DOI]
40. Mariño R, Ramos-Gómez F, Manton DJ, et al. The future of pediatric dentistry education and curricula: a Chilean perspective. BMC Oral Health. 2017;17(2):1–7. [DOI]
41. Yassa MK, Khattab NM. Assessment of advanced paediatric dentistry education programmes in Egypt: a survey of programme directors. BMC Medical Education. 2024;24(1):196. [DOI]
42. Al-Nerabiah Z, Alkhouli M, Laflouf M, Abdul-Hak M. Pediatric dentists consideration for covid-19 in children. International Journal of Applied Dental Sciences. [Online]. Available from: [Accessed: Mar. 3, 2020]. [DOI]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
